
Abstract
Introduction
There is widespread trend in total hip replacement to limit soft tissue damage. New approaches that respect the capsule and ligaments has been recently reported. The potential advantages of this approach is to improve short-term results in terms of stability, pain, length of stay, transfusions and complications.
Methods
From October 2015 to March 2016 the two senior authors performed 21 hips using the Superpath® technique, the measured variables included age, sex, operative time, acetabular inclination, pain assessment using visual analogue scale at 24 hours, need for transfusion, length of stay and complications. Surgical technique is described.
Results
10 women and 11 men with a mean age of 56.57 (35-74) years. Average operating time was 102.85 (80-130) minutes. The mean acetabular inclination was 44.05 (26-60) degrees. The visual analogue scale (VAS) at 24 hours of the procedure was 2.38, standard deviation (SD) 0.9. The length of stay was on average 4.04 days 1.4 days shorter when compared with a cohort of patients treated using standard posterolateral. All patients were discharged to home. Two patients required transfusion, and in one patient with a calcar crack, crutches for 8 weeks were instructed. No patients were readmitted.
Discussion
The new generation of hip approaches have a strong anatomical basis, hip capsule preservation is a revolutionary concept, it ensures anatomical restoration, length and offset near to native joint. The Superpath® potentially minimises morbidity, reducing transfusion rates, allowing rapid recovery, shortening hospital stay and could save a significant cost to the healthcare system.
Keywords
Introduction
The last 20 years of history in prosthetic joint replacement have witnessed several methods to match the good long-term results of total hip arthroplasty while decreasing soft tissue and bony parts damage. The choice of surgical approaches are dependent on several factors that are due to the influences of surgeon training, trends within hospitals and even regional or geographical trends. Regardless of the approach, there is widespread tend in reduced muscular dissection and minor damage to soft tissue. New approaches that respect anatomical stabilisation structures like the articular capsule and ligaments have recently been reported (1). The potential advantages of this approach are to improve short-term results in terms of stability, pain, length of stay, transfusions and complications. The disadvantages cited traditionally for minimally invasive techniques are grouped into those related to the learning curve because of the difficulty in execution and the potential complications due to wrong position of the final implants; specific procedure material cost has also been pointed out as a drawback.
Since the first publication of the technique in 2011 (2), the supercapsular percutaneously assisted total hip (Superparth®) has expanded throughout North America and Europe. The philosophy of this technique is the use of the interval between the gluteus minimus and piriformis, accessing the capsule from its top and preparing the femur without dislocating the femoral head, reaming the acetabulum through an accessory portal, preserving capsular attachments and maintaining integrity of the external rotators. The Superpath® technique borrows elements from two previously developed and proven techniques the Path® and the SuperCap®, that have over 12 years of history (2-3-4). This family of posterior access can be seen as a continuum where it is possible for the surgeon intra operatively move from micro to mini incision and thence to conventional posterolateral approach (1); this greatly eases the pressure about the learning curve and prevents compromises in components placement due to an uncomfortable approach or lack of adequate visualisation of surgical field.
Methods
From October 2015 to March 2016 the two senior authors performed 21 hips using the Superpath® technique. The training for this technique was conducted in 2 cadaver laboratory sessions led by experts. The measured variables included age, sex, operative time, acetabular inclination, pain assessment using visual analog scale at 24 hours, need for transfusion, length of stay and complications.
Patient selection
Patients included in this first group are adults with non-inflammatory joint disease, candidates for uncemented total hip arthroplasty with a radiograph showing enough space, more than 3 cm, between the tip of the greater trochanter and the most lateral part of the acetabular rim in the AP pelvis. We excluded patients with general conditions that contraindicate a standard primary total hip arthroplasty (i.e. active infection). Patients over 100 kg, BMI >40 or protrusio acetabuli were also excluded.
Pre-op planning
Planning has been made using digital software on calibrated AP pelvis radiographs, the size of the PROFEMUR L stem and PROCOTYLE L cup as well the distance from the tip of the greater trochanter to the implant shoulder was measured in order to predict the depth of insertion of the broach in the femoral canal.
Operative technique
Procedure requires a team consisting of a surgeon, an assistant and a nurse. The patient is placed on conventional table, in lateral decubitus with the affected limb letting the foot rest on a padded Mayo stand and raised about 20 cm from the level of the operative table (Fig. 1). The hip is flexed about 50°, knee falls maintaining an internal rotation of the hip of about 20°. This position places the axis of the femoral neck vertically and opens the posterior hip space where dissection will be carried out.

Home position for SuperPATH® technique. Lateral decubitus with the affected leg with foot resting on a padded Mayo table, surgeon stand at the patient's back and assistant at front. The posterosuperior area is easily exposed without tearing any structure avoiding unnecessary leg manipulation at unnatural positions.
The incision is made in the axis of the shaft of the femur with a length of about 6-7 cm extending proximally from the tip of the greater trochanter. The subcutaneous tissue is dissected down to the fascia of the gluteus maximus which is opened in the same direction of skin incision. Blunt dissection of the gluteus maximus is done respecting the arrangement of the fibers and progressing down to the bursa between the gluteus medius and minimus over the hip external rotators, a blunt Hohmann protects the gluteus medius. Dissection proceeds to identify the piriformis tendon which is elevated from the capsule to place another blunt Hohmann posteriorly. The abduction movement relaxes external rotators to facilitate this maneuver, the gluteus minimus is discreetly mobilised anteriorly without fully detaching it from the capsule; this gives access to the upper region of the capsule which is opened over the axis of the neck from the acetabular rim to the base. It is optional to resect a longitudinal band of 5-7 mm width instead of longitudinal capsulotomy to prevent over tensioning and tearing of the capsular attachments during the procedure. The superior labrum, the femoral head and neck are exposed. Blunt retractors can be placed now intra-articular helping with an abduction movement.
Femur preparation is carried out “in situ” by keeping the femoral head in the acetabulum without dislocate the joint, the introduction of the broaches is analogous to the use of an intramedullary nail. The base of the neck is located and a sharp starter reamer is introduced, followed by a blunt larger diameter reamer and a lateralise reamer working on the inner part of the lateral cortex, an oval or round chisel is used to create a trench in the middle of the head, a toothed spoon is used to remove cancellous bone and expose the calcar, to avoid undersizing. Broaches are introduced sequentially according to plan until resistance is noted, stability must be confirmed and distances from the tip of the trochanter to the shoulder of the stem according to pre-op planning should be equal, fluoroscopy verify the position of the stem (Fig. 2).

Fluoroscopy check for broach position. According to pre-op planning femoral preparation goes similar to an endomedullary nail. Head remains inside acetabulum.
The osteotomy is performed over the neck of the broach, knee-lifting movement makes this step easier and aids to ensure a complete cut. The removal of the head is performed either using Schanz pins (Fig. 3) rotating the fragment or using a corkscrew. In more complex cases where a powerful ligament persists or in a deep acetabulum case, it might be necessary to divide the head into small fragments.
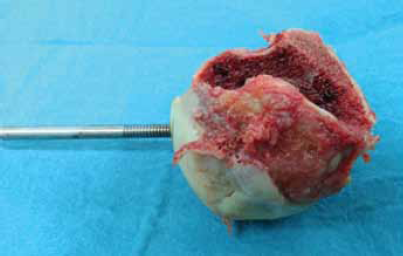
Femoral head extraction. After neck osteotomy, a Schanz pin is placed on head and rotated caudally, a second Schanz is placed repeating the maneuver until ligamentum teres is sectioned. Traction is applied on both Schanz to extract the head, notice the trench along the longitudinal axis of the head, necessary to broach the femoral canal.
Spiked Hohmanns are placed in the anterior and posterior capsulolabral recesses, the remaining labrum is resected. Using an external guide, a portal that communicates a more distal and posterior incision with the acetabulum is established. The cannula is held in place, acetabulum basket reamers are introduced sequentially through the main incision and connected with the reamer drive shaft through the percutaneous cannula (Fig. 4), reaming is performed until get the right size and stability, cup is inserted and impacted first from above with a vectorial handle impactor and then with a straight cup impactor through the accessory portal, the orientation of the acetabulum should follow native anatomical position except severe anatomical deformity. Cup screws, if necessary, could be inserted through the portal cannula. The trial liner is placed and the femur is mobilised in internal rotation and adduction while the assistant pushes from knee bringing the neck to the surgical field; the trial head is placed within the cup and the trial neck attached to the broach, the reduction is carried out controlling rotation and telescoping to attach the components in situ. Component position is checked with C-arm and length, range of motion and stability by the surgeon. Uncouple the head and neck require using a lever mechanism which interacts with the lifting hook in contact with broach and pointed rod engaged in the trial neck. The final components are coupled in situ according to the same initial reduction technique combining rotation, abduction and translation of the femur. The capsule is closed (Fig. 5) at the top, superficial layers are approximated using the usual technique.

Acetabular preparation through accessory portal. (

Capsular closure. The image at the left shows supercapsular capsulotomy, ceramic head and neck can be seen intracapsullary. Image at right shows anatomically closed capsule with noncontinuous suture.
Postoperative
The multimodal analgesia protocol includes periarticular injections, intravenous opioids on first 24 hours. Then oral analgesic regimen with paracetamol, nonsteroidal anti-inflammatory drugs (NSAIDs) and weak opioids for unexpected pain rises. AP pelvic radiograph is performed immediately after. Walking on crutches within the first 24 hours is allowed. There are no special restrictions besides those coming from pain, patients can sleep on the affected side if pain permits. Stiches are removed after two weeks and usually we recommend, if possible, to cease the first crutch after this appointment. Successive checks of patient, extremity and wound (Fig. 6) were conducted at 6, 12 weeks, 6 months.

Surgical scar. Right side SuperPATH® hip. Wound at 10 weeks in a patient with BMI of 36. Notice proximal scar in line with femur and accessory portal.
Results
This initial group of patients consisted of 10 women and 11 men with a mean age of 56.57 (35-74) years with a follow-up time of 6 months. The average operating time was 102.85 (80-130) mins. The mean acetabular inclination measurement using ischial tuberosity as baseline was 44.05° (26°-60°). The mean visual analogue scale (VAS) at 24 hours of the procedure was 2.38 (1, 2, 5-6-7). The length of stay was on average 4.04 days, 1.4 days lower when compared with a cohort of patients treated using standard posterolateral in our centre. All patients were discharged directly to home. Two patients required transfusion of blood products. In one patient with a calcar crack, crutches for 8 weeks were instructed. No patients were readmitted.
Discussion
Although treatment of osteoarthritis by means of traditional approach total hip arthroplasty is confirmed as an effective, safe procedure with a high rate of excellent results, there is still room to make this a more efficient treatment, less costly and less invasive for the patient (5). In past decades attempts to minimise soft tissue injury and wound size had no universal acceptance among surgeons, but certainly have helped move from large incisions with maximum exposure to limited incisions in size without compromising the proper placement of implants. The new generation of hip approaches have a deeper anatomical basis, hip capsule preservation is a revolutionary concept, although it has the ability in most cases to heal and restructure, occasionally it originates a defect with the formation of atypical pseudocapsule, the structural preservation of the capsule ensures anatomical restoration, length and offset near to native joint, similarly the prosthetic components can be placed with a more anatomical position since the capsular integrity limits instability peaks moments. There is great controversy about “the safe area”; dislocation events that occur within this area, clearly demostrates the multifactorial nature of joint instability. The importance of the soft tissue is reinforced when analysing the importance of preservation beyond prosthetic surgery; i.e. the treatment of femoroacetabular impingement (FAI) in our days is considered arthroscopic, osteochondroplasty with labral and capsular repair as the gold standard, once again, soft tissue and capsule preservation has a leading role for good results.
Another problem associated with early techniques of hip mini incisions was the extensibility of the approach, with Superpath® it is possible to distally extend incision and dissection to a standard posterolateral approach, just in case component position its compromised during the learning curve. Other studies have suggested Superpath® consistency in the placement of the implants even during the learning curve (1), being the cup abducted at 39° ± 8.4° (6).
Although there are no long-term studies with the use of this technique, it is reasonable to think that consistent positioning of the components and preserving largely all anatomical structures will at least match in the long term those of conventional arthroplasty.
The Superpath® potentially minimises morbidity of procedure reducing the need for transfusion and allowing rapid recovery, shorter hospital stay and could save a significant cost to the healthcare system (7).
Footnotes
Financial Support: None.
Conflict of Interest: None.