
Abstract
Purpose
The purpose of this study was to evaluate whether the ipsilateral knee alignment secondary to knee osteoarthritis affect positioning of the femoral component anteversion during total hip arthroplasty.
Methods
Preoperative and postoperative computed tomography-based 3-D femoral models were reconstructed for 20 total hip arthroplasty patients. Prosthetic femoral stem and native femoral anteversion was measured and compared.
Results
An average increase by 4.5° ± 8.1° in femoral anteversion was found following total hip arthroplasty (p = 0.02). Strong positive correlation was found between the knee varus angle and the changes in femoral anteversion (R = 0.87, p<0.0001). The knee alignment was an independent factor for predicting the intraoperative positioning of femoral stem anteversion.
Conclusions
The ipsilateral knee varus deformity should be considered to optimise the femoral component position during contemporary total hip arthroplasty.
Introduction
The prevalence of ipsilateral symptomatic hip and knee osteoarthritis (OA) has been estimated to be 11% in adults over 65 years of age (1). Total hip arthroplasty (THA) is the surgical treatment for advanced hip OA with satisfactory long-term outcomes (2). Optimal component placement is one of the prerequisites for a successful THA, as component malposition is related to aseptic loosening, impingement, dislocation and eventually, implant failure (3). The recommended position of the femoral component is to restore native anteversion in the absence of severe deformity (4, 5). However, several studies have reported that THA does not restore native anteversion (6, 7).
Previous studies have reported significant differences between intraoperative and postoperative femoral component anteversion, ranging from 1° to 25° (8, 9). These studies suggested that the limited osseous landmarks available and the inability to estimate the femoral diaphyseal bow and anteroposterior canal isthmus, were the possible reasons for the observed differences (8). A recent study also showed that knee OA could increase surgical error in estimating femoral stem anteversion when the posterior approach was used in THA (10). Interestingly, the femoral component anteversion is commonly measured intra-operatively as the angle between the lower leg axis and the femoral trial stem axis by placing the tibia in a vertical position (8, 10). This technique assumes that the position of the tibia is perpendicular to the floor with neutral rotation of the femur, especially during the posterior approach. Since lower limb axis and knee alignment are associated with the ipsilateral knee OA (11), varus malalignment of the knee might affect the surgeon's ability to reliably reproduce femoral stem anteversion. Up to date, the potential effect of the ipsilateral knee alignment on femoral stem anteversion in primary total hip arthroplasty has not been reported.
The purpose of this study was to quantify the differences between preoperative native femoral anteversion and postoperative femoral stem anteversion, and to determine whether the knee alignment affected these differences. We hypothesised that ipsilateral varus knee alignment, secondary to knee OA, would influence the intraoperative positioning of femoral stem anteversion in THA patients.
Methods
The study was approved by the institutional review board and informed consent was obtained from all patients prior to participation. All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patients
20 patients (11 males, 9 females) who underwent unilateral THA for end-stage non-traumatic hip OA enrolled in this study. All patients received cementless THA with cementless acetabular cup, highly cross-linked polyethylene, collarless tapered wedge cementless femoral stem (Linear stem; DJO Global, Vista, CA, USA) and cobalt-chromium femoral head by a single surgeon, using a posterior approach. The preparation was started on the femoral side, according to the combined anteversion technique. The final stem was the largest stem that could fit into the femoral canal and was adjusted, as possible, to follow the preoperative native anteversion. With the trial stem in place, stem anteversion was measured as the angle between the lower leg axis and the femoral trial stem axis by placing the tibia in a vertical position. Acetabular cup and femoral head diameter ranged from 50-56 mm and 32-40 mm, respectively. The patient's demographic data were age 62.4 ± 8.4 years (range 47-71 years), height 167.7 ± 7.4 cm (range 155-183 cm), weight 76.6 ± 19.6 kg (range 49-118 kg), and BMI 27.0 ± 5.6 kg/m2 (range 18.6-37.3 kg/m2). The average follow-up period was 12.4 ± 4.6 months (range 6.8-22.6 months). 10 patients had their left hip replaced while 10 patients had their right hip replaced. Inclusion criteria were no history of surgical complication, dislocation or component subluxation.
Ipsilateral knee anatomical alignment
The anteriorposterior scout views of a supine CT scan of the entire lower limb were used to measured the anatomical angle of the ipsilateral knee radiographs (positive value for varus and negative value for valgus alignments). Identical CT protocol with both legs stabilised in a neutral position without any rotation was applied to all patients. We defined the anatomical axes of the distal femur and proximal tibia using an angle subtended by the line of the femoral shaft as it intersects in the knee with the line of the tibia shaft.
Grades of ipsilateral knee OA
On the preoperative computed tomographic (CT) images and scout films, the degree of knee OA was classified into four grades adopting Kellgren-Lawrence classification (12). Briefly, grade 1: doubtful joint space narrowing and possible osteophytes; grade 2: definite osteophytes and possible joint space narrowing; grade 3: moderate osteophytes and definite joint space narrowing; grade 4: definite bone ends deformity.
Three-dimensional (3-D) femoral modelling
All patients received a computed tomography (CT) scan (Sensation 64, Siemens, Germany) in supine position, from the 5th lumbar vertebra to the mid-femur, with their legs in neutral position as confirmed by scout views. The images were acquired along the axial direction with slice thickness of 0.625 mm and an in-plane resolution of 0.3 mm × 0.3 mm. In accordance with previously validated and published study protocol, surface models were reconstructed in commercial software (Rhinoceros®, Robert McNeel and Associates, Seattle, WA, USA) and imported to a customised MATLAB program (The MathWorks Inc., Natick, MA, USA) for analyses (7, 12).
Femoral anteversion
The centre of femoral head was defined as the centre of the best-fit 3-D sphere of the surface of the femoral head (Fig. 1). The centre of femoral neck was defined as the centroid of best-fit ellipse at the isthmus level. Femoral anteversion was defined as the angle between the line connecting the centre of femoral head to the centre of femoral neck and the posterior condylar axis (the line connecting the most posterior aspect of the lateral and medial femoral condyles) projected on the transverse plane. The femoral anteversion differences were evaluated by calculating the difference between preoperative native femoral anteversion and postoperative prosthetic stem anteversion (anteversion difference = prosthetic anteversion - native anteversion). The other proximal femoral parameters such as neck-shaft angle, femoral horizontal and vertical offset, and head diameter were measured following the previously published protocol (7).
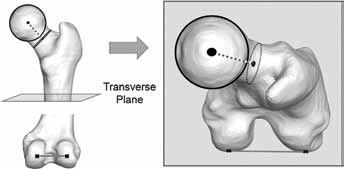
Femoral anteversion angles were measured on the reconstructed CT-based 3-D models. The anteversion angle was defined as the angle between the femoral neck axis of femoral neck and the posterior condylar axis. Femoral neck axis and posterior condyle axis were shown in dotted and solid line, respectively. • Centre of the femoral head; • Centre of femoral neck; × Margin of the posterior condyles. Dotted line = femoral neck axis; solid line connecting crosses = posterior condylar line.
Statistics
The distributions of the variables were examined in exploratory data analyses and all variables met the criteria for a normal distribution. Descriptive statistics of averages, standard deviations and ranges were applied. Paired t-test was used to compare the average values of native and prosthetic femoral anteversion. Simple linear regression analysis was used to investigate correlations between the knee OA grade and the femoral anteversion difference, while Pearson's correlation coefficient was reported to quantify the correlation between ipsilateral knee anatomical angle and the femoral anteversion difference following THA. Multiple linear regression analysis adjusted for age, gender, height and body mass index was performed to account for potential confounders. Statistical analyses were performed with SPSS software (version 22.0, SPSS, Chicago, IL, USA) and p value less than 0.05 was considered statistically significant.
Results
The average native and postoperative prosthetic anteversion were 14.4° ± 8.9° and 19.0° ± 9.4°, respectively (Tab. I). Femoral anteversion was increased by 4.5° ± 8.1° following THA (p = 0.02, Fig. 2). In 14 of 20 cases, the prosthetic femoral anteversion was increased compared to those of native femur whereas the femoral anteversion decreased in 6 cases after surgery. The distribution of knee OA grades among the patients was as follows: grade 1 in 5 cases; grade 2 in 7 cases; grade 3 in 4 cases; and grade 4 in 4 cases. The mean varus angle of the knees was 7.1° ± 6.5° (Tab. I). There was a strong positive correlation between knee OA grades and knee varus angle (R = 0.92, p<0.001).
The knee and proximal femoral parameters of the patients
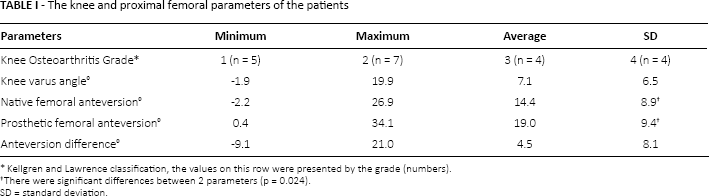
Kellgren and Lawrence classification, the values on this row were presented by the grade (numbers).
There were significant differences between 2 parameters (p = 0.024).
SD = standard deviation.

The femoral anteversion of native and prosthetic femur. Box length represents the interquartile range, the line in the centre of the box represents the median value, the bars represent the range, and the points represent the outliers.
There was a positive correlation between knee OA grades and femoral anteversion difference (R = 0.88, p<0.001). A strong positive correlation (R = 0.87, p<0.0001) was also found between knee varus angle and femoral anteversion differences (Fig. 3). An increase in the knee OA grade by 1 was found to be associated with a 6.6° increase in femoral stem anteversion (95% confidence interval [95% CI], 4.8° 8.5°). However, there was no statistically significant difference for all the other parameters including neck-shaft angle, femoral horizontal and vertical offset, native head diameter, and native femoral anteversion between knee OA grade groups (Tab. II). Multivariate analysis demonstrated that knee varus angle was an independent factor for predicting the femoral anteversion differences when the model was adjusted for potential confounders such as age, sex, body mass index, and knee OA grade (B = 1.167, 95% CI, 0.586-1.748, p = 0.001).
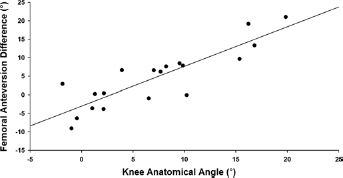
Correlation between knee alignment angle and femoral anteversion difference (R = 0.867, p<0.0001).
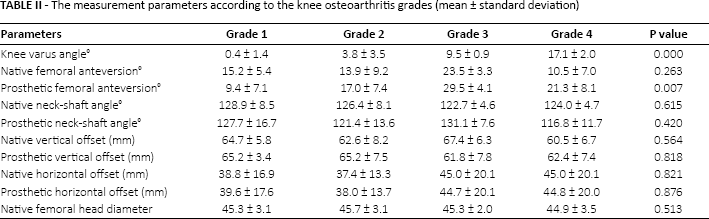
The measurement parameters according to the knee osteoarthritis grades (mean ± standard deviation)
Discussion
Based on the demographic changes in the population, it is projected that the incidence of ipsilateral knee and hip OA will increase dramatically over the coming years (14). Therefore, the number of patients with pre-existing ipsilateral knee OA requiring THA is expected to rise. This study used 3-D CT models to investigate whether ipsilateral knee alignment was correlated with the femoral anteversion change following THA. Significant increase of femoral anteversion was observed after THA (p = 0.02). Varus knee alignment, secondary to knee OA, had a strong positive correlation (R = 0.87, p<0.001) with the changes in femoral anteversion, suggesting that ipsilateral varus knee alignment could result in increased prosthetic femoral anteversion.
The surgeon's intraoperative estimation of femoral component anteversion has poor prediction and is often not within the recommended range for THA (9, 13). Combined anteversion in THA is the sum of the acetabular cup and femoral stem anteversion (14). The recommended safe zones to avoid dislocation in THA range from 25° 50° and 10° 20° for combined and femoral anteversion, respectively (8, 14–15–16). Dorr et al (8) reported that with cementless femoral stems, a wide range of femoral anteversion (-8.6° to 27.1°) was obtained even though an experienced surgeon intended to achieve ideal femoral anteversion. Wines et al reported that only 71% of femoral components were within the expected clinical anteversion range. Similarly, the current study showed a wide range of femoral component anteversion (0.4° 34.1°). There were significant differences between the native and prosthetic femoral anteversions, ranging from -9.1° to 21.0°. These data suggested that the intraoperative positioning of femoral stem anteversion is prone to significant variation.
Several factors have been reported to be associated with the increased femoral anteversion following THA. Emerson et al (6) suggested that the press-fit stems follow the proximal femur anatomy, leading to increased anteversion as the femoral canal is more anterverted at the level of the lower neck and intertrochanteric area. Dorr et al (8) suggested that surgeon's poor intraoperative estimation of femoral anteversion, in combination with the shape of the femoral canal may account for the wide range of stem anteversion. Wines et al (9) found that posterior approach resulted in more anteversion compared with the modified Hardinge lateral approach. Recently, Hirata et al (10) reported that knee OA affected the degree of surgeon error in estimating femoral stem anteversion in THA using a posterior approach.
The potential association between hip anatomy and knee OA using plain x-ray have been reported (17–18–19). Wise et al (17) found that medial compartment knee OA was associated with different ipsilateral proximal femur shapes. Boissonneault et al (18) demonstrated that medial knee OA was correlated with a more varus femoral neck and a decreased abductor angle. The different proximal femoral anatomy associated with knee OA could imply a potential correlation between knee OA and femoral component position found in our study. In the current study, several proximal femoral parameters such as neck-shaft angle, femoral horizontal and vertical offset, head diameter and native femoral anteversion, were analysed using 3-D CT hip models (Tab. II). We found no correlation between the knee OA grade and all the parameters measured in these patients group. This pre-existing proximal femoral anatomy was not found to affect the femoral stem positioning during surgery in this study.
We found that knee varus angle was an independent factor for predicting the femoral anteversion differences after adjustment for knee OA grade (B = 1.167, p = 0.001) suggesting the knee malalignment due to the ipsilateral knee OA needs to be taken into consideration when the posterior approach is used in THA. This could be, in part, due to the fact that the posterior approach for total hip arthroplasty usually uses the long axis of the lower leg as the reference for determination of femoral anteversion during surgery. It is assumed that the position of the tibia being perpendicular to the floor with neutral rotation of the femur in patients with normal knee alignment. However, the osteoarthritic knee with significant varus deformity may cause inaccuracy in the assumption. Patients with knee varus deformity would require more internal rotation of the lower leg until the long axis of tibia is vertical to the plane during THA (Fig. 4). This would result in an increased internal rotation of the posterior condyle line, by an angle similar to the knee anatomical angle, with subsequent increase of femoral stem anteversion (Fig. 4).
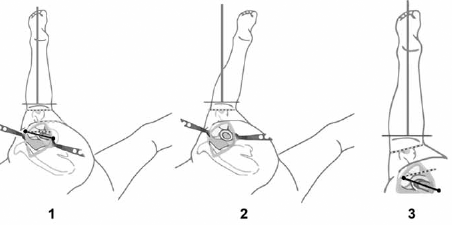
Long axis of the lower leg as the reference for determination of femoral anteversion during posterior approach in total hip arthroplasty. (
The results of this study need to be considered in light of the potential limitations. First, only posterior surgical approach was used in this study which uses the tibia as a reference for femoral positioning. Hence, the effect of other approaches on femoral anteversion could not be established. It should be noted that the stem rotation is often determined by native femoral neck anteversion while optimising stem-bone contact. Therefore, the results of our study are relevant when using vertical tibia axis to adjust for the femoral anteversion. Moreover, this study included only 1 femoral stem design. Although, this design is similar to other commonly used straight tapered implants available, our findings may not be generalised to other types of femoral stems. Another potential limitation is that knee varus angle may change between full extension, as measured in x-ray and 90° of flexion, as measured intraoperatively in patients without fixed varus deformity. Finally, the sample size was relatively small. However, statistically significant differences between native and prosthetic hip were observed.
In conclusion, this is 1 of the first studies to evaluate the potential effect of the ipsilateral knee alignment angle, secondary to knee OA, on the femoral stem positioning in THA. The results demonstrated that when using a posterior approach, varus malialignment of the ipsilateral knee is associated with greater anteversion of the femoral stem. Surgeons should consider the ipsilateral knee alignment to optimise the femoral component position during THA in the patients with severe knee OA.
Footnotes
Financial support: This study was partially funded by Mako Surgical Inc.
Conflict of interest: None.