
Abstract
Background
2-stage revision with the use of an antibiotic-loaded interval spacer is therapy of choice in late periprosthetic joint infection for most surgeons. For the spacer, either a prefabricated, functional articulating or custom-made spacer can be used. Little is known about which type of spacer provides optimal outcome after 2-stage revision. The aim of this study was to determine which type of spacer provides the best results, when used in 2-stage revision of an infected THA.
Methods
We performed a systematic review of the literature to analyse which type of interval spacer provides highest infection eradication rate and best functional outcome after a minimum 2 year follow-up. Exclusion criteria were follow-up of less than 2 years, single-stage revision, or 2-stage revision without use of a spacer.
Results
25 studies were included. Infection eradication rate was similar with rates of 96%, 93% and 95% for the prefabricated-, functional articulating- and custom-made spacers respectively. Functional outcome was scarcely described. Postoperative HHS was 81, 90 and 83 respectively.
Conclusions
Functional articulating spacers achieve a comparable rate of infection eradication in the treatment of periprosthetic hip joint infections as compared to preformed or custom-made antibiotic-loaded spacers. There is insufficient evidence concerning rehabilitation and functional outcome after 2-stage revision hip arthroplasty to advocate or discourage the use of either kind of interval spacer.
Keywords
Introduction
Periprosthetic joint infection (PJI) is a devastating complication after primary and revision arthroplasty. The number of total hip arthroplasties performed yearly is expected to increase drastically in the coming decades (1). Even if the percentage of PJI can be decreased, this will cause an increase in the absolute number of PJI requiring treatment. This development asks for standardised evidence based protocols describing the best type of treatment for PJI. Debridement, antibiotics and implant retention are treatment of first choice in case of early infection after total hip arthroplasty (THA) (2, 3). In case of late or persisting infection, 1- or 2-stage revision needs to be performed according to global consensus (3, 4). The use of different kinds of spacers in 2-stage revision surgery has been widely debated in the past years (5, 6). Various preformed spacers are available, as well as functional articulating spacers and spacers custom-made by individual surgeons following a local protocol.
The aim of this study was to determine which type of spacer should be used during the interval of 2-stage revision of an infected THA. First, we hypothesise that functional articulated spacers achieve infection eradication results comparable to other types of spacers. Second, we hypothesise that the rehabilitation period is shorter and patients’ functional outcome is improved after 2-stage revision with the use of a functional articulated spacer. In addition, we compared the incidence of spacer-related complications between the groups.
Methods
A review protocol was constructed and registered at PROSPERO international prospective register of systematic reviews (http://www.crd.york.ac.uk/PROSPERO/) with reference number CRD42014014324.
The search term can be found in Appendix 1. The search was limited to adult humans and the databases (Pubmed/Medline, Embase, and Cochrane Library) were searched from 1978 to April 1st 2015. The lists of references of retrieved publications were manually checked for additional studies potentially meeting the inclusion criteria and not found by the electronic search. 1-stage revision, 2-stage revision without use of a spacer, in vitro studies and studies with a follow-up of less than 2 years were exclusion criteria. Studies on objective or functional outcome were selected and more closely reviewed by 1 of the authors (EV) and verified by a second author (DJM).
We extracted all information regarding the level of evidence, mean years of follow-up, number of patients initially included in the study and the number of patients available for follow-up, baseline patient characteristics and baseline clinical and laboratory findings. Data regarding type of spacer and antibiotics used, timing of second stage surgery, tissue culture results, postoperative regimen, functional outcome and patient satisfaction were extracted. The type of spacer was identified and studies were divided into 3 groups. Group I comprised studies using a preformed spacer (such as the Spacer-G) (Fig. 1A), Group II comprised studies using a functional articulating spacer (Fig. 1B) and Group III comprised studies using a custom-made spacer either from a prefabricated template or manufactured by the individual surgeons following a local protocol.

Postoperative radiograph of a patient with: (
A spacer is considered a functional articulating spacer when patients are encouraged to bear partial to full weight and rehabilitation is stimulated. Functional articulating spacers consist of (parts of) regularly used prosthetic hip devices combined with antibiotic cement. An example is the PROSTALAC spacer. A spacer is considered a custom-made spacer when a mold (either prefabricated or constructed by the authors of the original article) is used intraoperatively to construct a cement spacer, with or without the addition of any kind of internal stabilisation.
The data included in the articles were extracted by 1 author (EV) and verified by a second (DJM). Primary outcome was success rate of infection eradication, defined as retention of the revision prosthesis at final follow-up without signs of recurrent infection. Secondary outcomes were the number of adverse events or complications and patient satisfaction and functional recovery as measured by patient reported outcome measures (PROMs).
Studies were graded according the scoring system of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group (http://www.gradeworkinggroup.org/index.htm, accessed April 1st 2015). In short, for studies on therapy or prognosis, Level I is attributed to well designed and performed randomized controlled trials, Level II are cohort studies, Level III are case-control studies, Level IV are case series and Level V are expert opinion articles.
Results
The search resulted in a total of 375 related studies, of which 93 studies were selected for additional review of the full text. A total of 25 studies met our inclusion criteria and were included for data analysis (Fig. 2) (4, 7–8–9–10–11–12–13–14–15–16–17–18–19–20–21–22–23–24–25–26–27–28–29–30). General characteristics of the included studies can be found in Table I. All reported averages in Table II are sample size weighted. Pooling of the overall results was not possible due to the clinical heterogeneity of the data. As a consequence no statistical analysis could be performed. Outcome after treatment will also depend on extent of infection, delay in treatment, virulence and susceptibility of infecting agents, quality of surgical debridement, type and extent of antibacterial treatment, compliance with treatment and so on. These potential confounders were in general poorly reported and when described heterogeneity of these factors was too large to analyse the effect on outcome.
General characteristics
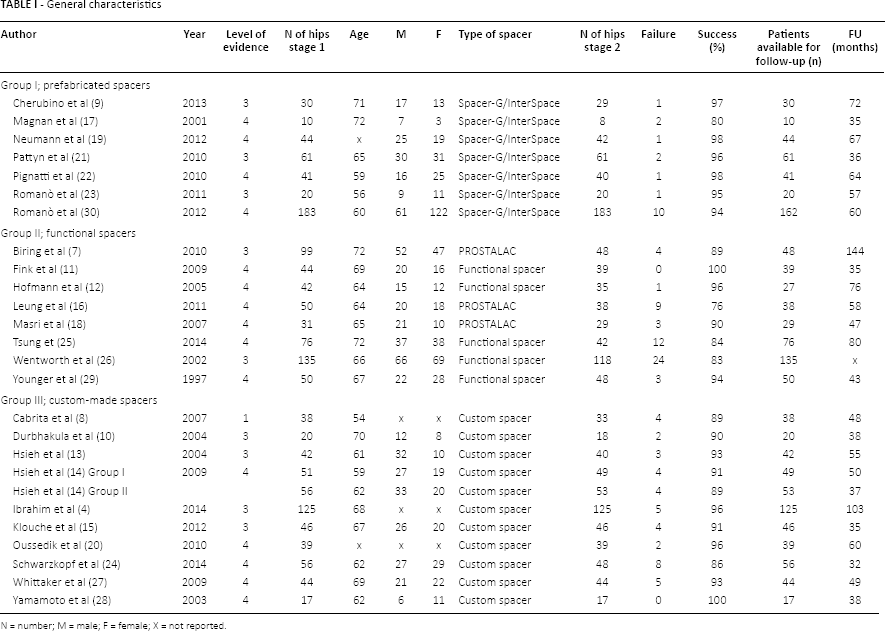
N = number; M = male; F = female; X = not reported.
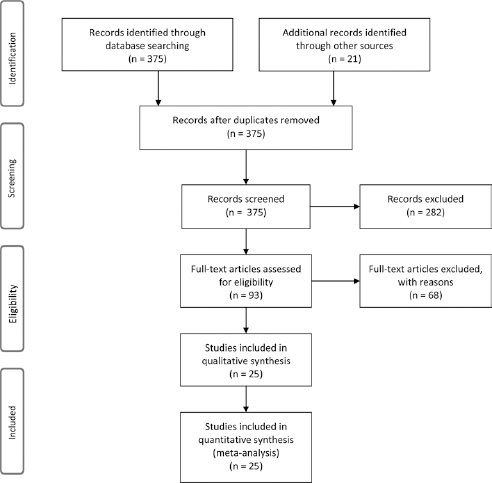
Flow diagram of included studies.
7 studies described preformed spacers, 8 studies described functional articulating spacers and 10 studies described custom-made spacers. The only functional outcome measure used both pre- and postoperatively in at least 1 study per group was the Harris Hip Score (HHS) (31), outcome measures used only pre- or postoperatively were not further analysed.
Group I; prefabricated spacers
A total of 389 patients in 7 studies were treated with 2-stage revision of an infected hip arthroplasty with the use of a prefabricated antibiotic-loaded spacer (9, 17, 19, 21–22–23, 30) In all studies the Spacer-G/Interspace was used. Characteristics of the patients, type of spacer, complications and causative micro-organisms can be found in Tables I–II–III. Re-infection occurred in 4% of patients, resulting in a treatment success rate of 96% (range 80%-98%). Mean interval between the first and second stage procedure was 13 weeks. The second stage procedure was performed in 97% of originally included patients. Mean preoperative HHS was 28, which improved to 84 postoperatively after the second stage (22, 23).
Complications
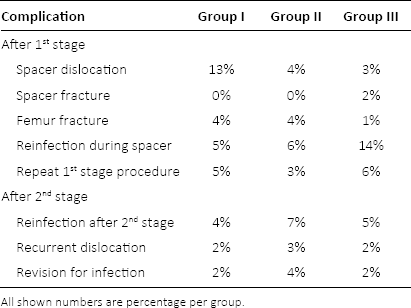
All shown numbers are percentage per group.
Bacteria isolated at first stage procedure

Group II; functional spacers
A total of 527 patients in 8 studies were treated with 2-stage revision of an infected hip arthroplasty with the use of a functional articulating antibiotic-loaded spacer (7, 11, 12, 16, 18, 25, 26, 29). Characteristics of the patients, type of spacer, causative micro-organisms and complications can be found in Tables I–II–III. Reinfection occurred in 7% of patients, resulting in a treatment success rate of 93% (range 76%-100%). Mean interval between the first and second stage procedure was 16 weeks. The second stage procedure was performed in 89% of originally included patients. Patients retaining the functional spacer were not accounted for when calculating time between first and second stage. Mean preoperative HHS was 53, which improved to 90 postoperatively after the second stage (32).
Group III; custom-made spacers
A total of 534 patients in 10 studies underwent 2-stage revision with the use of a custom-made spacer (4, 8, 10, 13–14–15, 20, 24, 27, 28). The study by Hsieh et al (14) describes 2 groups of patients, which were both included in this study and were analysed separately. In 6 studies prefabricated molds were used, in the other 5 studies spacers were intraoperatively molded by hand. Spacers were enforced by K-wires in 4 studies, by a Küntscher nail in 2 studies, by a rush pin in 2 studies and by a modular head and stem in 1 study. In 2 studies no reinforcement was used. Characteristics of the patients, type of spacer, causative micro-organisms and complications can be found in Tables I–II–III. Reinfection occurred in 5% of patients, resulting in a treatment success rate of 95% (range 86%-100%). Mean interval between the first and second stage procedure was 11 weeks. The second stage procedure was performed in 97% of originally included patients. Mean preoperative HHS was 39, which improved to 81 postoperatively after the second stage (4, 13, 20).
Discussion
The aim of this study was to perform a systematic review of the literature to investigate which type of antibiotic-loaded spacer provides the best outcome in patients treated with 2-stage revision for an infected arthroplasty of the hip. Our first hypothesis was that functional spacers would provide a comparable rate of infection control as compared to custom-made or preformed antibiotic-loaded spacers. Our results show comparable good results for the 3 types of spacers when considering infection control, with control rates ranging between 93% and 96%. Patients receiving antibiotic suppression therapy after 2-stage revision were considered failure of treatment.
Our second hypothesis was that patients treated with a functional spacer would experience a shorter rehabilitation time and better functional results as compared to patients treated with custom-made or preformed antibiotic-loaded spacers. While functional and patient reported outcome after primary THA has extensively been described in literature, functional outcome after revision THA for PJI has scarcely been reported. Of all included studies only 1 study (17) describes postoperative range of motion, no studies report patient satisfaction. The only frequently used outcome measure was the HHS, which showed comparable postoperative scores in all groups. Other outcome measures were used less than twice per group and gave insufficient data to compare between groups of spacers. The original studies did not report on rehabilitation protocols. We had insufficient data to prove or disprove our second hypothesis.
Most complications are evenly distributed among the 3 groups, except for dislocation. The incidence of spacer dislocation is high in the prefabricated spacer group as compared to both other groups (13% vs. 4% and 3% respectively). Although this appears to be a large difference, significance levels could not be calculated, due to heterogeneity of the original data. The difference can be explained by the possibility for the orthopaedic surgeon to adjust functional spacers and custom-made spacers to the situation in an individual patient, considering for instance femoral shaft size, neck length, offset deficiency, acetabular size or bone loss. The prefabricated spacers are only available in a limited number of sizes resulting in overstuffing or instability in some patients, which might lead to spacer dislocation.
Remarkably, in 11% of patients in Group II no second-stage procedure was performed. This high incidence was caused by patients refusing second stage surgery because they were satisfied with the functional result after first stage placement of the functional articulating spacer. Outcome measures and functional results such as walking distance and range of motion were not specifically reported for the group of patients refusing second stage surgery.
There are differences in bacteriology between the 3 groups. Group I contains a high number of culture negative cases, especially in the study by Romanò et al (30). These patients might have a positive influence on the outcome, as infection has not been objectified during primary surgery and bacteria might have been absent in the patients.
A weak point of this study is the lack of quality of evidence. There is an absence of level 1 evidence comparing different kinds of spacers in the 2-staged treatment of PJI of the hip. Functional outcome and patient satisfaction after 1- or 2-stage revision of the infected THA have only scarcely been described and therefore could not be presented in the results. Also, due to the lack of information in and heterogeneity of the original data concerning extent of infection, delay in treatment, virulence and susceptibility of infecting agents, quality of surgical debridement, type and extent of antibacterial treatment, compliance with treatment, type of antibiotic in the spacer cement and timing of second-stage procedure the effect of these factors on outcome could not be analysed. We acknowledge these could be confounding factors.
This study creates a comprehensive overview of the available literature on the use of antibiotic-loaded spacers in 2-stage revision arthroplasty of the infected prosthetic hip joint. With the challenge of an increasing number of infected total hip revisions ahead, there is a need for an evidence based approach to the treatment of PJI after THA. Literature comparing functional outcome between various spacers in 2-stage revision of the hip is absent. Various studies have investigated the outcome of 1-stage versus 2-stage revision arthroplasty (6) or difference in outcome of 2-stage revision with the use of different types of spacers including cement beads and Girdlestone procedures (5, 15, 33–34–35–36). None of these studies have described functional outcome after revision arthroplasty of infected total hip arthroplasty.
Functional spacers may improve the congruence of the joint compared to preformed spacers, but up to date there have been no reports investigating whether clinical performance during and after 2-stage revision is better with a functional spacer.
The international consensus meeting (3) concerning periprosthetic joint infections organised in 2013 resulted in the following statements: (i) the type of spacer does not influence the rate of infection eradication in 2-stage exchange arthroplasty of the hip; (ii) a period of antibiotic therapy of 2 to 6 weeks after removal of the infected implant is recommended; (iii) there is no definitive evidence in the literature as to the optimal time interval between the 2 stages, reports vary from 2 weeks to several months. As could be expected after reading the recommendations from the international consensus meeting, we have found a large variety in treatment protocols described in literature.
Research should focus on finding the preferred type of treatment and type of spacer to combine a high success rate of infection treatment with a good functional and patient reported outcome. There is a need for a large, prospective study evaluating patient satisfaction and functional outcome after 2-stage revision hip arthroplasty comparing various kinds of antibiotic-loaded spacers. Secondly, research should focus on the optimal timing of the second-stage procedure (37).
Functional articulating spacers achieve a comparable rate of infection eradication in the treatment of periprosthetic hip joint infections as compared to preformed or custom-made antibiotic-loaded spacers. There is insufficient evidence concerning rehabilitation and functional outcome after 2-stage revision hip arthroplasty to advocate or discourage the use of either kind of interval spacer.
Appendix 1
A search term with Boolean operators was constructed: ((spacer[all fields] OR two-stage[all fields]) AND (((“hip”[MeSH Terms] OR “hip”[All Fields]) AND (“arthroplasty”[MeSH Terms] OR “arthroplasty”[All Fields])) OR (“arthroplasty, replacement, hip”[MeSH Terms] OR (“arthroplasty”[All Fields] AND “replacement”[All Fields] AND “hip”[All Fields]) OR “hip replacement arthroplasty”[All Fields] OR (“total”[All Fields] AND “hip”[All Fields] AND “replacement”[All Fields]) OR “total hip replacement”[All Fields]))) AND ((“infection”[MeSH Terms] OR “infection”[tiab] OR “infections”[tiab]) OR (revision[All Fields] AND (“hip”[MeSH Terms] OR “hip”[All Fields]))).
Footnotes
Financial support: None.
Conflict of interest: None.