
Abstract
Background
Bone impaction grafting is a biologically and mechanically appealing option in acetabular revision surgery, allowing restitution of the bone stock and restoration of the biomechanics. We analysed differences in proximal migration of the revision acetabular components when bone impaction grafting is used together with a cemented or an uncemented cup.
Patients and Methods
43 patients (47 hips), revised due to acetabular loosening and judged to have less than 50% host bone-implant contact were included. The hips were randomised to either an uncemented (n = 20) or a cemented (n = 27) revision cup. Radiostereometry and radiography was performed postoperatively, at 3 and 6 months, 1, 2, 3, 5, 7, 10 and 13 and 17 years postoperatively. Clinical follow-up was performed at 1, 2 and 5 years postoperatively and thereafter at the same interval as in the radiographic follow-up.
Results
here were no differences in the base line demographic data between the 2 groups. At the last follow-up (17 years) 14 hips (10 cemented, 4 uncemented) had been re-revised due to loosening. 3 additional cups (1 uncemented and 2 cemented) were radiographically loose. There was a higher early proximal migration in the cemented cups.
Discussion
Cups operated on with cement showed a higher early migration measured with RSA and also a higher number of late revisions. The reason for this is not known, but factors such as inclusion of cases with severe bone defects, use of smaller bone chips and issues related to the impaction technique might have had various degrees of influence.
Introduction
Bone defects in acetabular revision surgery may be addressed with different approaches (1–5). Re-cementing a loose cup or stem without any additional bone grafting was commonly used until the mid-1980s (6). High failure rates using this technique (16% to 48% at 4.5 to 11.9 years) (7–9) and a belief that the cement itself had a destructive effect on the bone tissue (10) encouraged the use of uncemented fixation in hip revision surgery (11–13). During the 1990s several authors reported inferior survival when uncemented fixation was used in acetabular revisions with significant bone loss (14–16). An alternative technique based on cemented fixation with impaction bone grafting using morsellised bone allograft was introduced more than 3 decades ago. There are several reports with favourable long term results when this technique has been used (5, 17–20).
In 1993 we initiated a study intended to compare the clinical outcome and RSA migration pattern of acetabular components in patients with poor host bone-implant contact revised with either an uncemented or a cemented cup. Morsellised bone allograft was used in all patients.
Patients and Methods
Between June 1993 and December 1997 all acetabular revisions in patients less than 80 years of age operated on at our hospital (n = 117) were offered the chance to participate in this study. 82 patients (90 hips) were eligible and agreed to participate (Fig. 1). Pre-Operative radiograph of all cases were assessed pre-operatively. The amount of vital host bone was estimated by at least 2 consultant surgeons with experience in revision surgery. 43 patients (47 hips, 4 patients were revised bilaterally) with less than 50% vital host bone consented to participate (Fig. 1). The recruitment to this study was stopped when we changed our impaction technique to the use of larger bone chips and discontinued the reverse reaming technique. The most common index diagnosis was primary osteoarthritis (n = 19) followed by rheumatic diseases (n = 10), avascular necrosis (n = 8), sequels after childhood disease (n = 5), osteoarthritis secondary to trauma (n = 5) and osteoarthritis associated with alkaptonuria (n = 1). The mean age of the patients was 59 (33-79) years; there were 27 women. End-point for the study was re-revision of the acetabular component due to aseptic loosening (n = 14) or radiographic loosening (n = 3).
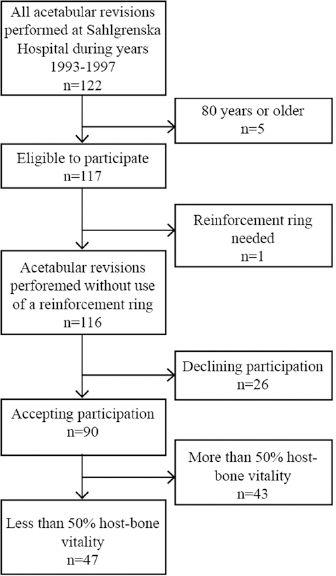
Patient selection flowchart.
Classification and choice of implant
Randomisation to an uncemented (n = 20) or a cemented cup (n = 27) was performed using a software program (Pocock SJ. Clinical trials: a practical approach. New York: Wiley; 1983). In the uncemented group either a Harris Galante II cup (Zimmer) (n = 16) or a multi-hole Trilogy cup (Zimmer) (n = 4) was inserted. The change of the uncemented cup design to the Trilogy design was made due to the inferior liner locking mechanism in the Harris Galante cup. In the remaining 27 hips a cemented cup was used. In 24 hips this was a Reflection cup (Smith & Nephew), noncrosslinked and gas sterilised and in 3 hips, with a well-fixed non modular Charnley stem, a Charnley Ogee cup (DePuy Intl. Ltd.) was used. After the operation the surgeon completed a standardised form to account for the type of bone defect according to Gustilo Pasternak (21) before and after the reaming of the acetabulum. The volume of transplanted bone and the estimated contact between living bone and the implant or the cement were recorded (Tab. I).
Demography and surgical intervention
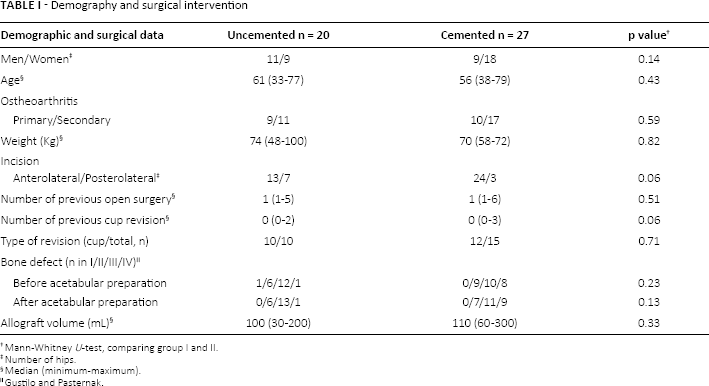
Mann-Whitney U-test, comparing group I and II.
Number of hips.
Median (minimum-maximum).
Gustilo and Pasternak.
Surgical technique
2 surgeons performed 45 of the revisions and the remaining 2 operations were performed by 2 other surgeons. A direct lateral incision was used in 12 and 23 hips in the uncemented and the cemented group respectively. Trochanteric osteotomy was performed in 1 case in each group. The remaining 7 and 3 revisions were performed through a posterolateral incision. Milled frozen femoral heads were used for bone grafting in all cases. At this time, we used an air powered mill (Synthes-Stratec) or a Tracer mill, (Ossano), which both produce comparatively small bone chips. Polished spherical impactors and the reversed reaming technique were applied for impaction of the graft. Bulk allografts were used in 1 uncemented and 1 cemented revision. In the uncemented cases under reaming by 1-2 mm were applied.
In all uncemented revisions 3-5 screws were used in order to maximise primary fixation. In the cemented group a mesh was used in 4 cases to cover a major medial bony defect. 8-10 tantalum markers (Ø = 0.8 mm) were inserted into the periacetabular bone and another 8-10 markers (Ø = 1 mm) into the cup or the liner. Partial weight-bearing was recommended for 3 months postoperatively.
Conventional radiography
Anteroposterior, cross-table lateral and pelvic radiographs were obtained postoperatively (1-7 days), 3 and 6 months and 1, 2, 3, 5, 7, 10, 13 and 17 years after surgery. Due to the introduction of digital radiographic techniques and a failure to scan old analogue roentgen films, a complete sequence of radiographic examinations was not available at the time of the present evaluation in 6 hips. These 6 patients died 2 to 8 years after the index revision and none was re-revised. For the remaining 41 cases the radiographic examination performed at the last follow-up was assessed. Evaluation of the bone-implant interface was performed on both the AP and lateral view according to the classification described by Hultmark et al (22). The extension of radiolucent lines was measured as the percentage of each region (1–6), divided into 4 groups corresponding to 0, 0-49, 50-99 and 100 per cent radiolucency between implant and bone (groups 0-3). The cup was classified as loose if there was a complete zone (100%) on the AP or the lateral view or both.
Radiostereometry
Radiostereometry was performed with the patient supine, at the same interval as the radiographic examinations. The Uniplanar technique with the calibration cage positioned under the examination table (23, 24) was used. The rotation and translation of the cup in relation to the 3 cardinal axes was analysed. The UmRSA system (RSA Biomedical) was used for all measurements and calculations. Until 1997 the stereoradiographs were measured manually on a digitising table. At that time we changed to a digitised system, with higher precision (25).
Complete evaluation including rotations and translations was done if at least 3 well-defined markers could be identified with a scatter corresponding to a condition number less than 125 and a marker stability corresponding to at most 0.36 mm (24). 3 patients had unstable or poorly visualised RSA markers, preventing accurate measurements being taken at the last available RSA examination. These cases had at least 3 markers identified in the acetabulum. The proximal cup translation was computed either as the average value of 2 markers, 1 on the medial and 1 on the lateral side of the cup or using model based RSA measurement of the cup (26). The model based technique used in uncemented cups, was evaluated by analysing the proximal migration at 1 year, measured with the use of tantalum markers in the cup and using the model based technique, in 15 randomly selected uncemented cups. Comparison between the 2 methods in a linear regression model revealed an adjusted r-square of 0.99. The error of the RSA measurements, based on measurements of implant and bone markers was analysed in 20 double examinations. The 95% detection limit for rotation about the horizontal, longitudinal and sagittal axes was 0.45, 0.53 and 0.28 degrees respectively. The corresponding values concerning medial/lateral, proximal/distal and anterior/posterior translation were 0.40, 0.08 and 0.28 mm.
Clinical evaluation
Clinical outcome data was collected prospectively during years 1993-2014. The Harris Hip Score (HHS) (27) was captured. A visual analogue scale (VAS) (0-100 mm) was used to assess patient pain at rest and during physical activity (28). The clinical data were recorded pre-operatively and at 1, 2, 3, 5, 7, 10, 13 and 17 years after surgery. Due to digitalisation of the medical charts during the study period we were not able to retrieve all the data collected (Tab. II). At the last follow-up (17 years), HHS and VAS scores were available in all cases attending the follow-up.
Number of hips with uncemented/cemented cups at each follow-up
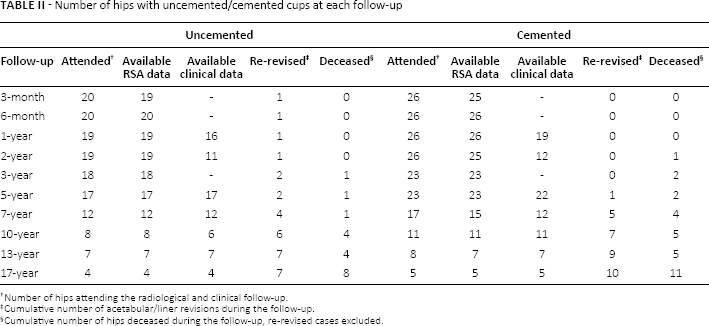
Number of hips attending the radiological and clinical follow-up.
Cumulative number of acetabular/liner revisions during the follow-up.
Cumulative number of hips deceased during the follow-up, re-revised cases excluded.
Statistics
Nonparametric testing was used to compare baseline demographics of patients, differences in clinical outcomes and RSA data measured during the follow-up. Kaplan Meier survival and the Log-rank test were used to calculate and compare the survival at 17 years, and presented as a percentage with standard error (SE).
Results
During the follow-up, 14 hips (4 uncemented, 11 cemented) were re-revised due to aseptic cup loosening. 3 hips (1 uncemented, 2 cemented) were assessed as loose at 3-13 years, 2 patients died before re-revision. The last patient had no symptoms from the revised hip at 13 year follow-up and declined further participation due to restricted mobility after a transfemoral amputation on the contralateral leg. 1 additional patient with deteriorating medical condition was not able to attend the follow-up at 17 years. This patient was contacted by phone: there had been no re-revision and she did not report any disability associated with the revised hip. During the follow-up 3 additional cup or liner revisions (all uncemented) were performed due to femoral loosening, acetabular osteolysis and liner wear respectively, preventing further RSA measurements. 19 patients (19 hips; 8 uncemented, 11 cemented), none re-revised were deceased.
Conventional radiography
On the postoperative radiographs the occurrence of radiolucency did not differ between the 2 groups. At the last available radiograph, complete radiolucent line was observed in 10 hips (2 uncemented and 8 cemented). These 10 cups were classified as radiographically loose. 7 of these cases were re-revised, 2 died before any re-revision and 1 without symptoms had not been revised at the latest follow-up. At the latest follow-up, the extension of radiolucent lines in region IV was more pronounced in the cemented group (p = 0.05). In the other 5 regions the extension of radiolucent lines did not differ between the groups (p≥0.07).
Radiostereometry
Proximal migration was lower in the uncemented group. This difference was statistically significant up to 1 year (p≤0.05, Tab. III). Anteroposterior translation (z) was higher for the uncemented cups at 6 months (p = 0.03). The mean rotation of the cup around the y axis was higher (p = 0.01) for the uncemented group at 6 months and the mean z-rotation was higher (p = 0.04) in the cemented group at 5 years (Tab. III). Proximal migration of the cemented cases tended to increase during follow-up. At 17 years the mean proximal migration in the cemented group reached 2.18 mm (SD 1.42). The corresponding value in the uncemented group was 0.01 mm (SD 0.21) (Fig. 2). In cases subsequently re-revised because of loosening or defined as radiographically loose at the last follow-up, a higher proximal migration was observed compared to the well-fixed group (up to 10 years: p≤0.01; 13 years: p = 0.13) (Fig. 3).
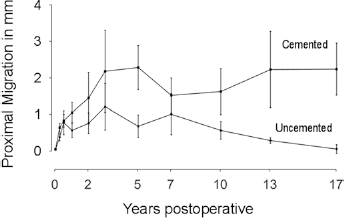
Proximal migration, measured with RSA comparing uncemented and cemented acetabular revisions with bone impaction grafting. The number of observations is presented in Table II.
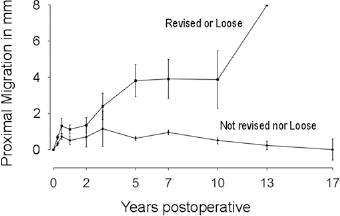
Proximal migration, measured with RSA comparing cups revised because of loosening or radiographically loose cups with cups judged to be radiographically fixed, regardless type of fixation.
RSA measurements at different time points
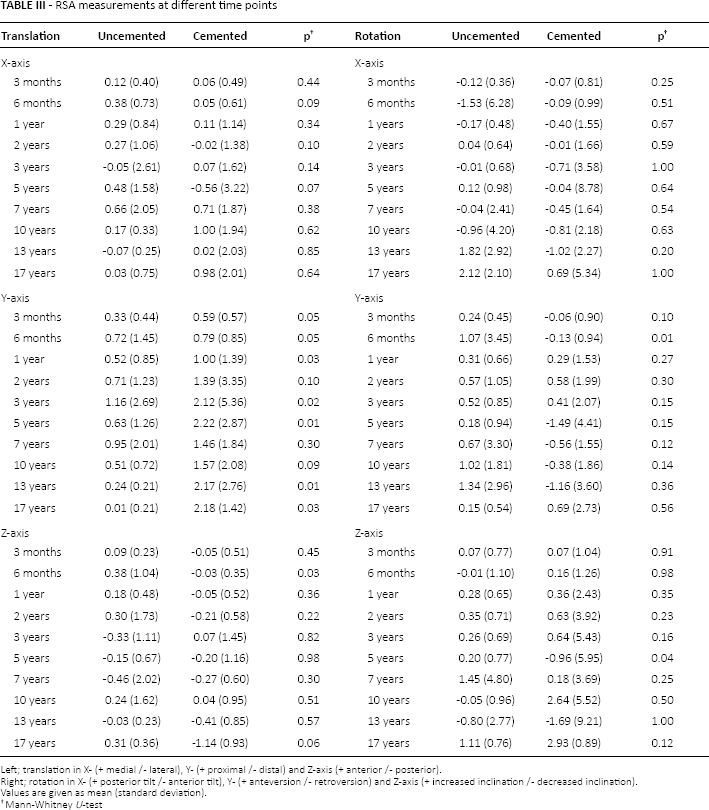
Left; translation in X- (+ medial /- lateral), Y- (+ proximal /- distal) and Z-axis (+ anterior /- posterior).
Right; rotation in X- (+ posterior tilt /- anterior tilt), Y- (+ anteversion /- retroversion) and Z-axis (+ increased inclination /- decreased inclination). Values are given as mean (standard deviation).
Mann-Whitney U-test
Clinical results
Harris hip and pain scores increased from a median of 47 and 20 before the index revision to 83 and 44, respectively, at 1-year follow-up (p<0.001). Pain at rest and during activity had decreased from a median of 0 and 45 before revision to 0 and 0 at 1-year follow-up (p≤0.004) (Tab. IV). There was no difference between the cemented and uncemented cups regarding improvement of the clinical outcome (p≥0.12).
Clinical scores in the uncemented and the cemented group
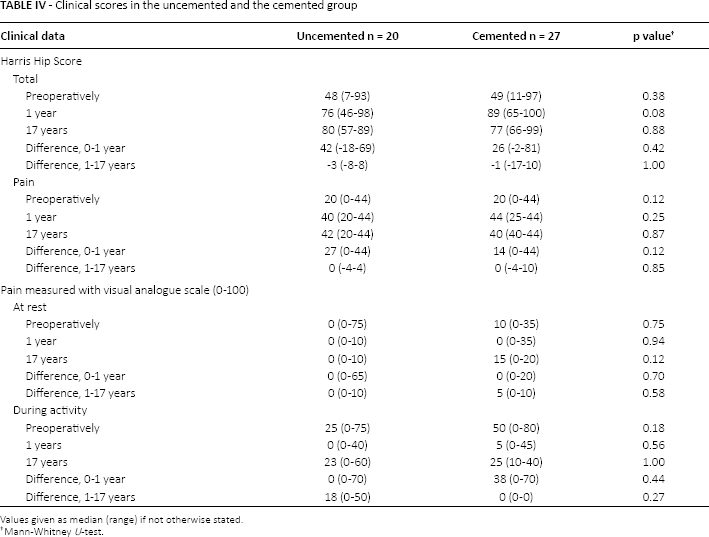
Values given as median (range) if not otherwise stated.
Mann-Whitney U-test.
Cup survival
The survival of the uncemented cups at 17 years with re-revision due to any reason as end-point was 63% (SE: 12%). The corresponding survival for the cemented cups was 46% (SE: 13%). With re-revision due to loosening or radiographic loosening as end-point the survival of the uncemented cups at 17 years was 65% (SE: 12%). The corresponding figure for the cemented sockets was 37% (SE: 12%). There were no statistical differences between the 2 groups (p≥0.15).
Discussion
The primary aim of this prospective study was to evaluate the differences in proximal migration measured with RSA when uncemented and cemented cups are inserted together with bone graft in acetabular revision surgery. According to our data the cemented cups show higher proximal migration.
Schreuer, Slooff and co-workers (5, 17, 18, 20) have repeatedly reported favourable long-term results using impaction bone grafting with cemented technique. Comba et al (29), using the same technique in 142 hips, reported a re-revision rate of 4.2% after a mean of 4.3 years follow-up. Van Haaren et al (30) reported a 35% risk of re-revision at a considerably shorter follow-up. Several authors (11, 31, 32) have reported favourable results using uncemented revision cups with the addition of bone grafting. The medium- and long-term survival rates in these reports vary between 90%-100%. We analysed only hips with major bone defects pre-operatively, and found that the 17-year survival for the uncemented cups was better than when a cemented cup was inserted. However, this difference was not significant, probably due to the limited number of patients in our cohort.
Nivbrant et al (33) followed 60 hips revised with an uncemented Harris Galante cup. Cups requiring morsellised bone grafting (n = 31) migrated significantly more than uncemented sockets operated on without bone grafting. Ornstein (34), analysing cemented cup revisions operated on with impaction grafting, reported a mean proximal migration 4 times higher than Nivbrant (33). Our uncemented cups showed a proximal migration of about the same magnitude as reported by Nivbrant et al, whereas the cemented cups operated on with impaction grafting seemed to migrate less than those reported by Ornstein et al (34). The magnitude of this migration probably mirrors the grafting technique used, including factors such as the quality of donor bone, size of the bone chips and the surgical technique employed to achieve impaction. It could also be argued that in uncemented acetabular revisions the cup reinforced by several screws will have better rim-contact with living bone allowing for better initial stability and limited ingrowth. This could partly explain the lower proximal migration for the uncemented cups in the current study. In a later study (35) we used a cemented Ogee (Thacekery) socket in conjunction with the original impaction technique described by Slooff et al (5) In this study the median proximal migration at 3 years was 0.5 mm, suggesting that better primary fixation is possible than the one achieved with the technique used in current study.
In a recently conducted analysis of 312 acetabular revisions (36) we were able to illustrate a strong correlation between early proximal migration measured with RSA and later risk of aseptic loosening. The lower early migration in our uncemented cases could be interpreted in favour of uncemented fixation, but this hypothesis needs further investigation.
Our study had several limitations. Firstly, different types of bone mills were used. The importance of bone chip size was not recognised during the time period in which the patients were operated on. Secondly, we used the original classification system by Gustilo Pasternak. This classification system does not describe the integrity of the acetabular rim and has since been revised by Raut et al (37). It would have been beneficial to classify the pre-operative bone defects according to a more established bone defect classification system. Unfortunately, we were not able to retrieve the pre-operative radiographs due to a failure in the scanning old analogue roentgen films after the implementation of digital radiographic techniques in the hospital. Thirdly, the inclusion criteria were based on the vitality of bone stock rather than the bone defects described by Gustilo Pasternak. In 2001 Campbell et al (38) evaluated the reliability of 3 different classifications of acetabular bone defects. The authors showed inconsistent reliability for the evaluated classifications. The true size and location of the bony defect, the quality of the graft, the amount of graft used and the final amount of vital bone facing the implant or the cement are probably all factors with a more or less pronounced influence on cup fixation. We therefor believe that assessment of bone defects perioperatively might have advantages compared to only a pre-operative classification of bone defects.
Although there are limitations in our study, conducting a randomised study with 17 years follow-up, including RSA, we are able to conclude that cemented fixation with bone grafting in acetabular revision surgery results in higher proximal migration. Better results for cemented fixation could probably be obtained if bigger graft particles and a more consistent impaction technique had been used. It could also be argued that the increased proximal migration of the cemented acetabular components is due to a different pattern of bone remodelling when cemented fixation is used in conjunction with bone impaction grafting. These hypotheses are beyond the scope of the current analysis but should most certainly be addressed in future studies.
Footnotes
Financial support: Funding was obtained from IngaBritt och Arne Lundberg research foundation and Felix Neubergh research foundation. Conflict of interest: None.