
Abstract
Introduction
Femoroacetabular impingement (FAI) has been proposed as a possible cause of early osteoarthritis of the hip. The treatment of this condition and its related lesions can be performed by 3 methods: surgical dislocation of the hip; pure arthroscopic; and anterior mini-open technique with or without arthroscopic assistance.
Methods
We describe the anterior mini-open technique and report our experience over the last decade in the treatment of FAI and different associated pathologies of the hip.
Results
This technique was found to be safe and reliable, allowing tissue preservation and providing a clinical improvement similar to the purely arthroscopic-treated patient, even in complex cases.
Discussions
According to our experience there are several presentations of FAI and associated hip conditions, where other authors advocate surgical dislocation, which can be conducted through a mini-open approach when increased surgical skills are reached. Moreover, this technique was found to be useful as an additional tool to consider, even for surgeons involved in the arthroscopic learning curve.
Introduction
Femoroacetabular impingement (FAI), defined as a conflict between anterior femoral head-neck junction and anterior acetabular rim, has been proposed as a possible cause of early osteoarthritis of the hip (1-2-3). The treatment of this condition and its related lesions can be performed by 3 methods: surgical dislocation of the hip (4), pure arthroscopic (5-6-7-8), and anterior mini-open technique with or without arthroscopic assistance (9-10-11-12-13-14-15-16-17).
We report our experience over the last decade with the anterior mini-open approach in 845 cases operated between 2003 and 2014 in the treatment of FAI and different associated pathologies of the hip. This technique was found to be safe and reliable, allowing tissular preservation and providing a clinical improvement similar to purely arthroscopic treated patient even in complex cases, as reported in other studies (9, 11, 12, 15, 17). The first description of this anterior approach can be attributed to Carl Hueter (18).
The mini-open anterior approach takes advantage of an interneural and intermuscular approach, with features of notable importance:
Compared to pure hip arthroscopic, the mini-open approach avoids excessive traction of the lower extremity, minimising the risks of potential neural damage (19-20-21);
There is no need to perform either hip dislocation or trochanteric osteotomy. If necessary, the hip can be dislocated by detaching the upper insertion of tensor fascia lata (22);
During the procedure there is a permanent view directly from the external to the internal compartment of the hip, with an improved view of the internal compartment if arthroscopic technique is associated (23);
With proper instrumentation and different femoral rotations, an extended exposure of head-neck junction and acetabular rim can be obtained (23, 24);
High accuracy in femoroacetabular reshaping can be obtained, with reduced radiological assistance (23-24-25);
With increased surgical skills, other and more complex conditions as coxa profunda, big labral cysts, moderate sequelae of slipped capital femoral epiphysis (SCFE) or Perthes disease, acetabular stress fractures, acetabular and femoral subchondral cysts, whole labrum allogenic transplantations, rectus anterioris pathology, heterotopic ossifications, among others, can be treated (26);
There is no real need for permanent image intensifier use to control the femoral head-neck junction osteoplasty. When compared with arthroscopic technique, limited use of image intensifier is needed (24);
This approach can constitute a part of other associated techniques as periacetabular osteotomy for the treatment of combined dysplasia and FAI (23, 24);
Head-neck junction osteoplasty and acetabular or femoral microfractures or other cartilage repair procedures can be safely performed. Viable chondral acetabular flaps (Beck III to Beck IV) can be safely reattached as subchondral bone is prepared with microfractures (27, 28);
The postoperative management and rehabilitation programme is similar to the arthroscopic technique (29).
Methods
An extended cohort of 296 patients operated between 2003 and 2008 (mean follow-up 8.7 years) was analysed, based on a previous published study group (30).
Indications for surgery were mostly FAI cases (Figs. 1, 2), with extended indication over the years to other associated and more complex conditions of the hip:
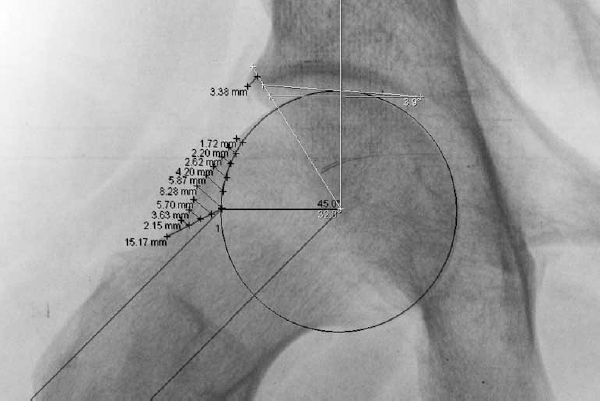
Preoperative planning of a FAI case on a Dunn x-ray view.
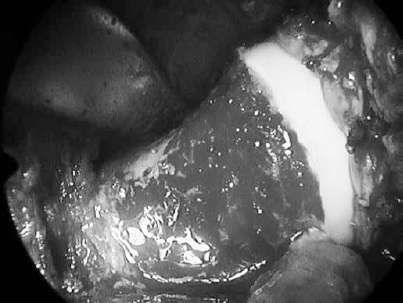
Postoperative result after labral reattachment and femoral osteoplasty.
complex presentations of FAI (combined patterns)
pronounced anterolateral femoral abutments
coxa retroversa minor, coxa profunda, extended Pincer deformity, hip dysplasia
labral reconstruction or transplantation (Fig. 5), acetabular stress fractures
Rectus anterioris and anterior inferior iliac spine pathology
Revision cases (hipocorrection, adherencial syndrome)
Broken hardware removal during arthroscopic technique
Other conditions: synovial chondromatosis, synovectomy, capsular redondance, benign bone tumours, heterotopic ossifications.

Dunn x-ray view of a 30-year-old man with a big cam deformity as SCFE sequelae, treated 20 years before by in situ pinning.

3 years postoperative result after osteoplasty performed by anterior approach. The pin was left in situ (BIPE = bipedestation).
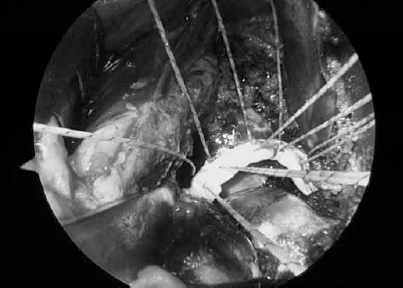
A case of labral transplantation. Note the labrum charged on 6 transosseous sutures.
The Merle D'Aubigné score (31), the Western Ontario and McMaster Universities (WOMAC) osteoarthritis index (32) and the University of California Los Angeles (UCLA) activity level were assessed pre-operatively and at the latest follow-up. Alpha angle and the Wiberg angle were assessed on plain x-ray preoperatively and postoperatively (33). A Kaplan–Meier survivorship curve was established considering as endpoint either a loss to follow-up or a conversion to total hip replacement. The chi-squared and Wilcoxon tests were used for comparisons between groups according to preoperative Tönnis (0-1-2) radiological stage (statistical significance set as p<0.001).
Surgical technique (14, 16, 17)
Preoperative planning is mandatory and routinely performed: a fail to plan is a plan to fail (Fig. 1). The patient is placed in a supine position in an extension table without traction. Skin incision begins 1 cm below and 1 cm lateral to the anterosuperior iliac spine. It runs 4 to 8 cm distally towards the peroneal head. Both fascias cruralis and that of the muscle tensor fascia lata (TFL) are then opened approximately 1 cm lateral to first fibres of TFL, to protect the posterior branches of the lateral femorocutaneous nerve. A curved blunt Hohmann retractor is introduced laterally over the upper part of the capsule and a straight Hohmann retractor is placed medially over the femoral neck. Capsulotomy is performed along the neck from distal to cranial in a T-shape following the acetabular rim orientation. Then 2 blunt curved Hohmann retractors are located into the joint around the femoral neck. The impingement manoeuver should be clearly tested. Extension is applied for hip distraction. Acetabular chondral and labral lesions can be inspected. On the femoral side, lesions can be directly identified. Acetabular osteoplasty and labral repair could then be performed, as cartilage repair procedures. Once acetabular surgery is performed, extension is released. Then, femoral osteoplasty is performed, according to preoperative planning and following a sequential order of combined femoral manoeuvers according to “the hip spaces rule” previously described (24). Pulse-lavage is used during all procedure to avoid heterotopic ossification. Final fluoroscope view is recommended after bone resection is completed to check the osteoplasty. Finally, femoroacetabular clearance and range of movement are tested. Closure of the capsule is routinely performed. Soft-tissue planes are reinserted in full extension of the hip to avoid capsular retraction.
Results
A mean improvement was observed in the Merle D'Aubigné score (15.7 preoperatively to 17.4 at final follow-up), WOMAC (from 59.7 to 93.3) and UCLA activity level (from 7.3 to 8.7), and were all statistically significant (p<0.001). Survivorship at mean follow-up for all patients was 88.8%; it was 98.8% for Tönnis 0 patients, 92.8% for Tönnis 1 patients and 62.3% in Tönnis 2 patients (p<0.001). Alpha angle was significantly restored after osteoplasty (Figs. 2, 4). The most frequent complication was a temporary pathology of posterior branches of the lateral femoral cutaneous nerve, with an incidence of 5.5% (24).
Discussion
Different authors have reported results with the mini-open technique in retrospective studies (14, 16, 17, 23, 24, 29, 34-35-36) with a global success rate ranges from 71% to 92%, with all different preoperative degenerative stages (from Tönnis 0 to Tönnis 2) taken into account.
In a level-III study (24) a clear statistically significant difference was found between the clinical and functional results between Tönnis 0, Tönnis 1, and Tönnis 2 patients. These results have been confirmed in the midterm (37).
Regarding complications, in a meta-analysis by Matsuda et al (29) were recorded 1 fracture of the femoral neck and 2 cases of deep infection, with an incidence similar to purely arthroscopic treatment of FAI. No cases of osteonecrosis have been reported. The most frequent complication arising from the mini-open procedure was related to temporary problems with posterior branches of the lateral femoral cutaneous nerve, with incidences ranging from 0% to 17.1%. Although arthroscopic treatment of FAI gained acceptance worldwide (38-39-40-41-42-43), unsuccessful clinical results have been related to early stages in the learning curve. The most common complication is an incomplete resection and reshaping of bony deformities (44-45-46). In a cadaveric study comparing arthroscopic versus open femoral osteoplasty, Mardones et al (47) showed a tendency to under-correction at the most distal and posterior head neck junction with arthroscopic technique. Surgical dislocation adds the risk of problems related to trochanteric osteotomy, whereas the mini-open procedure has the risk of lesion the posterior branch of lateral femoral cutaneous nerve. Our rate of complication diminished from 17.1% (14) to 5.5% (24, 37) by performing a lateralised incision of the fascia of the tensor fascia lata.
Regarding clinical and functional results, there is no consensus about which technique provides better results (29, 44). Several studies have demonstrated that patients with symptomatic FAI presenting in early changes of hip osteoarthritis (Tönnis 0 or Tönnis 1) may benefit from surgical treatment through a mini-open approach, allowing patients to obtain a significant clinical and functional improvement (23, 24, 43, 44), even in elite sportsmen involved in high-level competitions with an outcome comparable with open and arthroscopic treated patients (14, 24, 48).
Conclusion
In conclusion, in our experience over the last decade, the mini-open anterior approach for FAI has represented a reliable and reproducible technique, allowing a direct view of femoroacetabular deformities present in FAI. The clinical and functional results will depend directly on the joint degenerative stage and early diagnosis.
The access and visualisation available lead the surgeon to a better understanding of the underlying pathomorphologies and associated lesions of FAI, and improve the learning curve associated with the arthroscopic management. We agree with other authors regarding the utility of this technique as a tool to be introduced in the field of hip arthroscopy, shortening the extensive learning curve with its price of unsuccessful results (29, 49).
According to our experience there are several presentations of FAI and associated lesions, where other authors advocate surgical dislocation, which can be solved through a mini-open approach when increased surgical skills are reached. This would provide an immediate and intensive rehabilitation and postoperative management, comparable to that achieved with arthroscopic technique.
Footnotes
Financial support: None.
Conflict of interest: None.