
Abstract
Introduction
Despite improvements in the technique of femoral impaction bone grafting, reconstruction failures still can occur. Therefore, the aim of our study was to determine risk factors for the endpoint re-revision for any reason.
Methods
We used prospectively collected demographic, clinical and surgical data of all 202 patients who underwent 208 femoral revisions using the X-change Femoral Revision System (Stryker-Howmedica), fresh-frozen morcellised allograft and a cemented polished Exeter stem in our department from 1991 to 2007. Univariable and multivariable Cox regression analyses were performed to identify potential factors associated with re-revision.
Results
The mean follow-up was 10.6 (5-21) years. The cumulative re-revision rate was 6.3% (13/208). After univariable selection, sex, age, body mass index (BMI), American Association of Anesthesiologists (ASA) classification, type of removed femoral component, and mesh used for reconstruction were included in multivariable regression analysis.
In the multivariable analysis, BMI was the only factor that was significantly associated with the risk of re-revision after bone impaction grafting (BMI ≥30 vs. BMI <30, HR = 6.54 [95% CI 1.89-22.65]; p = 0.003).
Conclusions
BMI was the only factor associated with the risk of re-revision for any reason. Besides BMI also other factors, such as Endoklinik score and the type of removed femoral component, can provide guidance in the process of preclinical decision making. With the knowledge obtained from this study, pre-operative patient selection, informed consent, and treatment protocols can be better adjusted to the individual patient who needs to undergo a femoral revision with impaction bone grafting.
Keywords
Introduction
Femoral impaction bone grafting is a biological reconstruction which replenishes bone stock defects in revision total hip arthroplasty (THA) by impacting fresh-frozen morcellised allograft within the femoral medullary canal before insertion of a cemented stem.
Long-term follow-up data are now available showing excellent survivorship for the endpoint re-revision for aseptic loosening, ranging from 98% to 100% after a mean follow-up of between 7 and 17 years (1–7).
Nevertheless, despite technical improvements like the use of specially designed instrumented femoral revision systems (introduced in 1991) and longer stems to bypass weak cortical areas (8, 9), re-revisions for any reason still occur with survival ranging from 93% to 96% (1, 5–7). These results are quite acceptable, however in our opinion further improvements of this valuable technique for femoral revision surgery can be achieved by proper identification of risk factors for re-revision.
The only study that reported on factors associated with re-revision in femoral impaction grafting revisions was performed by Lamberton et al (3). They concluded that the indication for femoral revision surgery and the use of any kind of reinforcements were factors that significantly increased the risk of failure for any reason. However, several potential important risk factors for re-revision in femoral revisions, such as Endoklinik classification, American Association of Anesthesiologists (ASA) classification and the type of the removed femoral component were missing.
Therefore, we designed this study to identify demographic, clinical and surgical risk factors for re-revision for any reason in femoral revisions performed with use of impaction bone grafting. Our rationale was that by identifying these risk factors, the results of this valuable technique in revision hip arthroplasty can be further improved.
Methods
Selection of study cohort
We used prospectively collected pre-operative and postoperative data on all patients who underwent a femoral component revision with use of a cemented polished Exeter stem (Stryker-Howmedica) and impaction bone allografting in our department between March 1991 and December 2007. This study is a consecutive unselected series, including the learning curve of the very first cases. Our policy is to perform all femoral revisions with bone stock loss with this technique, and we used the X-change femoral instrumented revision system (Stryker-Howmedica) in all hips.
In patients who need to undergo a femoral revision without bone stock defects and have an intact cement mantle below the lesser trochanter, we generally choose to perform a cement-in-cement revision (10). In femoral revisions without bone stock loss, or in patients with bone stock loss and a weak physical condition and/or very old age, we generally choose to perform a cemented revision with a polished stem without bone impaction grafting. These patients were excluded from the current study.
Characteristics of study cohort
Between March 1991 and December 2007, 202 patients (119 female [57%]) underwent 208 consecutive femoral revisions using bone impaction grafting and a cemented polished stem. Mean age at time of operation was 65 (30-86) years. 1 patient was lost to follow-up after 6 years (0.5%). At review in December 2013, 135 patients (64.9%) were alive and had a non re-revised femoral component after a mean follow-up of 10.6 (5-21) years. All other demographic features are stated in Table I.
Surgical technique
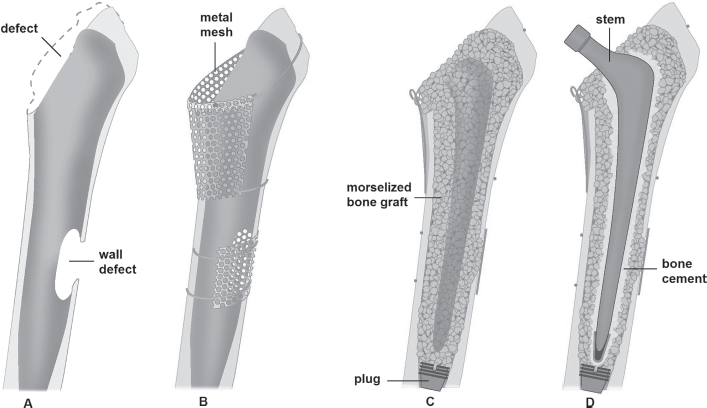
The surgical technique has been previously described in detail (11). In short, after removal of the old stem, the femoral shaft is cleaned and reamed (Fig. 1A). If needed, segmental defects are reconstructed with metal wire meshes. Also reconstruction of the calcar region is often necessary (Fig. 1B). A femoral plug with a guide wire attached is then inserted in the femoral shaft at least 4-5 cm below the most distal defect. Over this guide wire, a phantom implant is used to impact the morcellised bone grafts with a diameter of 2-5 mm in the femoral shaft (Fig. 1C). For the proximal part of the femur, larger morcellised grafts with a diameter of 6-8 mm can be used and these are solidly impacted around the phantom with special small impactor creating rotational stability of the final implant. Cement is injected retrograde using a syringe with a narrow nozzle that allows reaching the distal grafted area without damaging the graft reconstruction. Finally the femoral implant can be inserted and cemented into the newly reconstructed femur (Fig. 1D).
Demographic features of the study cohort
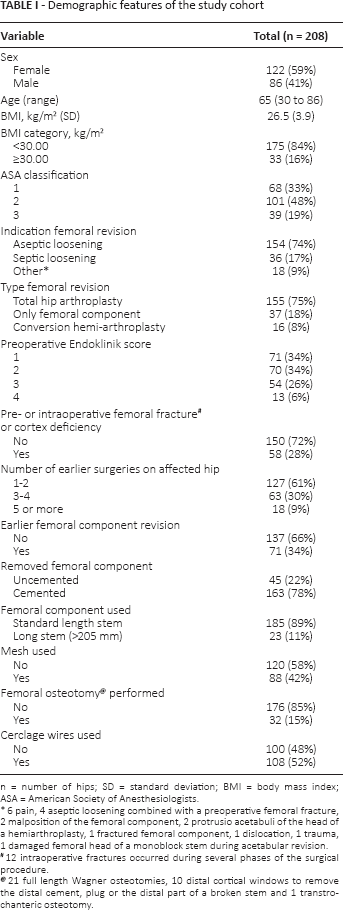
n = number of hips; SD = standard deviation; BMI = body mass index; ASA = American Society of Anesthesiologists.
6 pain, 4 aseptic loosening combined with a pre-operative femoral fracture, 2 malposition of the femoral component, 2 protrusio acetabuli of the head of a hemiarthroplasty, 1 fractured femoral component, 1 dislocation, 1 trauma, 1 damaged femoral head of a monoblock stem during acetabular revision.
12 intraoperative fractures occurred during several phases of the surgical procedure.
21 full length Wagner osteotomies, 10 distal cortical windows to remove the distal cement, plug or the distal part of a broken stem and 1 transtrochanteric osteotomy.
(
Follow-up protocol
A standard postoperative follow-up protocol was used, with physical and radiographic examination after 6 weeks, 3 months, 6 months, 1 year and afterwards on an biennially basis. The time period between 1991 and 2007 was chosen to collect a sufficient enough sample of patients, and to provide a minimum follow-up period of 5 years for all patients. This study was approved by our Institutional Review Board and all investigations were conducted in conformity with ethical principles of research.
Study endpoint and predictors
The study endpoint was a femoral re-revision for any reason, which was defined as any exchange of the femoral stem for a new component during the study follow-up. Potential demographic, clinical and surgical factors associated with a femoral re-revision were obtained from patient files (Tab. I). Decision to include these variables was based on guidance from directed acyclic graphs (12).
Aseptic loosening was defined as a revision without pre-operative diagnostic evidence of infection and/or without intraoperative visual evidence of infection and negative intraoperative cultures. Septic loosening was defined as a revision with pre-operative diagnostic evidence and intraoperative visual evidence of infection and/or at least 2 of the 6 intraoperative taken cultures positive. The BMI was dichotomised. The choice to cut off the BMI at 30 was made to differentiate between people with (BMI ≥30) and without (BMI <30) obesity (13).
Statistics
The associations between each variable and re-revision were examined with univariable Cox regression analyses. Predictors that were associated with the outcome in univariable analyses (p values <0.20) were included in multivariable Cox regression analyses. In multivariable Cox regression analyses p values less than 0.05 were considered significant. Hazard ratios (HR) are presented with 95% confidence interval (CI).
Analysis of the data was carried out using IBM SPSS Version 20.0 (IBM Corp.).
Overview of the 13 femoral re-revisions for any reason
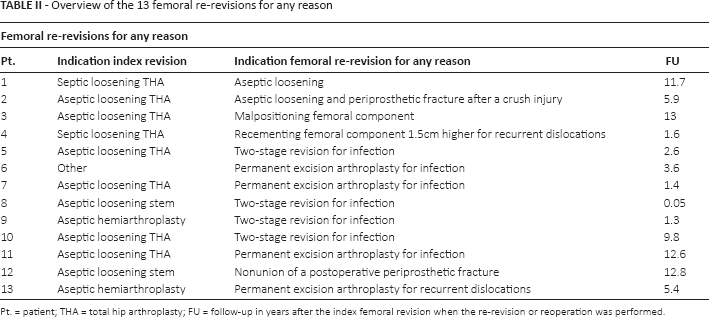
Pt. = patient; THA = total hip arthroplasty; FU = follow-up in years after the index femoral revision when the re-revision or reoperation was performed.
Results
The cumulative incidence of the endpoint femoral re-revision for any reason was 6.3% (13/208 patients). The most common reason for a re-revision was a postoperative infection (7/13 patients, 53.8%). In Table II a comprehensive overview of these 13 re-revisions is presented. The clinical outcomes and survival analyses of this patient cohort were recently described in detail (6).
The results of the univariable and multivariable regression analyses are presented in Table III. Sex (univariable HR = 2.12 [95% CI,0.70-6.38]; p = 0.18), age (univariable HR = 0.96 [95% CI,0.93-1.00]; p = 0.048), BMI (BMI ≥30 vs. BMI <30, univariable HR = 5.21 [95% CI,1.75-15.52]; p = 0.003), ASA (ASA grade 2 vs. ASA grade 1, univariable HR = 4.68 [95% CI,1.01-21.66] and ASA grade 3 vs. ASA grade 1, univariable HR = 1.34 [95% CI,0.12-15.01]; p = 0.09), type of removed femoral component (cemented vs. uncemented, univariable HR = 0.42 [95% CI,0.14-1.28]; p = 0.13), and mesh used for reconstruction (univariable HR = 2.11 [95% CI,0.69-6.46]; p = 0.19) were included in multivariable regression analysis.
BMI (BMI ≥30 vs. BMI <30, HR = 6.54 [95% CI,1.89-22.65]; p = 0.003) was the only factor that was significantly associated with femoral re-revision for any reason in multivariable analysis (Tab. III and Fig. 2).
Discussion
In order to improve the results of femoral revisions performed with impaction bone grafting, our goal was to determine which demographic, clinical and surgical characteristics were associated with the risk for a re-revision for any reason.
The most important finding in the present study was that patients with a BMI of ≥30 have a higher risk for re-revision for any reason compared to patients with a BMI <30.
The only other study that reported on risk factors for re-revision after femoral impaction bone revisions was performed by Lamberton et al (3). They included 540 femoral revisions with a mean follow-up of 6.7 years. The indication for the femoral revision surgery and the use of reinforcements were reported to be significant risk factors for re-revision. However, this study was not designed to identify risk factors and some important potential factors associated with the risk of re-revision, such as Endoklinik classification, ASA classification and the type of the removed femoral component were missing. A higher Endoklinik classification often results in the use of more reinforcements during surgery, and adjusting for Endoklinik classification might probably have neutralised the effect of the use of reinforcements.
In our study, a BMI ≥30 at the time of the index revision was the only significant risk factor for a re-revision for any reason (multivariable HR = 6.54 [95% CI,1.89-22.65]; p = 0.003). This can probably be explained by the fact that a higher BMI results in chronically higher biomechanical loads on the reconstruction. Lübbeke et al (14) and Pulos et al (15) also showed that obese patients who had undergone a revision total hip arthroplasty had a significant higher risk for a postoperative infection, which was the primary reason for re-revision in our study population. In addition, Pulos et al (15) also found that revisions in obese patients had a significant higher risk for reoperation. In our opinion, obesity is an important risk factor to discuss with the patient in the pre-operative phase. Obese patients can be advised to first lose some weight with for example a dietary program before a femoral revision using impaction allografting is considered.
Remarkably, Endoklinik score was not associated with an increased risk of re-revision. However, an Endoklinik grade 4 score presented a higher re-revision rate of 15% compared to 8% for grade 1, 6% for grade 2 and 2% for grade 3. Garcia-Cimbrelo et al (2) also stated that major bone defects may affect the clinical outcome. Their survival rate in 91 revisions for endpoint reoperation for any cause was 100% for type 2, 81.2% for type 3 and 70.8% for type 4.
Univariable and multivariable-adjusted risk of re-revision for any reason following cemented femoral revision with use of impaction bone grafting
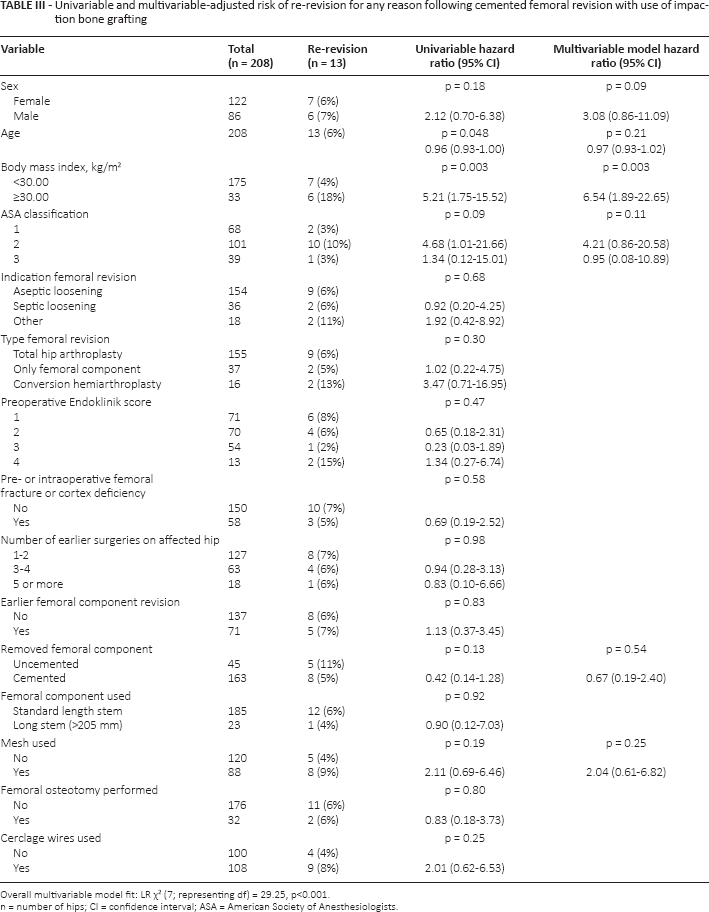
Overall multivariable model fit: LR χ2 (7; representing df) = 29.25, p<0.001.
n = number of hips; CI = confidence interval; ASA = American Society of Anesthesiologists.
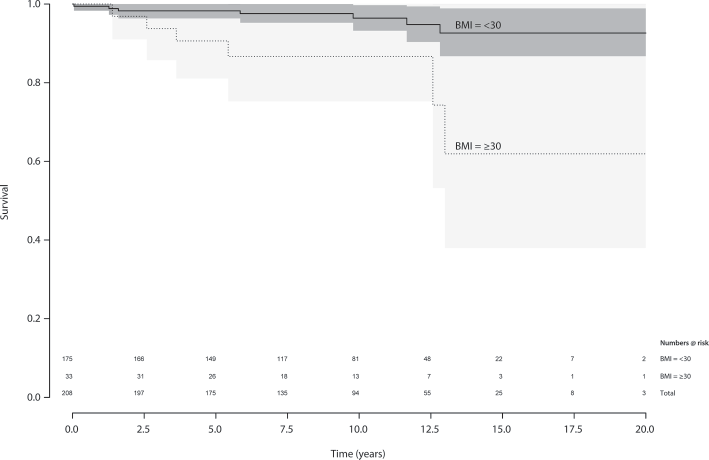
Kaplan–Meier curves showing re-revision free survival for patients with BMI <30 and BMI ≥30. Uncertainty is shown by 95% CIs and the numbers-at-risk at the bottom of the graph.
Although not significantly associated with the risk of re-revision (multivariable HR 0.67 [95% CI,0.19-2.40]; p = 0.54), the removed cemented stems showed a failure rate of 5% versus 11% for uncemented stems. We think that this difference can be explained by the fact that a revision of an uncemented stem in our opinion often is more difficult than a revision of a cemented stem. This is supported by other data from the present study: during revisions of uncemented stems we used more osteotomies (35.6% vs. 9.8%), cerclage wires (71.1% vs. 46.6%) and meshes (46.7% vs. 41.1%) compared to revisions of a cemented stem.
Similar to Lamberton et al (3), we also found that the use of reinforcements resulted in higher failure rates. However, in the present study the use of reinforcements was not significantly associated with the risk of re-revision.
Although the size of our group was not extensive with 202 patients (208 revisions), we think that our results are significant and clinically relevant. To the best of our knowledge, this is the first study that was designed to determine risk factors for failure of femoral revisions performed with bone impaction grafting. The strengths of the present study were the inclusion of a substantial number of possible important modifiable patients characteristics (e.g. BMI) and surgical characteristics (e.g. length of the used femoral component), and the use of prospectively collected data.
Some limitations have to be discussed. First, we dichotomised a number of variables (e.g. BMI). By the use of various cut points in different studies results may be difficult to compare. In addition, information is lost, e.g. every value above the cut point is considered equal, and so the statistical power to detect a relation might be reduced (16). Second, the number of re-revisions in our patient population was rather low (13 cases), potentially reducing the statistical power to detect a relationship. Rules of thumb, such as that logistic and Cox models should be used with a minimum of 10 outcome events per predictor variable, are useful signals for potential inaccuracies (e.g. reduction of statistical power) (17, 18). However, it has also been reported that these numbers might be a bit too conservative (19).
In conclusion, BMI was the only factor associated with the risk of re-revision for any reason. We acknowledge that a BMI ≥30 is no hard evidence for a negative outcome after a femoral revision using impaction bone grafting, but a factor that can be used as guidance in the process of preclinical decision making. Nevertheless, also factors that were nonsignificantly associated with the risk of re-revision, such as the higher failure rates for Endoklinik grade 4 and the revisions of uncemented stems, can obviously provide valuable information in this process. With the knowledge obtained from this study, pre-operative patient selection, informed consent and treatment protocol can be better adjusted to the individual patient who needs to undergo a femoral revision with impaction bone grafting.
Footnotes
Financial support: None.
2 of the authors (WHCR and BWS) certify that they have received an educational grant for instructional course lectures from Stryker-Howmedica during the study period.