
Abstract
Introduction
The purpose of this study was to compare acetabular cup position for 2 cohorts of total hip arthroplasty (THA) patients who had a direct anterior approach.
Methods
100 THA cases were performed with an anterior approach using intraoperative fluoroscopy (IF) to aid in cup positioning. Another group of 100 cases underwent THA with an anterior approach without the use of any fluoroscopy. Postoperative abduction and anteversion angles were measured using Martell's hip analysis software.
Results
Mean abduction angle was 43.2° (standard deviation (SD) = 4.5°) for the IF group versus 37.5°(SD = 7.4°) for cases without IF (p<0.001). 18% more cases with IF fell within the Lewinnek safe zone (p<0.001); however, a similar number of cases had over 50° of abduction. The mean anteversion angles of the two groups were also significantly different (IF 21.8° vs. 24.9°) (p<0.01).
Conclusions
There was significantly less variation in cup position among the cases using IF with regards to abduction.
Introduction
The direct anterior approach (DAA) is increasingly used as a surgical approach for total hip arthroplasty (THA). It affords an excellent intermuscular exposure to both the acetabulum as well as the proximal femur with the patient in the supine position. Although first described in 1881 by Carl Hueter as a surgical approach to the hip, the popularity of the direct anterior approach has increased in recent years with reports of earlier patient mobilisation, potential for more rapid recovery, and improved hip stability (1-2-3-4). There have been reports of an increased early complication rate and learning curve (5-6-7-8), but many surgeons have reported successful incorporation of this approach into their practice with consistent results and low complication rates (9, 10). Some studies have reported between 20 and 100 procedures as the learning curve for the approach, with complications including improper component position, fracture, and lateral femoral cutaneous nerve palsies that decrease with experience (9, 11, 12).
Patients undergoing hip arthroplasty through the anterior approach are typically placed in the supine position, allowing the surgeon to easily use fluoroscopy for evaluation and adjustment of the femoral and acetabular component position intraoperatively. In studies comparing anterior and posterior approaches, the use of the DAA with fluoroscopy has demonstrated more precise cup placement (13, 14). Other surgeons are performing the DAA without the use of intraoperative fluoroscopy (IF) but place an emphasis on intraoperative evaluation of leg lengths, range of motion, and stability of the hip to ensure appropriate cup placement (15).
Correct acetabular component position is one of many important factors in the success of a hip replacement. The effect of cup abduction and anteversion on the likelihood of dislocation has been reported by Harrison et al (16) and Lewinnek et al (17). Placing the cup too vertically, or too anteverted or retroverted, reduces the distance that the femoral head must travel to dislocate (16-17-18-19). Lewinnek proposed a “safe zone” for cup placement to minimise dislocation risk as 30°-50° of abduction and 5°-25° of anteversion (17). Cup position outside of the target range has also been associated with lack of bony support, edge loading, ceramic squeaking, and increased rates of adverse tissue reaction in metal-on-metal hips (20-21-22-23). Unfortunately, reports have shown that accurate and precise cup positioning can be elusive even for expert surgeons (19). Any adjunct to improve cup positioning may be beneficial to have in a surgeon's armamentarium.
The objective of this study was to compare the postoperative acetabular cup abduction and anteversion angles for 2 cohorts of patients undergoing primary total hip arthroplasty through the DAA with and without the use of intraoperative fluoroscopy. Our hypothesis was that there would be fewer outliers and less variation in cup position among the cases using intraoperative fluoroscopy, because it provides immediate feedback to the surgeon about cup position.
Materials and methods
The protocol was reviewed and approved by the ethics review committee at the institution where the studies were conducted. The procedures followed were in accordance with the ethical standards of the Inova Internal Review Board, national law, and with the Helsinki Declaration of 1975, as revised in 2000 and 2008. Using an institutional database, a retrospective analysis was performed on 2 cohorts of primary THA cases. Each group consisted of 100 consecutive DAA cases, 1 group performed by a surgeon who uses intraoperative fluoroscopy (IF), and the other without the use of fluoroscopy. Having previously performed over a hundred prior hip arthroplasties with the direct anterior approach, the surgeons were beyond the learning curve phase of their respective methods and were experienced in the direct anterior approach.
Patients in the 1st group were positioned in a supine position on a HANA fracture table (Mizuho OSI) for the DAA while the operative leg was extended downward to allow frontal access to the hip joint. Once the joint was exposed and trial components were placed, intraoperative fluoroscopy was used to confirm appropriate positioning of the acetabular component. Fluoroscopy was used during cup impaction, and small adjustments to the cup position were made to place the component in the goal position (Fig. 1). The surgeon's goal was 40° of abduction, with 20° of anteversion. A cementless, hemispheric acetabular cup (Pinnacle, DePuy) was used in all cases.

Fluoroscopy can be used to visualise the cup position intraoperatively.
Patients in the 2nd group were positioned in a supine position with a small support under the pelvis to allow hyperextension of the operative extremity. Upon exposure, the acetabulum was prepared, reamed, and the component impacted using anatomic landmarks for reference. The surgeon's goal was a cup position that created maximum joint stability through a range of motion. A cementless, hemispheric acetabular cup (Trident PSL, Stryker Orthopaedics) was used in all cases. Once stable fixation was achieved with a femoral broach, the hip was reduced with the trial head and neck in place and the joint stability was evaluated. Longitudinal force to assess the amount of hip distraction, also known as the “shuck” test, was applied to assess joint laxity. Finally, the leg was placed into extension and, using the medial malleolus as a reference, the leg length was compared to the nonoperative extremity.
Postoperatively, patients in both groups were allowed to bend their hip freely and bear full weight as tolerated. Their activity was not restricted, and assistive devices were used as needed. Patients returned for a follow-up evaluation and digital radiographs 4 months postoperatively, and radiographs taken at that interval were used for this study. Acetabular cup abduction and anteversion angles were measured on anteroposterior (AP) pelvic radiographs using Martell's Hip Analysis Suite™ software. All AP pelvic radiographs were obtained using a standardised technique with the patient supine, legs internally rotated, and the x-ray beam centered on the pubic symphysis. Angle measurements were evaluated by a single reviewer who was experienced using Martell's software and who was blinded to the study groups. This software has been validated (24) and used by other investigators to measure cup angles (18, 19, 25). Cross table lateral radiographs were viewed to determine if any cups were retroverted. The cup angle measurements were recorded for each case, and the number of cases outside the Lewinnek safe zone was calculated.
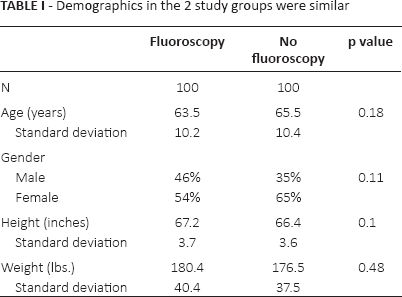
Patient demographic data for each case was obtained retrospectively from a patient database and chart review. In the IF group, average patient age was 63.5 years (standard deviation [SD] 10.2 years), average body mass index (BMI) 28.2. The non-fluoroscopy group average age was 65.5 years (SD 10.4 years) and average BMI 28.6. The groups did not differ statistically with regard to age, height, weight, or BMI as shown in Table I. The gender distribution was also similar in both groups with 54% females in the fluoroscopy group and 65% females in the non-fluoroscopy group (p = 0.11).
Demographics in the 2 study groups were similar
Descriptive statistics such as means of angles and frequencies of outliers were calculated in SPSS with a t-test for comparing means and a Fisher's exact test for comparing categorical data. The level of difference was considered significant if the p value was below the threshold of 0.01.
Results
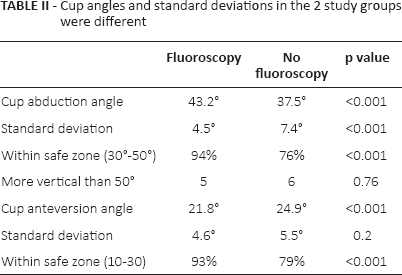
Among the 100 cases performed with intraoperative fluoroscopy, the mean cup abduction angle was 43.2° (SD = 4.5°). 94% of those cases fell within the Lewinnek safe zone of 30°- 50° of abduction. Of the 6 cases outside the safe zone, 1 was abducted less than 30°, and 5 were abducted >50°, but none >53°. The mean cup abduction angle for the 100 cases that did not employ intraoperative fluoroscopy was significantly less with 37.5° (SD = 7.4°) of abduction, p<0.001. 76% of the non-fluoroscopy cases were within the 30°-50° Lewinnek safe zone of abduction. Although more cases fell outside the safe zone (p<0.001), only 6 of the 24 cases outside the safe zone were more vertical than 50° of abduction, with the majority of the outliers falling below 30°. Table II summarises the cup angles and standard deviations of each group. The interquartile range as well as the total range of abduction angles in the fluoroscopy group were smaller than those of the non-fluoroscopy group, as shown in the box-and-whisker plot in Figure 2. The test of homogeneity of variance showed that the variance of the two groups was significantly different (p<0.001), with less variation in the fluoroscopy group.
Cup angles and standard deviations in the 2 study groups were different
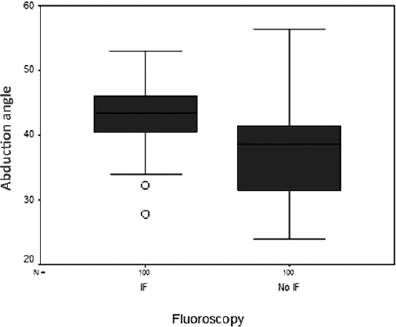
Box and whisker plot of the cup abduction angle distribution of the 2 study groups.
The mean anteversion angle for the cups placed with intraoperative fluoroscopy was 21.8° (SD = 4.6°). That angle was significantly less than the group without fluoroscopy, which averaged 24.9° (SD = 5.5°) (p<0.01). The test of homogeneity showed no difference in the variance of cup anteversion angle between the 2 groups (p = 0.20), and none of the cases in either group were retroverted.
1 case in the IF group dislocated 3 months after surgery and had a closed reduction in the emergency room. The cup angles for that case were very close to target at 41.5° of abduction and 20.9° of anteversion. 1 case in the non-fluoroscopy group sustained an intraoperative pelvic wall fracture. These are the only 2 complications that occurred in the 1st year after surgery.
Discussion
The target zone for positioning of the acetabular component has historically been 30°-50° of abduction and 5°-25° of anteversion (17). In the short term, the position of the acetabular cup plays an important role in hip stability and in decreasing the incidence of dislocation. Longer-term results also show cup position to be an important variable, as extremely high or low abduction angles have been correlated with increased polyethylene wear, edge loading, or impingement (18, 26, 27). The use of anatomic landmarks, external alignment guides, intraoperative radiographs, and computer assisted surgery have all been studied, and the results indicate that there is wide variability in accurately placing the cup in the desired position (28-29-30-31).
In our series of cases, the acetabular cup position was compared for DAA cases with cups placed by 2 different techniques. For the 1st group (DAA with IF), the goal was to optimise acetabular component position based on intraoperative fluoroscopy. In the 2nd group (DAA without IF) joint stability was used to determine final cup placement. 94% of the IF cups were within the Lewinnek safe zone of abduction compared to 76% of the non-fluoroscopy cups. In addition, there was less variation and fewer outliers in cup position among the cases using IF (Fig. 3). This is largely due to the intraoperative feedback in the cases where cup position was the priority.
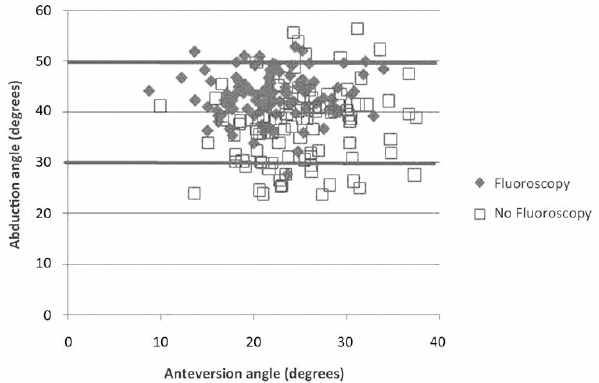
Scatter plot showing anteversion and abduction angles of 100 cases performed with intraoperative fluoroscopy (grey diamonds) and without fluoroscopy (white squares). The thicker lines indicate the Lewinnek safe zone of 30°-50° of abduction.
Non-fluoroscopy cases had a lower average abduction angle and more outliers <30° rather than >50°. Without the feedback of IF, the surgeon chose to err on the side of avoiding a vertical component, resulting in more cases with “flatter” cups. While avoiding high abduction angles may reduce early dislocation and edge loading, cups placed in a horizontal position have other potential concerns. The horizontal cup has decreased bony coverage on the back of the shell and can suffer from impingement at the superior edge (32, 33). These factors in combination have been shown to increase the risk of cup loosening in the long-term (26, 33).
The primary weakness of the study is that is it is a retrospective review of consecutive cohorts. The surgeon who does not use IF was unwilling to use it for the sake of the study, citing the cost and radiation exposure as unnecessary downsides to his patients. The surgeon who uses IF was unwilling to go without it, and considers it a crucial step in his procedure. It is a strength of the study that the surgeons were beyond their “learning curve” and had similar levels of experience with the direct anterior approach. Another relative shortcoming of this study is that the primary outcome measure is acetabular component positioning based on radiographs. Cup position is only 1 of several factors related to THA dislocation risk. With dislocation being a fairly rare complication, this study is underpowered to compare the 2 groups based on dislocation.
The effect of fluoroscopy on precision and accuracy of cup placement in total hip arthroplasty has not been well-studied. Rathod et al (14) retrospectively reviewed 825 cases where fluoroscopy was used in 453 direct anterior cases and no fluoroscopy was used in 372 posterior cases. They found variances for cup inclination and anteversion were significantly lower in the fluoroscopy group (p<0.01), but they compared those cases to a group performed without fluoroscopy using a posterior approach. These findings were confirmed in a recent study by Hamilton et al (13). In the current series, where all cases were performed through a direct anterior approach, the use of fluoroscopy resulted in less variation in cup abduction angle, however there was no difference in the variance of cup anteversion angle. 18% more cases in the fluoroscopy group fell within the Lewinnek safe zone of 30°-50° of abduction. The test of homogeneity of variance showed that there was significantly less variation (p<0.001), with the use of fluoroscopy.
Additional factors may play a role in the ideal cup position for different individuals. In studies of surgical approach, the cup may be positioned differently for the posterior approach compared to the direct anterior approach in order to prevent dislocation (13, 14). Emerging data suggests that patient factors also play a role in the optimal position of the cup. Pelvic tilt and spinopelvic mechanics have become a more common topic of discussion with regard to the optimal cup position (34-35-36). Indeed, in this series, the 1 case that dislocated postoperatively had a cup placed well within the safe zone, at 41.5° of abduction and 20.9° of anteversion. Until these phenomena are well-understood, surgeons should continue to use the established guidelines for position and stability.
Optimisation of acetabular cup position is 1 important factor to provide stability of the hip, prevent early failure of the bearing surface, and maximise range of motion. In our series of anterior approach THA cases, the use of intraoperative fluoroscopy resulted in less variation in cup abduction angle and significantly more cases within the traditional target zone when compared to 100 cases performed without fluoroscopy. It will be important to continue to follow these patients in the future to compare their long-term clinical results.
Footnotes
Acknowledgements
The authors would like to thank Cathy Huynh, BS, of Anderson Orthopaedic Research Institute for invaluable assistance with data collection.
Financial support: Inova Health System.
Conflict of interest: N.G. and W.H. are paid consultants at Cayenne Medical, Stryker Orthopedics, and DePuy. Our research institute receives institutional support from DePuy, Biomet, Nimbic Systems, and Inova Health Systems.