
Abstract
Introduction
In the present study, we identified factors affecting the outcomes of patients who underwent incomplete triple pelvic osteotomies due to acetabular dysplasia.
Methods
Data on a total of 58 hips in 50 patients for whom adequate data were available and who had undergone appropriate follow-up were retrospectively evaluated. We used Ömeroğlu scores for radiological evaluation, Harris Hip Scores for clinical evaluation, Tönnis scores to evaluate osteoarthritis progression and a modified Clavien-Dindo classification to evaluate complications.
Results
The average patient age was 23.26 (14-47) years, and the average follow-up duration 105.59 (18-191) months. The complication rate was 10.3%, and complications negatively influenced clinical outcomes. Patients with radiologically poorer outcomes had more advanced osteoarthritis. We found minimal improvements in lateral centre edge angle (LCEA), refined centre-edge angle (RCEA), and lateral acetabulum head index (LAHI) were associated with osteoarthritis progression and that good improvements in LCEA, RCEA, acetabular angle (AA), and LAHI were associated with radiological outcomes. Neither patient age at the time of operation nor development of a postoperative relative crossover sign affected osteoarthritis progression or clinical or radiological outcomes.
Conclusions
The most important factors influencing clinical outcomes were complications. However, neither postoperative acetabular retroversion nor a positive supra-equatorial crossover sign (often viewed as prognostically negative) directly affected clinical outcomes.
When treating patients with acetabular dysplasia, either inadequate correction or overcorrection may negatively affect outcomes. In such patients, an incomplete triple pelvic osteotomy (allowing controlled correction) is both safe and effective.
Introduction
The anterior and lateral walls are principally affected in patients with acetabular dysplasia. However, occasionally, the posterior wall is dysplastic. Such an abnormality is associated with the development of pain and symptomatic disease over time. Acetabular dysplasia causes secondary osteoarthritis (OA) in patients of advanced age (1-2-3-4). The major goal of treatment is correction of hip biomechanics, halting or even repairing the degenerative alterations triggering secondary OA (3-4-5).
Triple pelvic osteotomy was first introduced by Steel in 1965 and has since been modified by various authors, including Tönnis et al (6), Kumar et al (7), and Eren et al (2). The technique has been refined to feature only partial iliac osteotomy, thus sparing the posterior column. In this way, the advantages of the osteotomy can be ranked as: allowing adequate coverage of the acetabulum; being more stable; requiring less internal fixation material; needing less recovery time; having less risk of neurovascular damage due to not entering the sciatic notch; not requiring fluoroscopy imaging during surgery; and requiring less blood transfusion (2). In recent years this osteotomy has become popular and the medium-term outcomes of this technique have recently been described by Eceviz et al (8).
In the literature, retroversion, previous surgery, radiologic outcomes, progression of osteoarthritis and complications were reported as the factors which affect outcome (8, 9). In the present study we aimed to investigate possible factors affecting the outcome in patients who underwent incomplete triple pelvic osteotomies due to acetabular dysplasia.
Methods
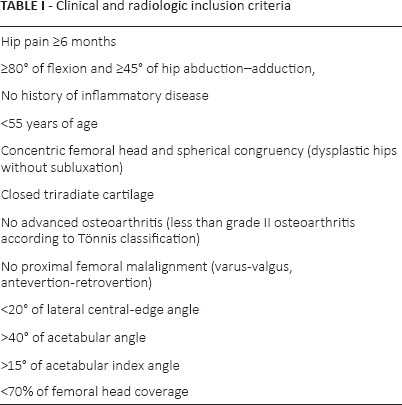
After Institutional Review Board approval, we retrospectively evaluated patients who underwent operations in our centre between April 1995 and June 2009. Incomplete triple pelvic osteotomies had been performed by a single surgeon on patients with acetabular dysplasia. Pre- and early postoperative data were collected from hospital records. The clinical and radiological inclusion criteria are listed in Table I. 5 patients were lost to follow-up, and we also excluded 3 patients with cerebral palsy, 1 with polio sequelae, and 1 with multiple epiphyseal dysplasia. Finally, data on 58 hips in 50 patients for whom adequate information was available and who completed follow-up were included.
Clinical and radiologic inclusion criteria
Pelvic x-rays were performed during weight-bearing and while the patellas were in a centralised position. We measured the lateral centre-edge angle (LCEA) (2, 3), refined centre-edge angle (RCEA) (10, 11), acetabular angle (AA) (12, 13), modified acetabular angle (MAA) (11), acetabular index angle (AIA) (13), lateral acetabulum head index (LAHI) (14), extent of lateralisation (LAT), and severity of OA on anteroposterior pelvic x-rays taken pre- and early postoperatively and at the last follow-up. While measuring RCEA and MAA, the maximal lateral corner of the subchondral sclerosis at the roof of the acetabulum were used instead of the maximal lateral corner of the acetabulum (11). We used the Tönnis system to score OA and the Ömeroğlu system to score preoperative and final follow-up radiological data (12). Preoperative clinical evaluation featured the use of hospital record data to calculate Harris Hip Scores (HHSs). We collected information on pain, function, and range of motion at the last follow-up, calculated HHSs, and compared these with preoperative scores. We also performed Trendelenburg testing and noted any paresthesia of the thigh (“meralgia paresthetica”). Clinical and radiological recoveries are presented as “recovery percentages.” Correlations among parameters are listed in Table II. We compared both preoperative and final Harris Hip and Ömeroğlu scores between patients with and without complications.
Surgical technique
Pelvic osteotomies were performed through two separate incisions; posteriorly for ischial osteotomy and anteriorly for pubic and iliac osteotomies. At a 45° oblique semisupine position, a posterior skin incision was made parallel to and 1 cm above the gluteal crest. Ischial osteotomy was performed just proximal to the origin of the biceps femoris. A bone wedge was resected to facilitate later acetabular reduction. After the patient was turned to a supine position, an anterior ilioinguinal skin incision was made. The tensor fasia lata and anterior fibers of gluteus medius were dissected by sharp dissection until gluteal tuberosity. Then the iliac bone was revealed subperiostally. Following pubic osteotomy performed at 1 cm medial to the iliopubic eminence, a subcristal iliac bone graft was resected from posterior part of the anterior superior iliac spine (ASIS). The graft was placed at the iliac osteotomy line which was started 2 cm superior to the ASIS and continued with a curvilinear cut that was parallel to the dome of the acetabulum through posterior to 1 cm above the sciatic notch. The acetabulum was redirected to the desired position with the help of a wedge shaped bone graft. K wire was used for stabilisation of the graft if needed.
Immobilisation was not required after the surgery. Partial weight-bearing and active hip movements were started on the 3rd postoperative day. Full weight-bearing with crutches was allowed after radiological verification of bony healing which usually occured at 6 to 8 weeks after surgery.
Statistical analysis
All statistical analyses employed NCSS 2007 software (NCSS Statistical Software). We used paired single-direction variance analysis when calculating definitive statistics and to evaluate the significance of recurrent measurements on multiple groups. We employed the Newman-Keuls multiple comparisons test for subgroup comparisons, the independent t-test for between-group comparisons, the chi-squared test to compare qualitative data, and McNemar's test to compare pre- and postoperative data. We used the Mann-Whitney U-test to compare “recovery percentages” calculated preoperatively and at the last follow-up. We calculated Spearman's correlations between parameters of interest. A p value <0.05 was considered to reflect statistical significance.
Results
The average patient age was 23.26 years (range 14-47 years); 41 of the 50 patients were female (82%), and 9 were male (18%). A total of 22 patients (44%) underwent surgery on the left hip, 20 (40%) underwent surgery on the right hip, and 8 (16%) underwent bilateral surgery. All patients had aceabular dysplasia, and 17 (34%) had undergone prior operations on the same hip(s). 10 patients had closed reduction, 2 had open reduction and Salter osteotomy, 2 had radical reduction, 1 had Chiari osteotomy, 1 had trochanteric shortening and 1 had subtrochanteric varisation osteotomy. The average follow-up duration was 105.59 (18-191) months.
The average LCEA, RCEA, AA, MAA, AIA, and LAHI values differed significantly pre- and early postoperatively and at the final follow-up. The preoperative values differed significantly from both the early postoperative (all p<0.001) and final values (all p<0.001), but the early postoperative and final values did not differ (all p>0.05) (Tab. II i).
Comparison of preoperative, early postoperative and final follow-up data (i) Radiologic data
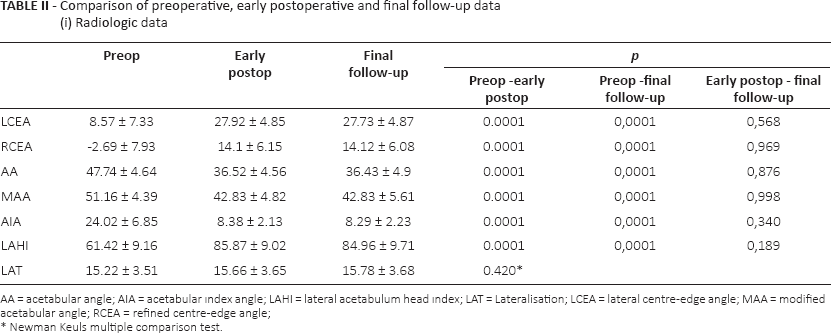
AA = acetabular angle; AIA = acetabular ındex angle; LAHI = lateral acetabulum head ındex; LAT = Lateralisation; LCEA = lateral centre-edge angle; MAA = modified acetabular angle; RCEA = refined centre-edge angle;
Newman Keuls multiple comparison test.
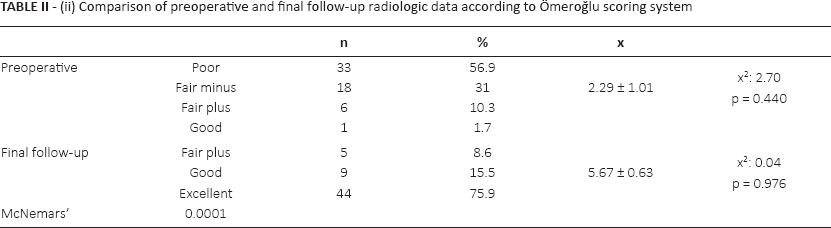
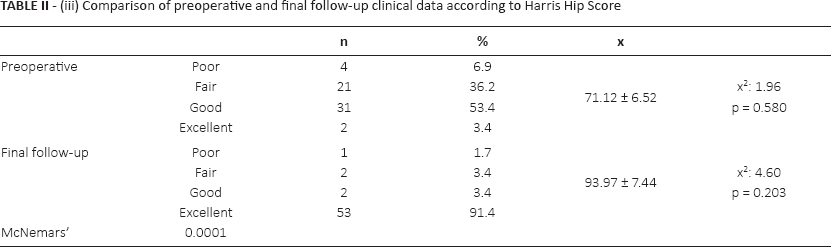
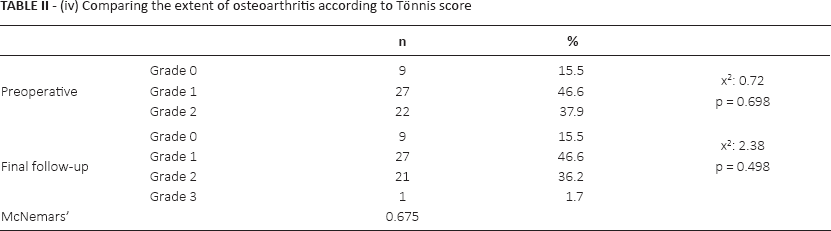
The average Ömeroğlu and Harris Hip scores were significantly higher at the final follow-up than preoperatively (both p = 0.0001) (Tab. II ii iii). The preoperative and final values did not differ in terms of either lateralisation (Tab. II i) or the extent of OA (Tab. II iv) (both p>0.05). We sought correlations between recovery percentages. Significant (negative) correlations were evident between the extent of OA and the recovery percentages of LCEA, RCEA, and LAHI (all p<0.001). However, we found no significant correlations between HHSs and LCEA, RCEA, AA, MAA, AIA, LAHI, lateralisation, OA, or the Ömeroğlu score (all p>0.05). Significant positive correlations were evident between the Ömeroğlu score and LCEA, RCEA, and LAHI (all p<0.05); and a significant negative correlation was apparent between the Ömeroğlu score and the AA (p<0.05) (Tab. III).
(ii) Comparison of preoperative and final follow-up radiologic data according to Ömeroğlu scoring system
(iii) Comparison of preoperative and final follow-up clinical data according to Harris Hip Score
(iv) Comparing the extent of osteoarthritis according to Tönnis score
Correlations between parameters
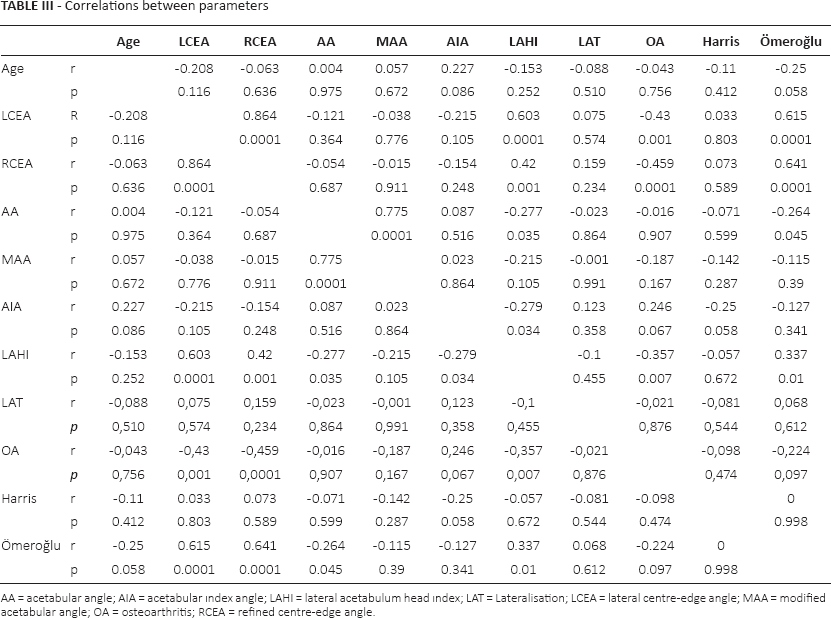
AA = acetabular angle; AIA = acetabular ındex angle; LAHI = lateral acetabulum head ındex; LAT = Lateralisation; LCEA = lateral centre-edge angle; MAA = modified acetabular angle; OA = osteoarthritis; RCEA = refined centre-edge angle.
Patients with complications were separately evaluated, and their data were compared with those of patients without complications. The average HHS of the former group was significantly lower than that of the latter group (p = 0.002). In patients with complications, the average HHSs preoperatively and at the final follow-up were similar (p = 0.113), but the Ömeroğlu score was significantly higher at the final follow-up.
Complications
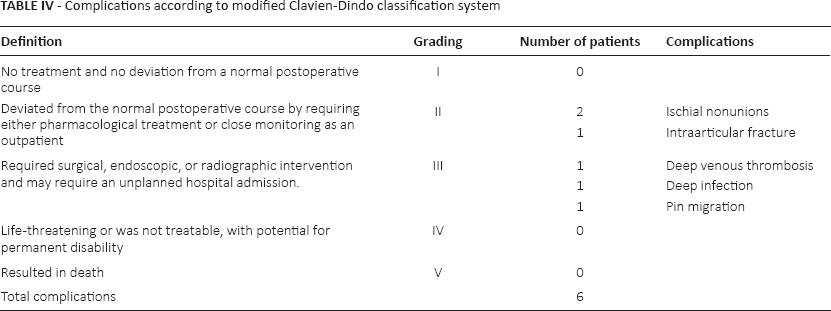
Complications were determined according to a modified Clavien-Dindo classification system (9); these included 1 case of deep vein thrombosis, 1 infection, 2 ischial nonunions, 1 intraarticular fracture, and 1 case of pin migration at the femoral head (6/58 hips) (Tab. IV). The only complication requiring revision surgery was chondrolysis of the femoral head caused by pin migration. This patient underwent resurfacing arthroplasty. No patient who was Trendelenburg test positive showed heterotopic ossification or complained of marelgia paresthetica during follow-up.
Complications according to modified Clavien-Dindo classification system
Discussion
Eren et al (2) has listed the advantages of the novel incomplete triple pelvic osteotomy technique: there is no risk of fracture or avascular necrosis of the acetabulum; there is a minimal risk of neurovascular injury; the learning curve is fast, and the procedure optimally mobilises the distal segment. Moreover, the authors suggested that retention of an intact posterior column would stabilise the osteotomy line, rendering a Kirschner wire adequate to stabilise the graft. Additionally, as the osteotomy line runs remote from the sciatic notch, the risk of neurovascular injury is reduced, as is the need for blood transfusion (2, 3). Of the various forms of triple osteotomy, the posterior column is retained in the incomplete triple pelvic osteotomy as carried out in the Bernese procedure (2, 3, 9, 10). The literature suggests that the most challenging feature of triple osteotomy is the risk of losing acetabular orientation after total release. Such loss during surgery may cause the acetabulum to be incorrectly stabilised, or (at least) to undergo more anterior-lateral rotation than necessary. The most significant complication of Bernese osteotomy is erroneous orientation of the acetabulum after total release; appropriate positioning requires extensive surgical experience. Acetabulum correction is adequately controlled if the CORA (centre of rotation angulation) point is not lost (2, 3).
Hasegawa et al (10) reported the outcomes of rotational acetabular osteotomies performed on 273 hips of 248 patients with a follow-up duration of 10.5 years. Steppacher et al (15) reported the 20-year outcomes of 58 patients who underwent Bernese osteotomies. Our present study is one of the most comprehensive in the literature in terms of both sample size (58 hips) and mean follow-up duration (8.79 years).
The Severin system is the gold standard for dysplastic hip classification (8, 12). However, interobserver reliability is very low. The major reason is that dubious parameters are evaluated; these include moderate deformity, moderate dysplasia, subluxation, and continuity of the Shenton line. Moreover, although the Severin system yields a snapshot of the present radiological situation, treatment success is not scored. Thus, in the present study, we used the Ömeroğlu system to standardise radiological outcome data. This system is objective and both inter- and intraobserver reliabilities are high due to the attention paid to objective criterias such as CEA, AA and centre of femoral head to trochanteric distance (8, 12).
We found that the preoperative LCEA, RCEA, AA, MAA, and LAHI values improved significantly at the last follow-up. All radiological outcomes were in line with those described in the literature, except for RCEA (evaluated by only Hasegewa et al (10)) and MAA (not evaluated in any prior study) (Tab. II i).
Compared with preoperative values, the Ömeroğlu score improved by 3.38 points (preoperative: 2.29, final follow-up: 5.67) and the radiological recovery percentage was 59.94% (thus, significant; Table II ii). Good radiological results (Ömeroğlu scores: good, very good, or perfect) were evident in 53 hips (91.4%). As the literature contains no data on radiological recoveries, we cannot present comparisons.
We found that neither a postoperative crossover sign nor complications affected radiological outcomes. No correlations were found between age at time of operation, MAA, AIA, lateralisation, OA, or HHS recovery percentages and radiological data, but the LCEA, RCEA, AA, and LAHI recovery percentages did (significantly) correlate. The literature identifies postoperative displacement (15), low postoperative LCEA, postoperative AIA >10° (16), advanced age, high HHS, and complications as factors (negatively) affecting radiological outcomes (17).
We found that lateralisation increased, on average, by 0.56 mm postoperatively; this was not statistically significant. Siebenrock et al (16) found that lateralisation decreased by 6 mm; Hasegawa et al (10) reported a decrease of 3.8 mm; Hailer et al (17) reported a decrease of 0.01 mm; and Doğan et al (18) reported an increase of 1.7 mm. Lateralisation of the acetabular rotational centre is a common complication of Steel osteotomy (6, 7). However, we found that incomplete triple pelvic osteotomy did not lateralise the acetabulum significantly; we had no need to perform the Kumar modification.
We found no significant difference between the pre- and postoperative extents of OA (Tab. II iv); OA progression in our patients was less than in other patient series. Although the eventual goal of acetabular dysplasia treatment is to prevent secondary OA, many publications do not grade the extent of OA. The absence of OA deterioration shows that incomplete triple pelvic osteotomy effectively halts or delays OA progression.
A low rate of total hip replacement surgery among pelvic osteotomy cohorts is generally regarded as an indicator of successful operative treatment. None of our patients has yet undergone total hip replacement surgery, except 1 who underwent resurfacing arthroplasty because of a complication of pin migration. Thus, incomplete triple pelvic osteotomy successfully obviates the need for total hip replacement.
Many authors use the HHS in clinical evaluation (10, 17, 19); others prefer the Merle d'Aubigné and Postel system (15, 17, 20, 21). We chose the HHS, which is currently the most favoured. The mean preoperative score (71.12) improved to 93.97 at the final follow-up. The clinical recovery percentage was 23.71%, which was statistically significant (Tab. II iii). Of all hips (57), 98.3% showed clinically good results (HHSs: good and perfect). Peters et al (22) reported that the HHS improved by 33 points in their patient series. Hasegawa et al (10) reported a 21-point improvement, and McCarthy et al (19) reported 17.1 points of improvement. The cited works did not give patient numbers or recovery percentages; however, our results are comparable in terms of recovery. We present clinical improvements as recovery percentages to clearly show how many patients benefited from surgery and to what extent.
We found that none of the postoperative crossover signs, complications, age at time of operation, AA, MAA, AIA, lateralisation, or Harris Hip or Ömeroğlu score affected OA progression. However, the LCEA, RCEA, and LAHI were significantly correlated with the extent of OA (Tab. II ii). Both postoperative retroversion (23) and preoperative advanced OA have been reported to correlate with OA progression (15, 16).
We found that complications negatively affected clinical outcomes and the Harris hip score. Patients with positive postoperative supra-equatorial crossover signs recovered better than did patients with negative signs. Complications affecting outcomes included an intra-articular fracture and pin migration. Although neither any radiological criterion nor the Ömeroğlu score was associated with clinical outcomes, many studies have reported that advanced age at the time of operation (15-16-17), low preoperative Merle d'Aubigné and Postel score (15), positive impingement test (15), preoperative limping (15), preoperative labral lesion (16), complications (17), and a lower Harris Hip Score (17) correlated with clinical outcomes.
We found that postoperative crossover signs did not affect radiological outcomes (Ömeroğlu scores) or OA progression (Tönnis scores). Indeed, patients with postoperative positive supra-equatorial crossover signs recovered better than did those without signs. All of the patients who had acetabular retroversion were positive for posterior wall sign. Since incomplete triple pelvic osteotomy leaves both the posterior column and the posterior wall intact, encountering with true retroversion is not predicted. So a supra-equatorial crossover sign is associated with relative acetabular retroversion. As such patients were in poorer preoperative clinical condition, their recovery percentages were higher. Moreover, after incomplete triple pelvic osteotomy, patients developed neither femoraacetabular impingement nor restriction of flexion. The radiographs showed that the crossover signs were in the middle-to-upper one-third of the acetabulum (supra-equatorial). We are of the view that a crossover sign appearing after incomplete triple pelvic osteotomy is attributable to a global acetabular deficiency. No patient with a sign experienced any negative effect; thus, the sign is not of concern. However in Bernese osteotomy, acetabular reorienting is difficult and may cause anterior impingement if it is overcorrected.
The complications of pelvic osteotomy include major neurovascular injury (16, 19-20-21, 24), heterotopic ossification (10, 19, 24), abductor weakness (10, 25), displacement of the major trochanter (10), haematoma formation (10, 24), Sudeck atrophy (10), over- or under-correction, posterior subluxation caused by a defective posterior cover (16), and posterior colon fracture (24). Half of all patients undergoing Bernese osteotomy develop major complications (4, 11, 26, 27). None of these complications is associated with incomplete triple pelvic osteotomy. As the osteotomy line runs remote from the hip joint, heterotopic ossification and avascular necrosis of the acetabulum are not to be expected. Also, as the abductors are separated by sharp dissection from the iliac bone, abductor weakness does not develop. As the sciatic notch is not invaded, neither sciatic nor peroneal palsy is encountered. Only 6 of our patients developed complications according to a modified Clavien-Dindo classification (10.34%); this is much lower than other findings in the literature (10%-65%) (10, 16, 19). In a recent study Zalzt et al (9) revealed complications in Bernese periacetabular osteotomy and reported that while the complication rate was 14.6% at early term, it increased to 20.4% at late-term follow-up. These authors utilised a modified Clavien-Dindo classification. Compared with our series (without grade IV or V complications), Zalzt's study consisted of experienced surgeons and grade III and IV types of complications were a common concern. Another point of interest is about heterotopic ossification is that while we did not encounter any heterotopic ossification cases, in Bernese osteotomy it is quite a common problem (9, 10, 19, 24).
The hospital records did not contain pre- and postoperative false profile views. Therefore, we did not take such images at the final follow-up, as the images would not have been useful. The limitations of our study include its retrospective nature and the absence of false profile data. Because of the rarity of the cases, power analyses could not be carried out. The positive features of the study are our description of the mid-term outcomes of a reasonable number of patients; the fact that all patients were operated on by a single surgeon; and our use of a radiological scoring system for patient evaluation.
Conclusions
Incomplete triple pelvic osteotomy affords all the advantages of the Bernese periacetabular osteotomy procedure, as the posterior column remains intact and the abductor mechanism is not destroyed. Additional advantages include the absence of any need for intraoperative fluoroscopy (enhancing the safety of both patient and surgeon), a low complication rate, and excellent control of the extent of correction. We found that complications negatively affected clinical outcomes, that patients with positive postoperative crossover signs recovered better than did others (with no signs), and that advanced OA (stages 2 and 3) was more evident in patients who had the poorest radiological outcomes. Also, inadequate correction of radiological parameters, as reflected in the postoperative LCEA, RCEA, and LAHI, were associated with OA progression. However, neither advanced age at the time of operation nor a positive postoperative crossover sign (commonly regarded, in the literature, as contributing to negative outcome) was associated with OA progression or the clinical or radiological outcomes.
Although rare, the most severe complications encountered were an intra-articular fracture and chondrolysis caused by pin migration. The most important factors influencing clinical outcome were complications. However, neither postoperative acetabular retroversion nor a positive supra-equatorial crossover sign (often viewed as prognostically negative) directly affected clinical outcome. We are of the view that the principal concern is femoroacetabular impingement syndrome. This is the most common complication after Ganz osteotomy; the syndrome causes overcorrection.
When treating acetabular dysplasia, both inadequate correction and also overcorrection may negatively affect outcome. We have shown that incomplete triple pelvic osteotomy (which permits controlled correction) is a safe and effective option.
Footnotes
Financial support: None.
Conflict of interest: None.