
Abstract
Purpose
The main aim of our study is to report the medium-term survivorship of Birmingham Hip Resurfacing (BHR) cup and a large modular metal head (MMT) on an uncemented Freeman femoral stem. No results have been reported till date with these implants combinations.
Methods
A total of 205 metal-on-metal total hip replacements (MoM THRs) were performed on 190 patients from October 2002 to November 2004. Prior to the Medicines and Healthcare Products Regulatory Agency (MHRA) guidelines, the patients were followed up at 3, 6 and 12 months postoperatively and annually thereafter. Following the MHRA alert in 2010, the patients were followed-up as per the MHRA guidelines.
All statistical analyses were conducted using Stata 13.
Results
At a mean follow-up of 10.5 years, a total of 42 out of 205 hips were revised for reasons related to ALTR. The failure rates increased significantly over time (7% at 6 years and 29% at 10-year follow-up). The analysis showed no statistically significant association to age, gender, side, BMI or component size or position (p<0.05). Blood metal ions showed a poor discriminant ability to separate failed from well-functioning MoM hip replacements.
Conclusions
Large head MoM BHR on an uncemented stem has extremely high failure rate. The authors do not recommend the use of large head MoM articulation in total hip arthroplasty in the wake of this report and similar findings across the world. Continued surveillance of these implants is required as the failure rates increase with time.
Keywords
Introduction
The metal-on-metal (MoM) bearings became popular due to the lower dislocation rates, expected reduced wear and their ability to provide a ‘natural feel’ with a better range of movement (1–2–3–4). The metal-on-metal total hip replacement (MoM THR) was initially introduced to counteract the potential disadvantages of femoral neck fracture that could occur in metal-on-metal hip resurfacings (5–6–7). The MoM THR retained the advantages of a large metal on metal bearing by using a modular head on a clinically proven femoral stem. This concept enabled the surgeons to use the metal on metal articulation, especially in cases where the anatomy did not favour resurfacing and very soon, the large-head MoM THR became a widely used primary option in the treatment of hip arthritis in the young and active patients.
The Birmingham Hip Resurfacing (BHR, Smith & Nephew, Warwick, UK) had shown excellent results except for the issues of femoral neck fracture (8). The Midland Medical Technologies (MMT, Birmingham, UK) introduced the large cobalt-chrome (Co-Cr) heads to counteract the problems encountered with femoral neck anatomy and neck fractures. These large metal heads were specifically engineered to fit the 12/14 taper geometry of the Freeman femoral stem (Finsbury Orthopaedics, Leatherhead, UK), which had previously shown excellent results in the conventional THR (9, 10)
However, widespread concerns exist regarding all MoM articulations due to the biological consequences of metal wear debris causing local tissue damage, which is broadly termed as ‘adverse local tissue reaction’ (ALTR) (11–12–13–14–15–16). The systemic risk of carcinogenesis remains unproven (17). The implant retrieval studies have incriminated the taper-neck junction of MoM THR as a major source of metal debris, apart from the articulating surfaces (18–19–20). The larger metal heads generate a higher frictional torque and a larger bending moment on the taper-neck junction causing increased corrosion (21). However, the wear mechanism and tissue response is multifactorial and includes patient, surgical and manufacturing parameters (19). The National Joint Registry for England and Wales (2014) reports an overall revision rate of 22% for MoM THR at 10 years (22). The failure rates in some independent series are as high as 48% at 6 years (13). Despite major advances in the understanding of ALTR, there are several unanswered questions, partly due to the lack of large clinical studies with long-term outcomes following large head MoM THR.
The medium-term results of Birmingham Hip Resurfacing (BHR) cup and a large modular metal head (MMT) on an uncemented Freeman femoral stem has not been reported in the literature to the best of our knowledge. The aim of our study was to report the medium-term survivorship of this implant performed by a single surgeon in our unit.
Methods
The study included all patients who underwent the large diameter MoM THR using the Birmingham Resurfacing acetabular component, Freeman femoral stem and large modular Co-Cr heads (Fig. 1). A total of 205 MoM THRs were performed on 190 patients from October 2002 to November 2004. A single surgeon using the modified Hardinge approach performed all procedures. Prior to the Medicines and Healthcare Products Regulatory Agency (MHRA) guidelines (16), the patients were followed up at 3, 6 and 12 months postoperatively and annually thereafter. Following the MHRA alert in 2010, the patients were followed up as per the MHRA guidelines (16).

Radiograph showing a Birmingham Resurfacing Cup with an uncemented Freeman stem.
Clinical assessment
All patients with large-head MoM hips were reviewed as per MHRA guidelines. Patients who had new onset pain around the hip, clicking/clunking of the hip or new onset limp were classed as ‘symptomatic hips’. Harris Hip Score (HHS), Western Ontario and McMaster Universities Osteoarthritis index (WOMAC) and Short Form 12 (SF-12) scales were used to evaluate the clinical outcome by a specialist research nurse.
Haematological assessment
All patients underwent annual blood tests for serum metal ion levels. As per the MHRA guidelines (10), metal ions were considered to be elevated if levels >7 parts per billion which translates to cobalt (Co) level of >119 nmol/L and chromium (Cr) level >134.5 nmol/L. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were measured in symptomatic patients.
Radiological assessment
Plain radiographs included anteroposterior (AP) views of the pelvis and cross table lateral views of the hip. Acetabular component inclination and version were measured using the TraumaCad system (Voyant Health, Petach-Tikva, Israel). The radiographs were assessed by 2 authors independently for progressive radiolucencies around the acetabular and femoral components, bone resorption, component migration and osteolysis (23). Further imaging was considered in patients with symptomatic hips and/or rising serum metal ion levels in line with the MHRA guidelines. The patients underwent magnetic resonance imaging (MRI) using metal artefact reduction sequence (MARS) technique. A small group of patients who could not have MRI scan (claustrophobia, pacemaker) underwent ultrasound examination. All imaging was reported by experienced musculoskeletal radiologists.
Histological analysis
Tissue samples were sent for histological examination from all patients who underwent revision surgery. The specimens were analysed by an experienced pathologist to detect tissue changes consistent with metallosis. The histological manifestations of adverse reaction to metal debris range from associated lymphocyte dominated vasculitis associated lesion (ALVAL), pseudotumours, foreign body giant cell reactions with macrophages containing metal debris. For the purpose of this study, we will use the umbrella term ‘ALTR’ to encompass all the pathological changes attributable to MoM articulation.
Diagnosis of ALTR
The confirmation of the diagnosis of ALTR was made on the histological evidence. Tissue samples were sent to microbiology and histology to rule out prosthetic joint infection as the cause for failure.
Revision
The indication for revision surgery was based on the MHRA guidelines. However, prior to the MHRA guidelines, the revision surgery was offered to all symptomatic patients with evidence of loosening, osteolysis, fluid collections or pseudotumours on imaging (MRI/ultrasound) or rising serum metal ion levels.
Statistical analysis
Baseline demographics have been summarised as frequency (%) for categorical variables and median (IQR) for continuous variables. Survival functions were estimated using the Kaplan Meier method (24). Revision-free probabilities were initially calculated by classifying an event as revision due to any cause and for revision due to ALTR only. Patients who had a revision due to other causes or died were censored at date of revision/death. The univariate association of each variable with revision-free survival was investigated using Cox regression models. A multivariable Cox regression model was then fitted including all variables and a stepwise model selection procedure using Akaike's Information Criteria (AIC). All statistical analyses were conducted using Stata 13.
Exploratory analysis was conducted upon the variables to identify any associations between each other, using repeated-measures analyses. All models were adjusted for time.
Results
The demographics of the 205 hips are outlined in (Tab. I). The mean duration of follow-up was 8.3 years (range 3-11 years). 21 patients (22 hips) died from causes unrelated to the THR.
Demographics and reasons for failure
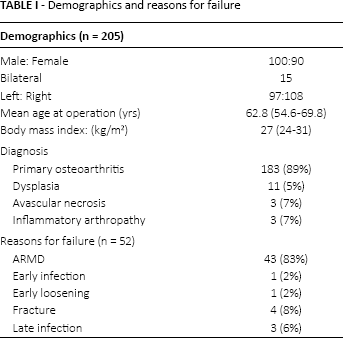
A total of 52 hips (25.4%) required revision. Of the 52 revisions, 43 hips were revised for ALTR and 9 hips were revised for reasons other than ALTR (Tab. I). Intraoperative findings ranged from periprosthetic fluid collection, caseous necrotic material and moderate to severe soft tissue damage with complete loss of hip abductors and bone loss. The diagnosis of ALTR was confirmed histologically in all the 43 cases.
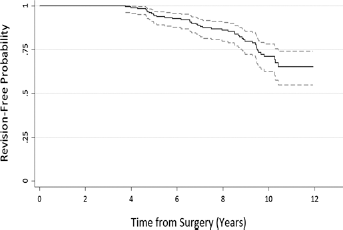
Survival
The cumulative survival for the implant with endpoint as revision for any reason was 98% at 2 years, 90% at 6 years and 68% at 10 years (Fig. 2). The survival of the implant with ALTR as the cause of revision was 100% at 2 years, 93% at 6 years and 71% at 10 years (Fig. 3).

Kaplan-Meier survival curves with 95% confidence intervals for all patients with the endpoint being revision for any reason.
Kaplan-Meier survival curves with 95% confidence intervals for all patients with the endpoint being revision for ALTR reason.
Univariate analysis was performed on the 196 hips in 181 patients (9 hips revised for reasons other than ALTR were excluded). The analysis showed no association to age, gender, side, BMI or component positioning (Tabs. II and III). The only statistically significant factor that was found to be associated with failure was the time from index surgery (p<0.001).
Comparison of patient demographics, component sizes and position and blood metal ion levels in the unrevised and the revised group
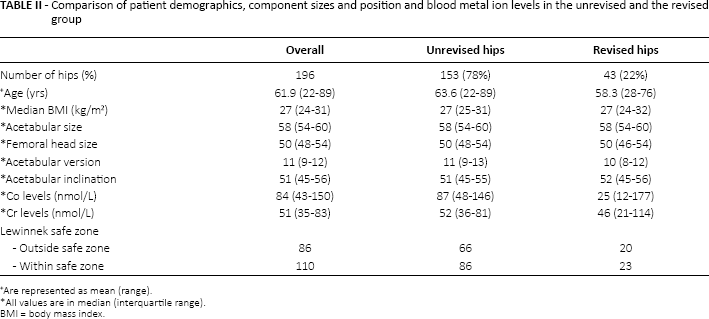
Are represented as mean (range).
All values are in median (interquartile range).
BMI = body mass index.
Analysis showing the association of each variable with revision for adverse local tissue reaction (ALTR) (n = 196 hips)
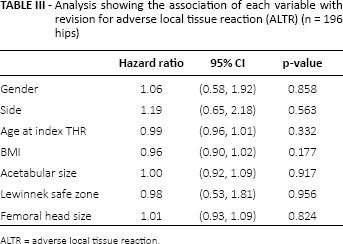
ALTR = adverse local tissue reaction.
Blood metal ions were found to have no significant association with the acetabular cup size, femoral head size or the acetabular inclination, version or Lewwinnek's safe zone (30°-50° inclination, 5°-25° anteversion), (Fig. 4).
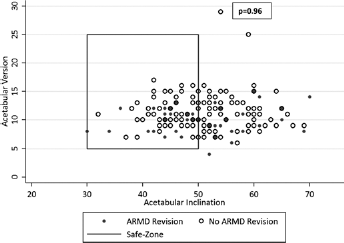
Acetabular component position vs. revision for adverse local tissue reaction (n = 196 hips). ARMD = adverse reaction to metal debris.
Receiver Operating Characteristic (ROC) analysis was used to assess the discriminatory ability of Co and Cr levels to detect patients with and without revision due to ALTR. The discriminatory ability of the MHRA suggested cut off points was also investigated (Fig. 5). It was found for this sample that Co and Cr levels are unable to satisfactorily discriminate between patients with and without a revision due to ALTR. Also, an elevated blood metal ion level did not imply poor clinical outcome (HHS, WOMAC or the SF12 scores).
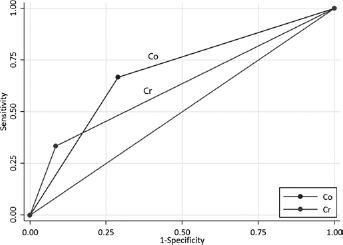
Receiver Operating Characteristic (ROC) analysis of Co-Cr blood tests using MHRA thresholds.
The only factor that showed significant association with the incidence of ALTR and risk of revision for ALTR was the time since index operation. The blood metal ion levels did not have any correlation to ALTR or risk of revision (p<0.05). The functional outcome scales were also analysed for their ability to detect MoM failures. The WOMAC function and the SF 12 Physical components showed some usefulness in detecting ALTR (p = 0.024 and p = 0.017 respectively), but the HHS had no association with a failing THR.
Plain radiographs showed changes such as medial calcar scalloping and resorption in a majority of the cases (74.4%). In our study, the majority of the patients had ultrasound scans and some of the patients could not undergo MRI for various reasons (claustrophobia, pacemaker, etc.) However, of the 10 hips that underwent a MRI prior to revision for ALTR, the scans were useful in predicting the level of tissue damage in all the 10 hips. The radiological findings of osteolysis, radiolucent lines or calcar resorption in symptomatic hips was a significant predictor for revision for ALTR (p<0.05).
Discussion
To the best of our knowledge, our study is the largest reported series of large diameter MoM THR with a long-term follow-up. This is a single surgeon, single institute study using a single implant combination that has previously never been reported. There have been increasing concerns with the long-term outcomes of large diameter MoM THR due to the unexpectedly high failure rates noted in various joint registries as well as independent series (14, 15, 20, 22, 25–26–27–28). The National Joint registry for England & Wales shows a 10-year revision rate of 22% for MoM THR (22). The survivorship in our series was 68% at 10 years. The failure rates appear to be higher compared to the previously published literature. In our opinion, 1 of the reasons accounting for higher failure rate is the long-term follow-up of our study. There is increasing evidence in the literature indicating that ALTR exponentially increases with time. Bolland et al (20) showed that the mean time to ALTR requiring revision surgery was 46-61 months. Langton et al (13) have reported accelerating failures of MoM THR. A similar picture is evident in our series as well. The failure for ALTR at 6-year follow-up was 7% (10 hips). A further 22% (33 hips) have failed during the 6- to10-year period. Our results clearly suggest that the time from index procedure is an important variable associated with changes of ALTR and risk of revision (p<0.05). Our study, along with a couple of other reports (13, 29), lends further support to the existing follow-up guidelines on large-diameter MoM THR outlined by the MHRA (16). These findings may also benefit the local health services in planning future resources for the increasing revision burden with time.
BHR cups in hip resurfacing arthroplasty and the Freeman femoral stems in conventional metal-on-poly THR have shown excellent results in various studies (8, 9). BHR cups when used in resurfacing showed a failure rate of 0.3% for ALTR (30), but there is 1 study, which analysed the performance of BHR cup in large-head MoM THR and reported a failure rate of 15% (20). In addition to the bearing surface wear, biomechanical studies have shown that the use of large heads on stems with narrow tapers results in excessive wear due to increased frictional torque and bending moments on the trunnion (18, 19). The MMT large modular heads were specifically designed to fit the taper of Freeman femoral stem and hence was expected to have superior wear and corrosion properties compared to using a BHR cup on other stems. Despite this, intraoperatively, trunnionosis was evident in all our cases that underwent revision surgery for ALTR.
There are conflicting reports describing various factors associated with increased risk of wear in the MoM THR. We did not find any association between age, gender, BMI, femoral head size, femoral neck offset, acetabular cup size, or position to increased blood metal ions, radiological changes or increased revision rates (19–20–21, 31, 32).
It has been suggested that acetabular component positioning outside Lewinnek's safe zone (acetabular inclination of 30°-50° and acetabular anteversion of 5°-25°) may be responsible for increased wear and failure in MoM THR (12, 33, 34). Our analysis did show 42% of the cups to lie outside the safe zone, but there was no significant difference in the blood metal ion levels, incidence of ALTR or increased risk of revision. The findings may lend further evidence to the fact that the mode of failure in hemispherical large-head MoM THR is due to taper corrosion, rather than edge-loading as described in some ASR studies (13, 14, 28).
Previous studies have claimed that elevated blood Co-Cr levels have a good discriminant ability to separate failed from well-functioning MoM hip replacements (14, 16, 35–36–37), but the optimum cut-off value is still a matter of debate (30). In our study, we did not find any statistically significant difference in the metal ion levels between the failed and the well-functioning MoM THR. The blood Co-Cr test did show a fairly good negative predictive value (92.1% for Co, 89.9 for Cr) but a poor positive predictive value (28.2 for Co, 46.7 for Cr) at MHRA thresholds, which means a positive blood test could not predict failure. On the other hand, although the blood metal ions serve as a useful and a relatively easy test to perform, it is unwise to assume the metal wear is directly proportional to the blood metal ions. Individuals have varying rate of absorption and metabolism of these ions. Furthermore, imaging with MARS MRI has been shown to be very sensitive in identifying local tissue changes consistent with the intraoperative findings of ALTR. The radiological changes are thought to reflect a combination of high component wear rate and tissue reaction to metal wear debris. Our study shows that there was no association between elevated blood metal ions and radiological or clinical ALTR changes. This has been described in some recent reports (38) and perhaps re-ignites the issues of metal hypersensitivity or the possibility of a genetic variability, exhibited by certain individuals making them more vulnerable to local tissue damage despite low blood metal ions. More recently, the cobalt ions have been shown to bind and activate a key immune cell receptor, TLR4 (toll like receptor 4) that has the ability to induce abnormal inflammatory response by increasing IL-8 (interleukin 8) and CXCL10 (C-X-C motif chemokine 10) secretion (39). The lack of correlation between blood metal ions and incidence of ALTR has been noted in few other studies (18), which may have future implications in justifying their usefulness in surveillance of MoM THR.
The HHS, WOMAC and SF-12 scales are universally accepted and validated tools for analysing the clinical performance of THR (40). Patients who had bilateral MoM THR were excluded for metal ion analysis. Our study showed no significant association of poor HHS with blood metal ions or diagnosis of ALTR. Similar finding has been seen in one other report, perhaps due to the ceiling effect as previously described. However, patients with ALTR showed deteriorating scores on the WOMAC stiffness subscale. This corresponds to the clinical presentation of reasonably good function despite elevated metal ions and radiological changes in failing metal on metal hip replacements. Often the only symptoms they complain of is stiffness. The SF-12 Physical parameter was useful in predicting failure. None of the current scoring systems are fool proof (41) in the evaluation of MoM THR and maybe there is a need for devising a new objective scoring tool specific to deal with ALTR related issues.
One of the limitations to our study is that we did not perform wear analysis studies on any of the retrieved implants, primarily due to logistic and financial constraints. We agree that the retrieval analysis would have further strengthened our understanding of trunnion behaviour.
Conclusion
The authors do not recommend the use of large-head MoM articulation in total hip arthroplasty due to the extremely high failure rates. Continued surveillance of these implants is required as the failure rates increase with time.
Markers of metal wear (blood Co-Cr level) are not very reliable; radiological changes are more predictive. Further research on biological inflammatory markers is required to identify the patients at risk of developing ALTR.
Footnotes
Financial support: None.
Conflict of interest: None.