
Abstract
Objectives
To evaluate periprosthetic bone mineral density (BMD) changes around a cementless short tapered-wedge stem and determine correlations between BMD changes and various clinical factors, including daily activity, after total hip arthroplasty (THA) with a tapered-wedge stem.
Methods
65 patients underwent THA with a TriLock BPS stem. At baseline and at 6, 12, and 24 months postoperatively the BMD of the 7 Gruen zones were evaluated using dual-energy x-ray absorptiometry. Correlations were determined between BMD changes and clinical factors, including the Harris Hip Score, body mass index, University of California at Los Angeles (UCLA) activity rating score, age at surgery, and initial spine BMD. Radiographic parameters, including the proximal femoral geometry (Dorr Classification), canal filling ratio, canal flare index, and calcar-to-canal ratio were also assessed.
Results
Minimal BMD changes were noted in the distal femur. However, significant BMD loss was noted in zone 7 at each time point. BMD loss was also noted in zone 1 at 6 and 12 months postoperatively, but BMD recovered after 18 months. Significant positive correlations were noted between BMD changes and the UCLA activity score in zones 1, 6, and 7. Additionally, negative correlations were noted between BMD changes and the preoperative lumbar BMD in zones 2 and 3. No correlations were noted between BMD changes and the radiographic parameters. Periprosthetic BMD was was virtually unchanged in the proximal femur, especially Gruen zone 1.
Conclusions
Daily activity may reflect improvements in periprosthetic bone quality after THA; however, the use of this tapered-wedge stem is not recommended in patients with poor bone quality.
Introduction
Under normal physiological conditions, the femoral head, neck, and femur bear mechanical stresses. Once a total hip arthroplasty (THA) has been implanted, mechanical loading in daily life activities is taken up by the implanted stem and femoral bone around and below the stem. The characteristics of both the stem and bone around and below the implant are different. The stem is stiffer than bone and can as a result cause stress shielding of bone (1, 2). Other factors can be involved in stress sharing and consequently stress shielding, and these factors will be reflected in the bone mineral density (BMD) values (3). Dual-energy x-ray absorptiometry (DEXA) is a well reported and sensitive means of assessing BMD and bone remodelling/adaptation following THA (4–5–6–7–8). A study of 33 patients reported that periprosthetic BMD loss was consistently less with a triple tapered stem than with a straight type stem (9).
The TriLock BPS stem (Depuy, Warsaw, IN) is a short tapered-wedge stem with a reduced shoulder shape, thin anterior-posterior width, and reduced length. It is a blade-style stem that obtains rotational stability in a typical ovoid femoral canal. The length variations of the component range from 114.5 mm to 140 mm, and the stem is made from titanium-alloy (Ti-6Al-4V) with a grit blasted surface. The distal portion of the stem has a longitudinal flute on the anterior aspect and posterior aspect that is grit blasted for on-growth to allow fluid/debris to exit the medulla. Short bone preserving cementless stems have become more popular having been marketed as ‘bone preserving’. In theory this would be expected to improve proximal load transfer and decrease stress shielding (10, 11).
The purpose of this study was to evaluate periprosthetic BMD changes around a cementless short tapered-wedge stem and determined the correlations between periprosthetic BMD changes and various clinical factors, including daily activity, in patients who underwent THA.
Methods
This was a prospective cohort study of patients (65 joints).. Inclusion criteria were patients with osteoarthritis (Tönnis grade 4) and those who underwent THA with a TriLock BPS stem at our institution between April 2012 and March 2013. The femoral canal was prepared using a custom broach that precisely replicated the shape of the prosthesis. Patients with distorted proximal femoral anatomy, osteoporosis (lumbar spine BMD >0.8), or evidence of metabolic bone disease were excluded. All procedures were performed at Kobe University Hospital. Full weight-bearing with a walker or T-cane was started the next day postoperatively, and patients stayed in the hospital for 2 weeks.
DEXA was performed in all cases using a DPX-L scanner (GE-Lunar Corp., Madison, WI). DPX-L total-body scans were performed using software version 1.35, which determined an appropriate transverse speed of 16, 8, or 4 cm/sec based on the subjects’ size BMD was determined in 7 regions of interest based on the Gruen zones (12), and preoperative lumbar BMD was also determined. The values were expressed in g/cm2. Baseline BMD around the stem was assessed within 2 months postoperatively. BMD ratios were calculated by dividing each BMD value at 6, 12, and 24 months postoperatively by the BMD value within 2 months postoperatively and multiplying the quotient by 100.
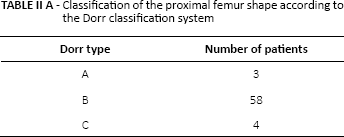
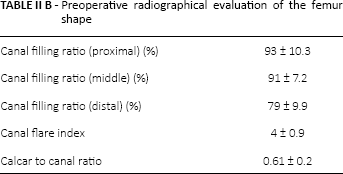
Postoperative follow-up included evaluation with DEXA, and secondary outcome measures including the Harris Hip Score (HHS) and University of California at Los Angeles (UCLA) activity rating score. Age at surgery and body mass index (BMI) was also recorded. Preoperative radiographic evaluation of the proxima femur was undertaken using the Dorr classification (Tab. IIB). in addition to the ratio of canal filling (13), canal flare index (14), and calcar-to-canal ratio (15). These parameters can influence the final position of the femoral stem and thus affect new stress patterns in the proximal femur resulting in changes to periprosthetic bone quantity. The ratio of canal filling was defined as the ratio of the width of the stem over the width of the femoral canal at the following 3 sections: (i) proximal (15 mm above the lesser trochanter), (ii) middle (60 mm below the lesser trochanter), and (iii) distal (15 mm above the tip of the stem).
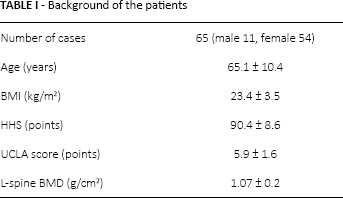
Background of the patients
Classification of the proximal femur shape according to the Dorr classification system
All data are expressed as mean ± standard deviation unless otherwise indicated. Statistical analysis was performed using one-way analysis of variance, with Tukey's post hoc test for multiple comparisons of paired samples. The Mann-Whitney U test was used for comparisons between the two groups. Correlations between periprosthetic BMD changes and clinical factors, including the HHS, BMI, UCLA activity rating score, age at surgery, and preoperative lumbar BMD, were evaluated using Pearson's chi-square test. A p-value of <0.05 was considered significant.
Preoperative radiographical evaluation of the femur shape
Results
Clinical and radiographic evaluation
Clinical evaluation was performed at 24 months postoperatively. The mean HHS of the patients was 90.4 ± 8.6, BMI was 23.4 ± 3.5 kg/m2, and UCLA activity rating score was 5.9 ± 1.6. The mean age at surgery was 65.1 ± 10.4 years (Tab. I). There was no case of stem subsidence. Postoperative BMD changes were analysed for each Dorr femoral bone classification. No significant differences of BMD changes among Dorr types were found. The average canal filling ratios were 93 ± 10.3% at the proximal, 91 ± 7.2% at the middle, and 79 ± 9.9% at the distal levels respectively. The average canal flare index was 4.0 ± 0.9, and the value was within normal range (normal: 3.0< canal flare index <4.7). The average calcar-to-canal ratio was 0.61 ± 0.2.
Periprosthetic BMD changes
The mean BMD of the lumbar spine at surgery was 1.07 ± 0.2 g/cm2 (Tab. I). Minimal BMD changes were noted in the distal femur (Gruen zones 3, 4, and 5), and BMD ratios at 24 months postoperatively were: zone 3, 103%; zone 4, 99%; and zone 5, 101% (Fig. 1). Significant BMD loss was noted in the proximal femur at zone 7 at each time point. Additionally, BMD loss was noted in zone 1 at 6 and 12 months postoperatively, but BMD recovered after 18 months. BMD ratios in the proximal femur at 24 months postoperatively were: zone 1, 97%; zone 2, 100%; zone 6, 97%; and zone 7, 85% (Fig. 1).
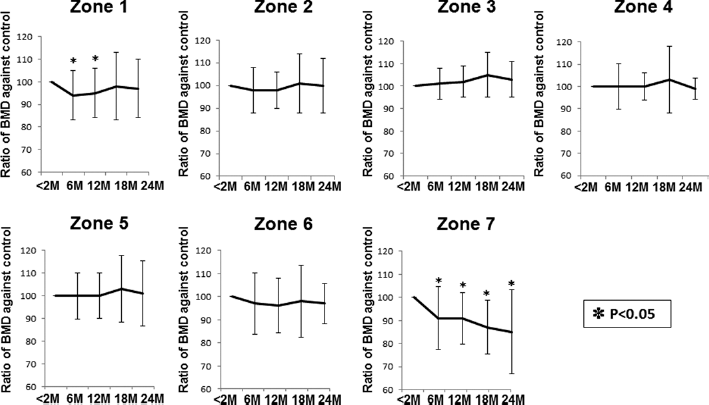
Bone mineral density changes (%) at 6, 12, and 24 months postoperatively in the 7 Gruen zones. The columns represent mean ± standard deviation. * indicates p<0.05 compared with the baseline bone mineral density.
Correlations between periprosthetic BMD changes and clinical factors
No correlations were noted between BMD changes and the HHS, BMI, or age at surgery (Tab. III). However, significant positive correlations were noted between proximal BMD changes and the UCLA activity rating score, and the correlation coefficients were 0.31 for zone 1 (p = 0.031), 0.351 for zone 6 (p = 0.017), and 0.348 for zone 7 (p = 0.017). Surprisingly, we noted negative correlations between proximal BMD changes and initial lumbar spine BMD, and the correlation coefficients were -0.488 for zone 2 (p = 0.001) and -0.460 for zone 3 (p = 0.002) (Tab. III).
Correlations between the periprosthetic bone mineral density changes and clinical factors (i.e., the Harris Hip Score, body mass index, University of California at Los Angeles activity rating score, age at surgery, and initial lumbar bone mineral density) in the 7 Gruen zones at 24 months postoperatively
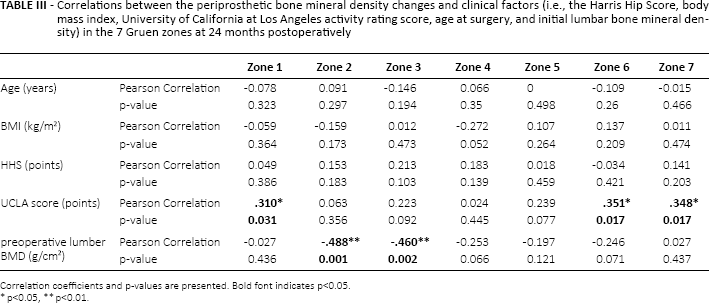
Correlation coefficients and p-values are presented. Bold font indicates p<0.05.
p<0.05,
p<0.01.
Correlations between periprosthetic BMD changes and radiographic parameters
We tested the correlation between periprosthetic BMD changes and the characteristics of the proximal femur. However, no correlations were noted between BMD changes and the canal filling ratio, canal flare index, or calcar-to-canal ratio in all periprosthetic zones (Tab. IV).
Correlations between the periprosthetic bone mineral density changes and clinical parameters (i.e., the canal filling ratio, canal flare index, or calcar-to-canal ratio) in the 7 Gruen zones at 24 months postoperatively
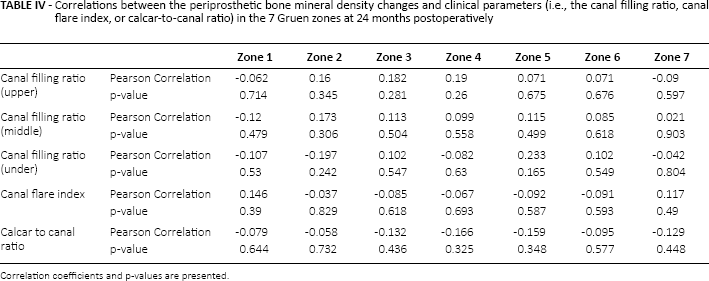
Correlation coefficients and p-values are presented.
Discussion
The study found that periprosthetic BMD remained virtually unchanged in the proximal femur, especially Gruen zone 1 after THA. Additionally, the study identified significant positive correlations between BMD changes and the UCLA activity rating score in Gruen zones 1, 6, and 7, and negative correlations between BMD changes and the preoperative lumbar spine BMD in Gruen zones 2 and 3.
Several reports have demonstrated periprosthetic BMD loss in Gruen zone 7 (16–17–18–19). Venesmaa et al (16) reported that periprosthetic BMD loss in Gruen zone 7 was 22.9% with a porous-coated Biometric stem (Biomet, Inc., Warsaw, IN, USA) at the end of the first year. van der Wal et al reported that periprosthetic BMD loss at anatomical contours of the proximal femur in all 3 dimensions in Gruen zone 7 was 11.9% (17) with an ABG-1 stem (Stryker-Howmedica, Kalamazoo, MI) at the end of 2 years, and BMD loss in Gruen zone 1 was 9.3% (18). Alm et al (19) reported that periprosthetic BMD loss of the proximal femur in Gruen zone 7 was 23% with an ABG-2 stem (the same concept as ABG-1) at the end of 2 years. In the present study, proximal lateral BMD (Gruen zones 1 and 2) was almost maintained with a short tapered-wedge stem. However, the proximal medial BMD loss (Gruen zone 7) was 15%. These results are consistent with those of other reports (16–17–18–19–20). We have previously shown that periprosthetic BMD loss was 3% in zone 1 and 14% in zone 7 (G2 stem), and 19% in zone 1 and 20% in zone 7 (VerSys FMT) at the end of 2 years (9). The results of the triple-tapered G2 stem were similar to those of the short tapered stem in the present study, but the results were much better than those of the straight tapered VerSys FMT stem. These findings suggest that proximal loading is a feature of a short tapered stem. Several studies have measured baseline BMD within 6 weeks (20, 21). Sabo et al (21) reported that slight periprosthetic BMD loss occurred at 3 months postoperatively. In the present study, baseline BMD was determined within 1 month in most patients.
Restricted mobility was associated with a low risk of stem loosening for cemented stems (22, 23). Flugsrud et al (24) reported that high physical activity increased the risk of early revision hip arthroplasty, whereas Wroblewski et al (25) reported that the C-stem was designed for proximal fixation, and can maintain bone quality and prevent stress shielding with proximal loading. Therefore, bone quality can be reasonably maintained in young, active patients with good-quality bone and good hip function. We previously reported significant positive correlations between periprosthetic BMD changes and the UCLA activity rating score in Gruen zones 1 and 2 with a triple-tapered stem (26). In the present study, we demonstrated that periprosthetic BMD in Gruen zones 1 and 7 was associated with daily activity. Our findings suggest that daily activity may contribute to proximal loading and early femoral stem fixation with a short-tapered stem.
Nixon et al (27) reported that low lumbar BMD was a predictive factor for stem loosening. Alm et al (19) reported that patients with low lumbar BMD were prone to periprosthetic BMD loss in Gruen zone 7. We demonstrated significant negative correlations between periprosthetic BMD changes and preoperative lumbar BMD in Gruen zones 2 and 3. These findings suggest that distal loading may occur with a short-tapered stem in patients with low bone quality, and this distal femur loading is not a feature of a short-tapered stem. Therefore, patients with low bone quality are not good candidates for the use of a short-tapered stem.
In the present study, no correlations were noted between periprosthetic BMD changes and BMI or age at surgery. However, several reports have demonstrated correlations between periprosthetic BMD changes and the HHS, BMI, and age at surgery (28–29–30–31). These differences may be dependent on a feature of the short-tapered stem.
The factors contributing to stem loosening are multi-factorial. One factor is the reduced tolerance of the femur to mismatch in shape between the femoral stem and the canal due to lower BMD (15), and insufficient canal filling may lead to thigh pain, stem loosening, or implant failure (32, 33). We demonstrated that the proximal canal filling ratios were 93% at the proximal level and 79% at the distal level. These results were in line with those of a previous study on another tapered-wedge stem (34), and a higher canal filling ratio at the proximal site suggest that proximal loading is a feature of a short-tapered stem. A shape mismatch between cementless stems and the femoral canal of very elderly patients can partly explain this.
Boymans et al (35) reported that canal flaring changed asymmetrically with increased medial and less lateral flaring in elderly subjects. They further demonstrated that the average value of the canal flare index was significantly lower in elderly female subjects, and these age-related changes should be considered for implant design, selection, and implantation. Therefore, we analysed the canal flare index and calcar-to-canal ratio, and both parameters were almost normal compared with that given in previous reports (15, 35). Furthermore, we analysed correlations between periprosthetic BMD changes and the canal filling ratio, canal flare index, and calcar-to-canal ratio, but we did not find any correlations. The shape of the proximal femur of most subjects in this study was classified as Dorr type B, and the canal flare index/calcar-to-canal ratio was relatively normal. These findings may lead to a higher canal filling ratio at the proximal site, and they may explain why there was no correlation between periprosthetic BMD changes and the radiographic parameters.
Regarding the limitation of this study, the periprosthetic DEXA analysis has some precision errors. Cohen et al (36) reported a mean precision error of 2.7%-3.4%. The most significant factor affecting reproducibility was rotation of the femur. Therefore, we used knee and foot support to control leg rotation during scanning in the anterior-posterior projection, and we believe that DEXA is a precise method of measuring small changes in BMD around femoral implants.
In conclusion, periprosthetic BMD was remained virtually unchanged 24 months post surgery. Daily activity may reflect improvements in periprosthetic bone quality after THA with a short-tapered stem; however, this stem is not recommended in patients with low bone quality.
Footnotes
Financial support: None.
Conflict of interest: None.