
Abstract
Purpose
To compare the functional outcomes of patients undergoing arthroscopic surgery for the treatment of femoroacetabular impingement (FAI) performed with either the classic or the outside-in access to the hip.
Methods
Data regarding patients arthroscopically treated for FAI from January 2009 to June 2013 were retrospectively reviewed and compared regarding the type of access.
Results
101 hips (91 patients) with a minimum of 12 months follow-up (mean 22 months, range 12-40 months) were included. Classic access was used in 48 cases while outside-in access was performed in 53 cases. Mean age was 37 years (range 15.7-59.6 years). Both groups were comparable with respect to preoperative characteristics. Mean operating time was 162 minutes for the outside-in group and 172 minutes for the classic access group. Complications between both groups showed no statistically significant differences but for the presence of heterotopic calcifications, which was more frequently observed regarding the outside-in access. Outcomes measured by the modified Harris Hip Score showed no overall differences regarding both types of access, except for patients under 35 years old, where there was a statistically significant increase in excellent and good outcomes with the use of the classic access in comparison to the outside-in technique. Postoperative hip motion was also significantly higher in the classic access group.
Conclusions
No differences have been found in outcomes regardless the access used. Classic access seems to offer a higher postoperative range of motion and lower risk of heterotopic ossifications.
Introduction
Femoroacetabular impingement (FAI) is a well-known condition of the hip that has been associated with the early development of osteoarthritis (1). Hip arthroscopy has been shown to provide an adequate correction of FAI with fewer complications and shorter recovery times than conventional open surgery and at least matching those of mini-open surgery (2–3–4–5–6).
The classic arthroscopic access to the hip has been described by many authors (7, 8). By using this technique, the central compartment is accessed first under fluoroscopy (Fig. 1). Joint traction is required at this moment. A capsulotomy is performed to allow the instruments to move freely enough to complete the acetabuloplasty and labral repair (Fig. 2). To perform the femoroplasty, the peripheral compartment is accessed by extending the capsulotomy distally after releasing traction. Capsular closure can be achieved at the end. Good early and mid-term results have been reported regarding this technique for the treatment of FAI (9–10–11). Nevertheless, it remains technically demanding and is associated with long learning curves (12–13–14).

Fluoroscopic image of a classic arthroscopic access to the hip.
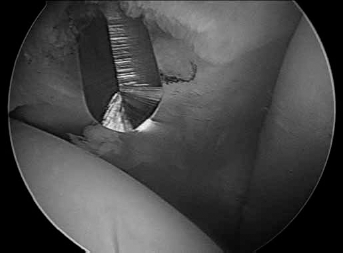
Arthroscopic view of capsulotomy regarding classic arthroscopic access to the hip.
For this reason, another arthroscopic access from outside into the hip joint was described (15). The outside-in technique creates a virtual space just anterior to the hip capsule, from which the capsulotomy is performed in order to access the peripheral compartment first, without the need of fluoroscopy (Fig. 3) (16). Traction is applied only for assessing the central compartment, which can be performed avoiding the risk of damage to the labrum. A broad capsulotomy is frequently needed to access the joint and allow correct visualisation. This access has been reported to minimise the time of the surgery and apparently shorten the learning curve. However, there is still little data regarding its outcomes. To our knowledge, no studies have been published comparing the outcomes of the classic and the outside-in arthroscopic access to the hip.
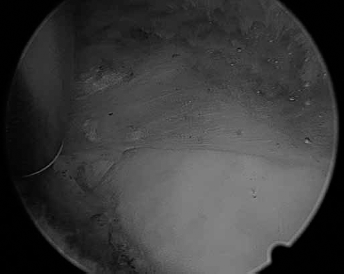
Arthroscopic view of capsulotomy regarding outside-in arthroscopic access to the hip.
The purpose of this study is to compare the functional outcomes between the classic and the outside-in access to the hip in patients undergoing arthroscopic surgery for the treatment of FAI. We hypothesised that there would be no differences between the outcomes, regardless the access used.
Methods
All patients undergoing arthroscopic treatment for FAI from January 2009 to June 2013 from a public institution were retrospectively reviewed. All surgeries were performed by a single team composed of 2 experienced arthroscopists. No major reason but the particular preference of the surgeon determined the use of the classic or outside-in access regarding each case. Only hips with a minimum follow-up of 12 months were included. Dysplastic hips with a centre-edge angle (CEA) (17) less than 20° measured on AP pelvis radiography preoperatively were excluded. During that time, a total of 101 hips met these criteria and were included in the study.
All arthroscopies were performed in the supine position using a standard fracture table. Intraoperative fluoroscopic imaging was only used for classic access. No specific prophylaxis for postoperative heterotopic ossifications was followed during the study.
To verify that both groups were homogeneous, data regarding affected side, gender, age, preoperative CEA measured on AP pelvis x-rays views, preoperative alpha angle measured on MRI studies (18), duration of symptoms and grade of osteoarthritis following Tönnis classification were registered and compared (17). Moreover, operative data regarding duration of surgery (from stab incision to the last stitch) and type of anaesthesia were also recorded and analysed.
To assess the functional outcome, the modified Harris Hip Score (mHHS) was used classifying results following the categories suggested by Byrd: 90-100 excellent; 80-89 good; 70-79 fair; <70 poor (19). Moreover, results were compared with regard to the access performed and grouped in excellent-good and fair-poor to easily distinguish between satisfactory and unsatisfactory outcomes. mHHS was recorded by the treating surgeon preoperatively and a minimum of 12 months after surgery. In addition, the joint motion (measured with a goniometer), the presence of complications (including heterotopic ossification graded following Brooker classification) (20) and other covariables were also analysed and compared with respect to both access techniques.
Regarding statistical analysis, the χ2 test was performed for qualitative variables; in case the expected number of occurrences was below 5 in more than 25% of the associations, Fisher's exact test was used. Additionally, the relationship between quantitative variables and each of the independent variables was analysed using Student's t-test (Mann-Whitney U test for nonparametric data). The sample size was calculated assuming a difference of a 20% in outcomes, with a confidence level of 95% and a power of 80%. Results were presented either showing the distribution of frequencies (for qualitative variables) or the mean, median (with standard deviation or interquartile range) and range (for quantitative variables); p values <0.05 were considered statistically significant. SPSS for Windows version 15.0 (SPSS Inc., Chicago, Illinois) was used for all statistical analyses.
Results
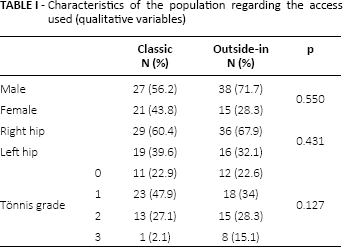
Of the 101 hips (91 patients) included in our study, 48 cases were arthroscopically accessed by a classic access and 53 by the outside-in technique. 10 patients underwent surgery on both hips at different times. Surgeries corresponded to a right hip in 64.4% cases and to a left hip in 35.6%. 58 (63.7%) were male and 33 (36.3%) female. The age ranged from 15.7 to 59.6, with a mean age (SD) of 37 (9) years. The mean follow-up (SD) was 22 (8) months (range 12-40 months). Preoperative mHHS showed a median (IQR) of 55 (19) points for the classic group and of 62 (19) for the outside-in. The mean alpha angle (SD) was 69° (12) and the CEA showed a mean value (SD) of 39° (7). According to the classification of Tönnis, 23 (22.8%) hips were classified as type 0, 41 (40.6%) as type 1, 28 (27.7%) as type 2 and 9 (8.9%) as type 3. Mean time (SD) from the start of symptoms to the surgery was 31 (3) months (range 5-137 months). No significant differences were found regarding these data between both groups (Tabs. I and II).
Characteristics of the population regarding the access used (qualitative variables)
Characteristics of the population regarding the access used (quantitative variables)
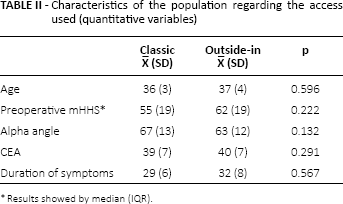
Results showed by median (IQR).
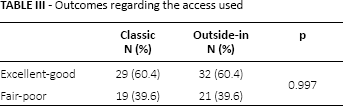
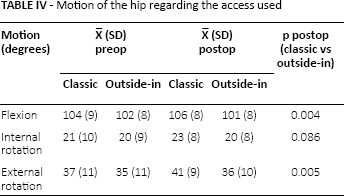
Patients were operated either under general anaesthesia or a combined general and spinal anaesthesia. Mean duration (SD) of surgery was 162 (11) minutes for outside-in access and 172 (12) minutes for classic. No differences were found in terms of these data between both groups. Regarding clinical outcomes, both groups of patients showed improvement of its mHHS. Postoperative medians (IQR) were 83 (32) and 83 (37) respectively and both accesses showed equal frequencies of excellent-good results (60.4%) and fair-poor results (39.6%), with no statistically significant differences between groups (Tab. III). Pre- and postoperative motion of the hip was also compared, showing statistically significant improved postoperative mobility in flexion and external rotation regarding the classic group (Tab. IV).
Outcomes regarding the access used
Motion of the hip regarding the access used
No major complications were observed. In 16 patients a transient neurological lesion was detected postoperatively, 9 in the group of classic access (8 femorocutaneous nerve and 1 pudendal nerve) and 7 in the outside-in group (3 femorocutaneous nerve, 2 pudendal nerve and 2 sciatic nerve). All neurologic complications recovered spontaneously. 12 patients underwent revision surgery: 10 a revision hip arthroscopy (5 for insufficient cam resection and 7 for labral or chondral revision) and 2 a total hip replacement. Of these, 8 corresponded to the classic access group and 4 to the outside-in, and all of them where classified as Tönnis type 2 or 3. No statistically significant differences were found between both access groups regarding these data.
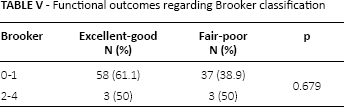
16 cases showed signs of heterotopic ossification (HO) according to Brooker. With respect to the access used, 12 patients had been operated by the outside-in technique and of these, 6 developed a Brooker grade 3 calcification. No Brooker grade 4 cases were registered. A statistically significant association (p = 0.017) was observed between HO and outside-in access. In addition, patients with high-grade HO (Brooker 2-4) showed poorer outcomes (Tab. V) although differences were not statistically significant.
Functional outcomes regarding Brooker classification
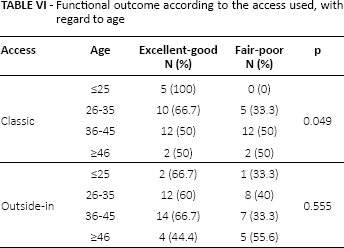
An analysis of the functional outcome according to patient age was included, showing a statistically significant difference towards the excellent-good results in patients under 35 years old who were operated using the classic arthroscopic access. The other age groups did not show any differences between both accesses concerning outcomes (Tab. VI).
Functional outcome according to the access used, with regard to age
Discussion
To our knowledge, this study is the first to compare the outcomes of patients treated for FAI using 2 different arthroscopic access techniques to the hip joint. Hips corresponding to the classic group showed statistically significant higher degrees of postoperative motion in flexion and external rotation, with a mean difference of 5°. In our opinion, a possible explanation to this difference would lie in the less aggressive management of the capsule and soft tissue surrounding the hip of the classic access. Nevertheless, in contrast with other reports, little and no improvement was found respectively in internal rotation amongst both classic and outside-in groups (21, 22).
No significant differences were observed in the outcomes measured by the postoperative mHHS between patients treated by using the classic and the outside-in access. However, a statistically significant difference towards excellent and good functional outcomes was observed for patients under 35 years old operated by using a classic access. This result would support the recommendation of using the classic access in younger patients.
Regarding immediate postoperative complications, our study was in line with other reports (23–24–25–26). However, with respect to late complications, we found a higher frequency of HO than reported by other authors, which was statistically associated with the outside-in access. HO has been reported as a complication in the literature (27–28–29–30) and for some authors it might be underestimated (31). Although high-grade calcifications around the hip were associated with poorer outcomes in our study, this difference was not statistically significant, probably due to the small number of patients. Reoperations rates were comparable in both groups and to reports by other authors (32).
This study has several limitations, mainly in relation to its retrospective design and the use of the mHHS. Although this score has been validated for hip arthroscopy (33, 34) and is the one used by most studied reporting on outcomes of hip arthroscopy (9, 35–36–37–38–39–40–41), it has limited responsiveness compared to modern scores like NAHS, HOS or iHOT and its reliability has not been tested (33, 42, 43).
In conclusion, no differences have been found between functional outcomes of patients operated by using classic or outside-in access. The classic access appears to offer better postoperative range of motion and lower risk of heterotopic ossifications.
Footnotes
Financial support: None.
Conflict of interest: None.