
Abstract
Introduction:
The design of the cementless Symax-HA femoral stem is based on geometrical analysis of human femoral anatomy to optimise the fit within the femur. The stem combines an anatomical proximal section enabling a metaphyseal anchorage with a straight distal section. This results in an improved proximal load transfer.
We aimed to determine the overall survival of total hip arthroplasty (THA) in patients operated at our institution with the Symax stem. Secondly, we investigated the cause of revision for patients having THA including the Symax stem.
Methods:
The study is a registry study with results from a single centre, Vejle Hospital. From the Danish Hip -Arthroplasty Registry, we identified all THAs operated with the Symax stem. The primary outcome was revision. The secondary outcomes were aseptic loosening, periprosthetic fracture, and all other causes for revision.
Results:
In total, 1,055 THAs were performed in 875 patients. The median 6.5-year survival rate was 97.5% (95% confidence interval [CI]: 96.6%-98.3%). 29 THAs had undergone revision due to the following causes: periprosthetic fracture (n = 11); aseptic loosening of the cup (n = 1); infection (n = 5); dislocation (n = 10); and component failure (n = 2). There was no revision due to aseptic loosening of the stem.
Conclusions:
From the Danish Hip Arthroplasty Registry, we identified the overall 6.5-year survival rate to be 95% for cementless THAs. In the present study, the Symax stem has a median 6.5-year survival rate at 97.5% (96.6%-98.3%). No revisions were due to aseptic loosening but the stem had a relative high prevalence of periprosthetic fractures.
Keywords
Introduction
The survival rates for cementless total hip arthroplasty (THA) depend on the component design, material, and type of coating. 1 Therefore, several issues must be addressed when using cementless stems: initial implant stability; durable long-term bone-implant fixation; strain transmission to the proximal femur; and restoration of the hip mechanics. 2
The primary stability of the stem is achieved by filling the femoral diaphysis or getting intimate contact between the stem and the anatomy of the proximal femur. 2 An important criterion to achieve primary stability is good rotational and axial stability of the implant. Primary stability is accomplished by press-fit fixations; therefore, a certain roughness and structures of the implant surfaces are required. 3 The early bone ingrowth is dependent of the primary stability of the stem. 1 Hydroxyapatite (HA), porous coatings or osteoconductive material like specific titanium-iron alloy improve the early bone apposition and biological fixation. 1 Fixation is achieved by biological integration of the implant by bone ingrowth. This ingrowth resembles the process of fracture healing, and include reactive, reparative, and regenerative stages. 4 Optimal fixation of cementless stems is therefore essential for long-term stability.
The Symax-HA femoral stem is designed for cementless THA. The design is based on geometrical analysis of human femoral anatomy to optimise the fit in the femur. The stem combines an anatomical proximal section enabling a metaphysical anchorage with a straight distal section. This results in an improved proximal load transfer and less chance of interface loosening, allowing more natural stress distribution and less stress shielding. Proximal press-fit fixation is achieved by a lateral and anterior extension based on analytical geometry. 3 rips ensure primary rotational stability. The stem is proximal plasma-sprayed with titanium and coated with a BONIT®-HA biomimetic coating, which secures secondary stability by osseous integration.3,5,6 The neck diameter is reduced and combined with a short taper and small caput-collum-diaphysels angle (128°) enables an extended range of motion. 3 The neck is coated with the DOTIZE® (DOT GmbH) 5 surface process, an electrolytic conversion of the titanium surface in which the thin native oxide film is replaced by a thicker, oxidised conversation layer that reduces protein absorption and hence reduces abrasion wear.5,7
To our knowledge, no study has investigated the medium-term survival of the Symax stem. Therefore, we aimed to examine the overall survival rate after maximal follow-up of 10 years and after a median follow-up, when a significant number of patients were at risk, and further to investigate the causes of revision of the THA in patients operated at Vejle Hospital, Denmark with the Symax stem.
Methods
Data sources
In Denmark, every citizen is at birth given an unchangeable 10-digit personal identification number, linking 5.6 million people to all Danish medical databases. 8 This allows for technically easy, cost-effective, and unambiguous individual-level record linkage of Danish registers. Daily updated information on migration and vital status allows for nationwide cohort studies with virtually complete long-term follow-up on emigration and death. 9
The Danish Hip Arthroplasty Registry (DHR) was established January 1, 1995. 10 Registration to the DHR is mandatory for all Danish orthopaedic departments and includes all THAs and all revisions of THAs. The completeness of the data is considered the proportion of THA reported to the DHR out of the total number of THAs reported to the DHR or the Danish National Patient Registry (DNPR) 11 , which is considered the gold standard as the health authorities reimburse the orthopaedic departments when reporting to the DNPR. In 2016, the completeness for primary THA and revisions were 99.8% and 98.1%, respectively.12,13
Study population
From the Danish Hip Arthroplasty Registry, we identified all THAs operated with the Symax stem from May 11, 2004 to May 24, 2013 at Vejle Hospital, Denmark. This includes all patients ever operated with the Symax stem at Vejle Hospital, Denmark before May 24, 2013.
Statistics
For the presentation of demographic data and procedure characteristics descriptive statistics were used. Patients entered the study on the date of primary surgery and were followed until revision, death, emigration, or end of study period (July 31, 2014) whichever came first. Revision was defined as a new surgical intervention including partial or complete removal or exchange of the implant. Any revision cause was considered as endpoint. When a patient received bilateral THA operations, both THAs were included in the study. Median follow-up and interquartile ranges (IQR) were calculated. Survival curves were constructed by the Kaplan-Meier method with 95% confidence intervals (CI) and log-rank test was used to test for difference in survivorship among sex, age, and -bearing groups. Primary outcome was any revision and secondary outcomes were aseptic loosening, dislocation, periprosthetic fracture and all other causes of revision at 10 years follow-up. Fisher’s exact test was used to compare femoral head sizes in the THAs revised due to periprosthetic fracture comparing with those femoral head sizes used in the rest of primary THAs.
A p value <0.05 was considered significant. Statistical analyses were carried out by using the Stata Statistical Software, Release 14.1, College Station, TX: Stata Corporation.
Results
In total, 1,055 THAs implanted by 4 surgeons were performed in 875 patients; hence, 180 patients were operated bilaterally. 577 patients (54.7%) were male. The mean age was 63.2 years ± 9.9 SD (range 21-91). 1 patient (0.1%) had an inverse hybrid THA (Table 1). The reason for this was that the acetabulum fractured perioperatively, when the cup was inserted. The surgeon therefore changed from a cementless cup to the cemented Contemporary cup. Otherwise, the fixation was cementless for all other patients. 779 primary THAs (73.7%) were performed between 2004 and 2008, whereas 276 (26.2%) took place during 2009 to 2013. There was a trend towards using larger femoral heads during the period 2007-2011, and the most commonly used femoral head size was 36 mm (Table 2).
Patient- and surgery-related characteristics of the study population.
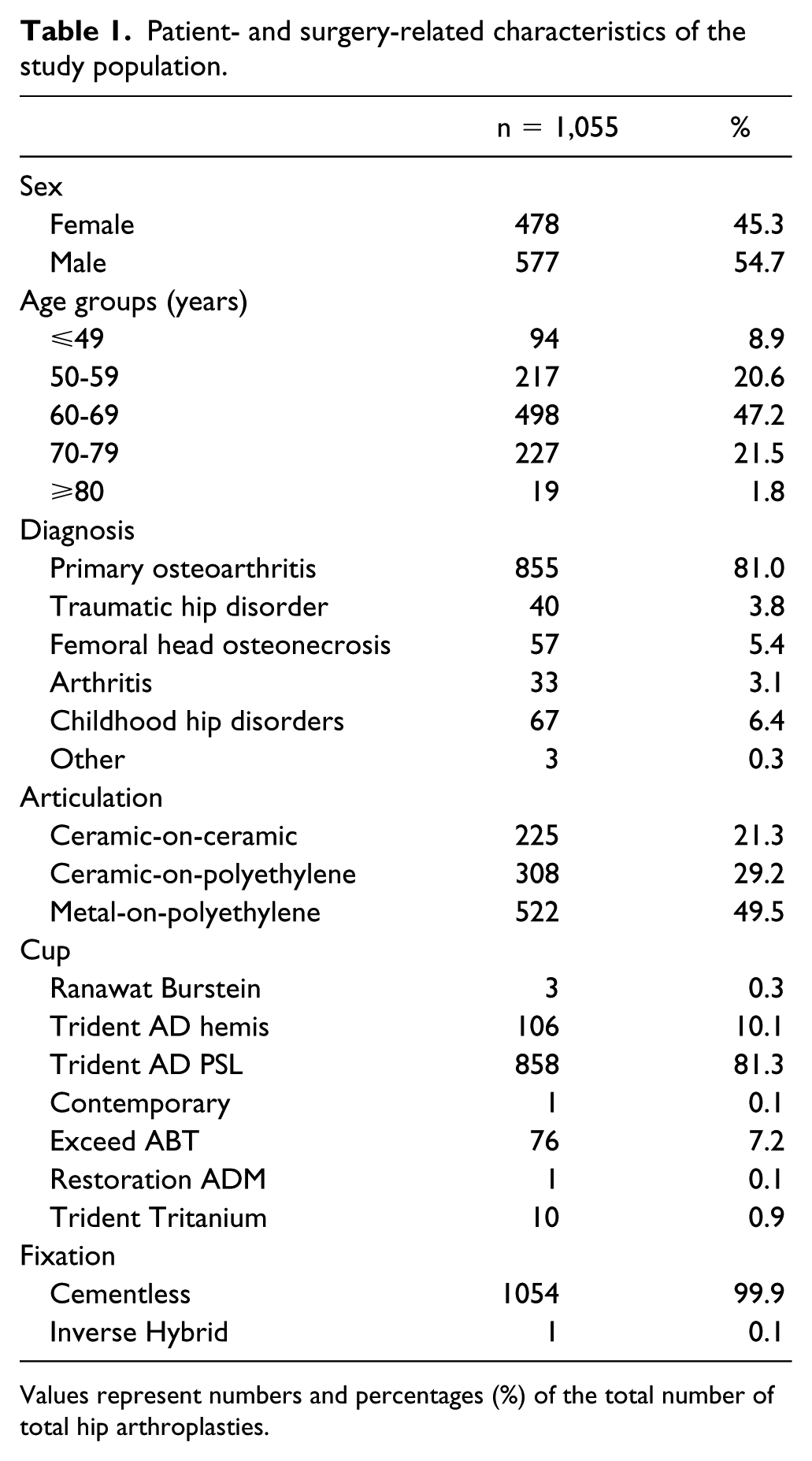
Values represent numbers and percentages (%) of the total number of total hip arthroplasties.
Femoral head size used.
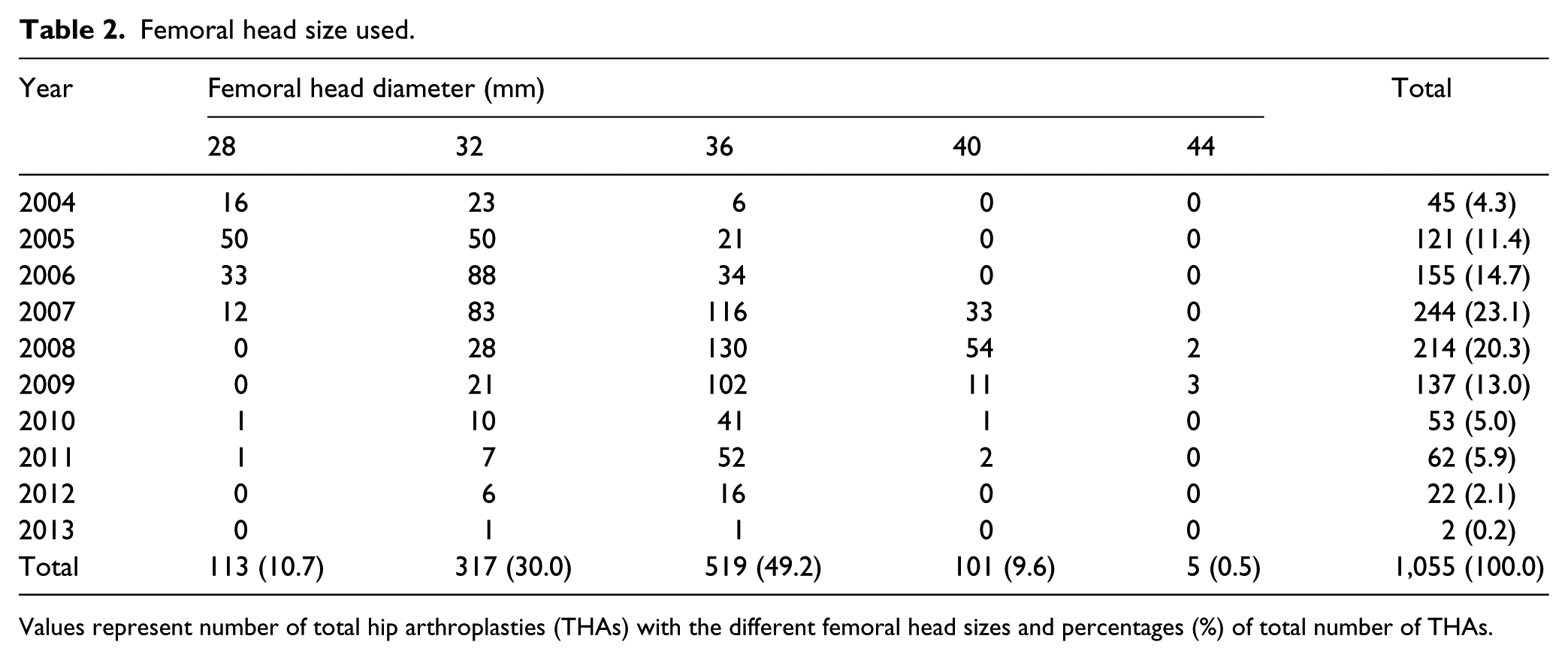
Values represent number of total hip arthroplasties (THAs) with the different femoral head sizes and percentages (%) of total number of THAs.
Median follow-up for the entire study population was 6.5 years IQR 5.1-7.8 (range 4 days to 10.2 years). 6 patients had a follow-up beyond 10 years and 2 of these had a follow-up to 10.2 years. At the end of the study period, 29 (2.8%) THAs had undergone revision surgery and patients with 86 (8.2%) THAs had died or emigrated. With all-cause revision as endpoint the overall survival rate at the median 6.5- year follow-up was 97.5% (96.6%-98.3%) and 10.2-year survival rate was 96.5% (94.6%-97.7%, n at risk = 2). There was no difference in survival for men and women (p = 0.12), for patients younger or older than 60 years (p = 0.70) or for patients with ceramic-on-ceramic, ceramic-on-polyethylene and metal-on-polyethylene bearings (p = 0.45) (Figures 1-4). No revisions were due to aseptic loosening of the stem. The most frequent cause for revision was periprosthetic fracture seen in 1.0% (11 of 1,055) of primary THAs (Table 3). No patients were revised for aseptic loosening of the Symax stem. With periprosthetic femoral fracture as endpoint, the survival rate after the median 6.5-year follow-up was 99.0% (98.2%-99.5%) and with all other revision causes as endpoint, the survival rate was 98.4% (97.4%-99.0%) after median follow-up.
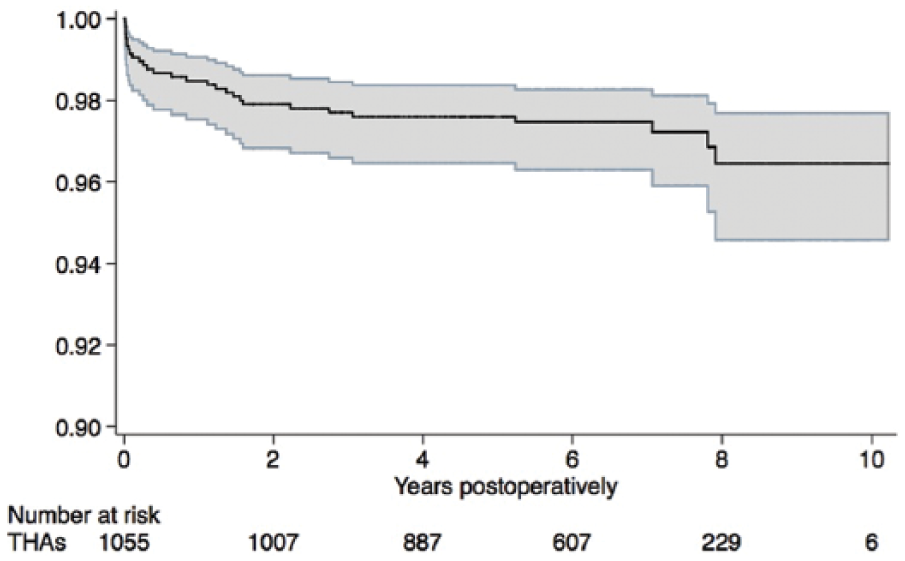
Kaplan-Meier survival curves for 1,055 Symax THAs. After median follow-up of 6.5 years, the survival rate was 97.5% (96.3%-98.3%).
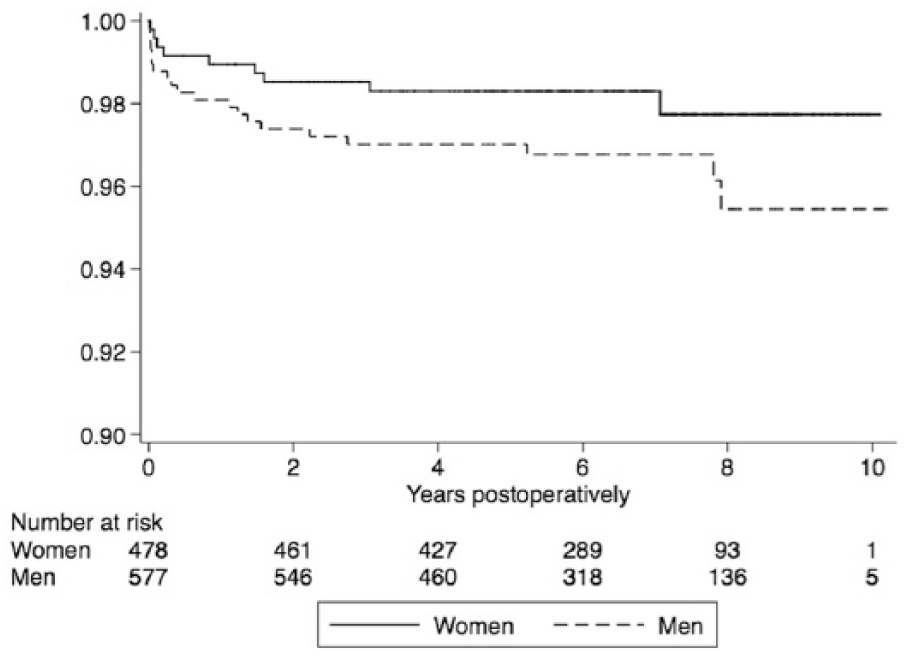
Kaplan-Meier survival curves for women (n = 478) and men (n = 577). After median follow-up of 6.5 years, the survival rate was 98.3% (96.6%-99.2%) for women and 96.8% (94.9%-98.0%) for men (p = 0.12).
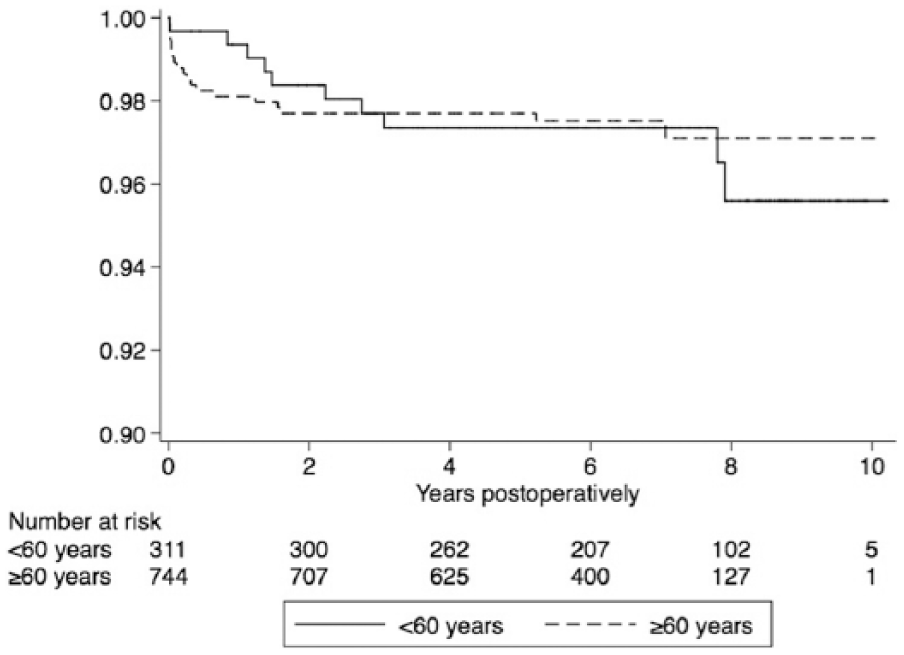
Kaplan-Meier survival curves for patients <60 years (n = 311) and for patients aged 60 years or older (n = 744). The median follow-up for patients younger than 60 years was 7.2 years (IQR 5.5-8.5) with a survival rate at 97.4% (94.8%-98.7%). For patients older than 60 years the median follow-up was 6.3 years (IQR 4.9-7.4) with a survival rate at 97.5% (96.1%-98.4%) (p = 0.70).
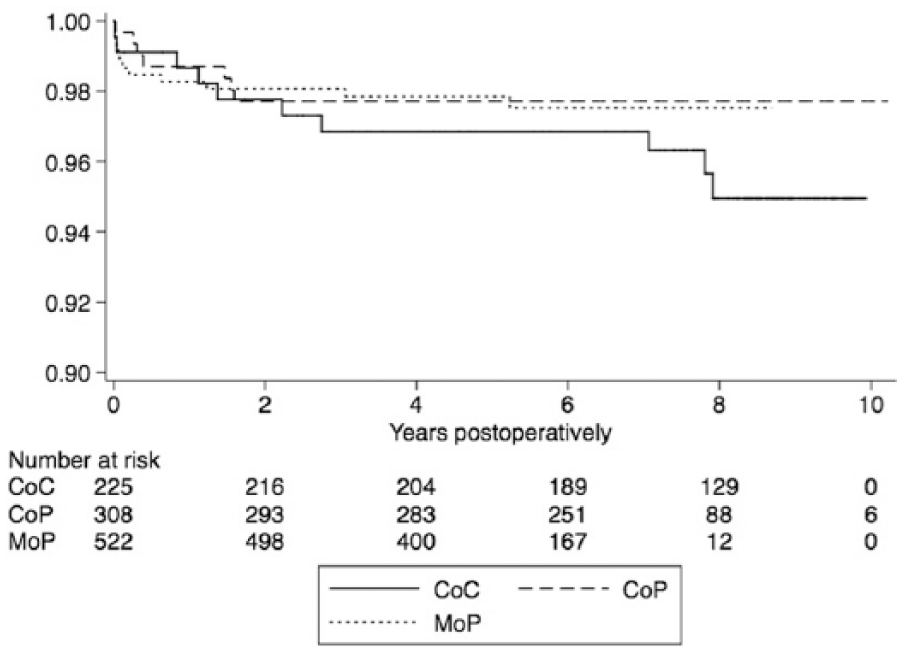
Kaplan-Meier curves for patients with ceramic-on-ceramic (CoC) ceramic-on-polyethylene (CoP) and metal-on-polyethylene (MoP) bearings. The median follow-up for patients with CoC was 8.4 years (IQR 7.5-8.9) with a survival rate at 95.0% (90.7%-97.3%). The median follow-up for patients with CoP was 7.3 years (IQR 6.5-8.2) with a survival rate at 97.7% (95.3%-98.9%). The median follow-up for patients with MoP was 5.5 years (IQR 4.2-6.4) with a survival rate at 97.5% (95.7%-98.6%) (p = 0.45).
Causes for revision.
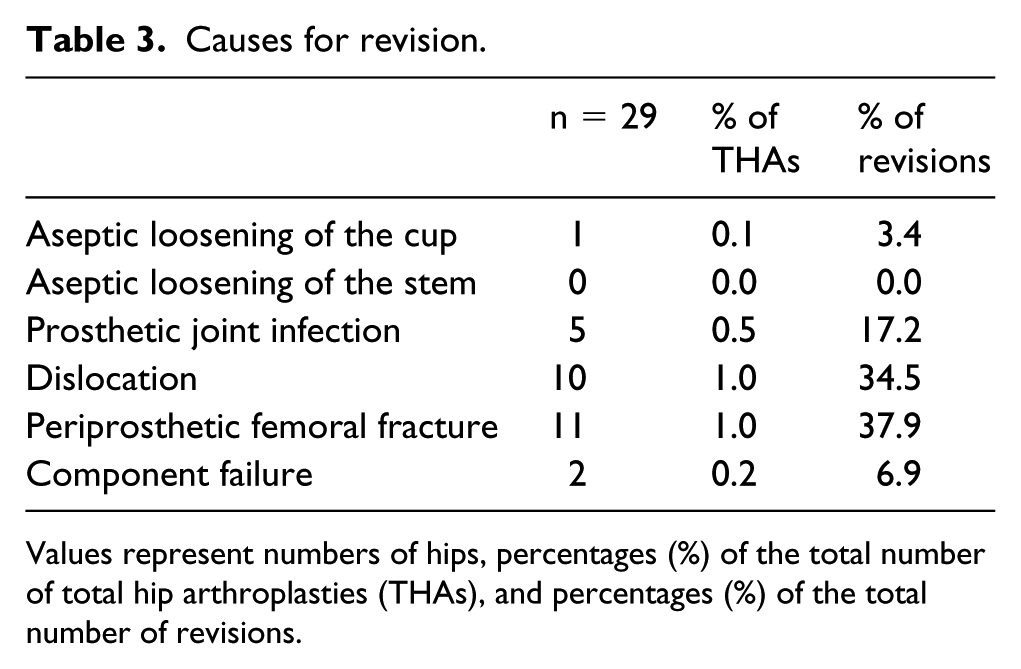
Values represent numbers of hips, percentages (%) of the total number of total hip arthroplasties (THAs), and percentages (%) of the total number of revisions.
The mean age of patients revised due to periprosthetic fracture was 62.9 years ± 12.0 standard deviation (SD) (range 42-77), and 7 of the 11 periprosthetic fractures occurred within the first 6 months after primary surgery. 4 of the fractures were seen in patients operated in 2007 whereas the rest of the fractures were evenly distributed in patients operated between 2004-2011. The follow-up from primary THA and revision for periprosthetic fracture ranged between 0.2-94.9 months, and the femoral head size in THAs revised for fracture had a range between 32-40 mm (Table 4). There was no statistical difference in the distribution of different femoral head sizes in THAs revised due to periprosthetic fracture compared to patients not revised for fracture (p = 0.56).
Correlation between year of surgery, age, follow-up, and femoral head size for patients revised due to periprosthetic femoral fracture.

THA = total hip arthroplasty.
2 revisions were due to component failure: a 51-year-old female experienced squeaking 8 months after surgery, and later on also intense clicking from the hip. On radiographs, it was suspected that the acetabular liner was not completely seated into the shell, but this suspicion was rejected during revision. Wear due to impingement between the neck of the stem and the titanium border of the acetabular liner was -recognised. The 2nd revision due to component failure was performed in a 58-year-old male who experienced clicking immediately after surgery. Radiographs showed the acetabular component positioned in excessive anteversion (37°), and 6 months after surgery there was also sign of impingement between the neck of the stem and the titanium border of the acetabular liner.
Conclusion
The Symax stem has a high survival rate after the median 6.5-year follow-up with no revisions due to aseptic loosening but with a relative high prevalence of periprosthetic fracture. The periprosthetic fractures were most frequent in the early postoperative months.
From the DHR, we identified the overall 6.5-year survival rate for cementless THA to be 95%. 12 This is lower than the study we present, in spite of an expected learning curve when introducing the Symax stem at Vejle Hospital. The DHR report an incidence of revision due to aseptic loosening of 16.6% of all revisions for all cementless stems between 1995-2016 12 but in our study, there were no revisions caused by aseptic loosening of the stem. To support our findings, -Buratti et al 6 report a study of 85 Symax femoral stems that were followed at regular intervals with radiographs at 6, 12, 24 and 36 months measuring the radiological migration of each stem using a computer-assisted EBRA-FCA method. In all cases, subsidence of the stems was minimal. These data represent a positive predictive factor for minimising the risk of future aseptic loosening and perhaps indicating a minimal risk of aseptic loosening in general for the Symax stem 6 . Ten Broeke et al 14 reported a study of 49 femoral stems comparing bone remodelling around the cementless Symax and Omnifit stems. The effect on bone mineral density was determined using standard adapted Gruen zones, which originally was designed for analysis of stem loosening.14, 15 The difference with the Symax bone mineral density values, which had been concealed using Gruen zones, became statistically significant in favour of the Symax stem when compared to the Omnifit stem. 14 Thus, there are several indicators supporting the minimal risk of aseptic loosening for the Symax stem.
Thien et al 16 have used the Nordic Arthroplasty Register Association database to evaluate the risk for revision of the THA due to periprosthetic fracture within 2 years. They found that the incidence of revision due to periprosthetic fracture was 0.47% for cementless THAs (Bi-Metric, CLS Spotorno, Corail, ABG I and II). Nearly all of the fractures occurred within the first 6 months. 16 We found the prevalence of revision due to periprosthetic fracture for the Symax stem at 10.2-years to be 1.0%.
The reason for this relative high prevalence of periprosthetic fractures compared to other cementless stems is unclear. The periprosthetic fractures were distributed between 2004-2011 indicating, that the reason was not a learning curve. A suggestion for the increased fracture risk has been, that it was related to the size of the femoral head. An explanation might be that the surgeon chose a large femoral head to avoid dislocation, which resulted in a different load transfer stressing the femur. However, there was no correlation between the larger femoral head sizes used between 2007-2011 and the higher prevalence of periprosthetic fractures in our study (Table 2 and 4). 7 of the 11 of the periprosthetic fractures occurred during the first 6 months. Some of them might have appeared during surgery as minor fissures, which -progressed to obvious clinical fractures during the rehabilitation period. 16 -Bergschmidt et al 3 experienced 3 intraoperative periprosthetic fractures as a result of -intraoperative preparation. They therefore recommended larger approaches, careful canal preparation when using the Symax stem. 3 Ten Broeke et al 17 investigated whether the Symax stem would yield improved bone remodelling in a clinical DEXA study compared to the Omnifit stem. They found that the geometry of the modified stem together with the other modifications were able to improve stress transfer from the implant to bone in the important area proximal and medial to the stem (Figures 5 and 6). They also showed that the stem preserved the periprosthetic bone better than almost all proximally and entirely porous or HA-coated stems. 17 This indicated that the geometrical design of the stem might decrease the incidence of periprosthetic fractures and aseptic loosening. Thus, the reason for the increased fracture risk with the Symax stem in our study may be related to the surgical technique or poorer bone quality although patients revised due to periprosthetic fracture had similar mean age as the other patients.

The Symax™ stem.

Postoperative x-ray of the Symax stem.
Strengths of our study include the prospective collection of data, the relatively large sample size for a single institution, and the complete follow-up. Furthermore, the registries that provided data for this study have an overall good validity.9,12,18 This study also has limitations that should be taken into account: Compared to a multicenter or a register-based study, a study from a single institution reduces the generalizability due to potential selection problems. From 2004 to 2013, alternative stems to the Symax were used, and 1 of 4 surgeons that operated on patients included in this study operated on the majority of patients indicating that confounding by indication could not be excluded.
After median follow-up of 6.5 years, the Symax stem has a survival rate at 97.5% (96.6%-98.3%). No revisions were due to aseptic loosening but the stem had a relative high prevalence of periprosthetic fracture. The periprosthetic fractures were most frequent in the early postoperative months. Due to the high survival rates and the absence of aseptic loosening, we find that the Symax stem is a good alternative to other cementless stems. However, patient selection, larger approaches and careful canal preparation shall be considered in order to minimise the risk of periprosthetic fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.