
Abstract
Significant thrombocytopenia following hemodialysis with electron-beam (e-beam) sterilized membranes has been recently reported in a large-scale Canadian study. However, the underlying mechanism and the clinical significance of this finding remain undetermined as yet. We prospectively evaluated for a 4-month period the thrombocytopenic effect of the e-beam sterilized dialyzers as compared to the steam sterilized ones in two groups of well-controlled hemodialysis patients. There were no significant differences in pre- and post-dialysis platelet counts of patients using e-beam-sterilized dialyzers compared to those using steam-sterilized ones. Furthermore, no statistically significant differences between pre- and post-dialysis platelet counts were found throughout the study in the e-beam-sterilized group. However, 1 out of 9 patients demonstrated significant post-dialysis thrombocytopenia in 2/4 measurements. In conclusion, our study data do not support a continuously occurring thrombocytopenic effect in patients dialyzed with e-beam sterilized membranes. Further studies are needed to determine whether and how the use of e-beam sterilization may impact the interaction between certain membranes and platelets.
Introduction
Bio-incompatibility and its associated complications have been considered major issues since the dawn of hemodialysis (HD) treatment. Despite constant advancement in HD technology during the past 50 years, membrane dialyzer material and sterilization methods remain two of the main sources of procedure-related adverse reactions. Electron-beam (e-beam) radiation has recently become a popular method of membrane sterilization (1). A significant association was reported between exposure to e-beam sterilized dialyzer membranes and thrombocytopenia in a large-scale investigation across two Canadian provinces (2). However, the authors acknowledge that the mechanism by which e-beam sterilization contributes to this platelet effect and, in addition, the clinical significance of this dialysis-associated thrombocytopenia is unclear as yet (3). Furthermore, in a recent study reported in abstract form, negligible changes in platelet count were found during HD and hemodiafiltration (HDF) with e-beam sterilized polyethersulfone dialyzers (4). The use of e-beam sterilized polysulfone dialyzers has been introduced in our dialysis unit since June 2010. In light of the above-mentioned findings, we prospectively evaluated two sterilization groups of well-controlled patients with similar demographic and dialysis characteristics, excluding patients with other factors potentially affecting platelets (mainly permanent catheter access and unfractionated heparin). The thrombocytopenic effect of the e-beam sterilized dialyzers was compared to the steam sterilized ones.
Materials and Methods
Nine patients (male/female:8/1), median age 67 (55-83) years, on maintenance HD (6 on conventional HD and 3 on HDF) for 108 (30-300) months, treated with polysulfone, e-beam sterilized dialyzers (REXEED™; Asahi Kasei Medical America Inc., New York, NY, USA) for 20 (19-20) months and 9 patients (male/female:5/4), median age 69 (61-78) years, on maintenance HD (5 on conventional HD and 4 on HDF) for 144 (18-372) months with polysulfone (FX80; Fresenius Medical Care, Bad Homburg, Germany) or polyarylethersul-fone (Polyflux™ H; Gambro, Lund, Sweden) steam sterilized dialyzers were included in the study. Unlike Polyflux dialyzers that are sterilized using standard steam sterilization process, FX-class dialyzers are subjected to the INLINE steam sterilization procedure in which both the blood and the dialysate compartments are continuously flushed with steam, ensuring excellent hemocompatibility and purity without the need for additional chemicals.
All patients were dialyzed via native fistulas or grafts and with low-molecular-weight heparin anticoagulation. Five patients in each group were receiving clopidogrel. Four consecutive monthly pre- and post-dialysis platelet and WBC count measurements were performed. The study was performed in accordance with the Declaration of Helsinki and with the approval of the local ethics committee. All patients gave informed written consent before enrollment.
Results
Baseline demographics were similar in both sterilization groups. There were no significant differences in pre- and post-dialysis platelet and WBC counts of patients using e-beam sterilized dialyzers compared to those using steam sterilized ones (Tab. I). No influence of gender, treatment mode (HD or HDF) or clopidogrel administration on platelet and WBC counts was found in any group. No statistically significant differences between pre- and post-dialysis platelet counts were demonstrated throughout the study in the e-beam sterilized group. However, 1 out of 9 patients in the e-beam sterilized group, not on clopidogrel treatment, in 2/4 post-dialysis measurements versus none in the steam sterilized group had platelet counts less than 100 × 103/μl and a decrease of more than 15%, meeting the thrombocytopenia criteria adopted by Kiaii et al (2). Furthermore, 4 other patients of the e-beam sterilized group in 1 measurement and 2 more in 2 measurements had a greater than 15% decrease in platelet count.
Platelet Count Measurements in HD Patients Using E-Beam Sterilized Dialyzers Versus Those Using Steam Sterilized Ones
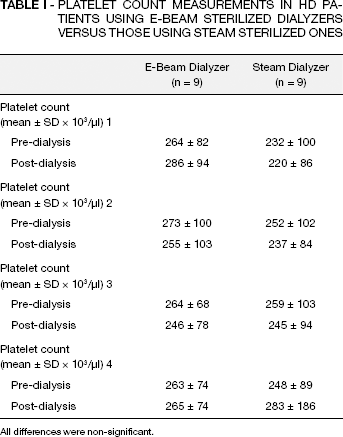
All differences were non-significant.
The platelet count percentage change in patients using e-beam and steam sterilized dialyzers is shown in Figure 1. No bleeding complications were noted in the affected patient. No significant decrease in white blood cell (WBC) counts was detected post-dialysis in the e-beam sterilized group. Three additional male patients treated with steam-sterilized dialyzers were switched to e-beam sterilized ones during the study period in order to test the hypothesis of an early thrombocytopenic reaction. These patients were not included in the study and were examined separately. No significant decrease in platelet count or WBC was found after the change to e-beam sterilized dialyzers.
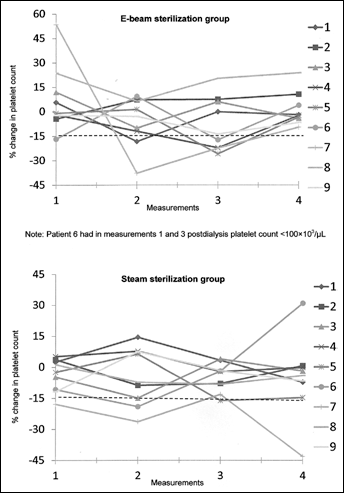
Platelet count change (%) in patients using e-beam and steam sterilized dialyzers.
Discussion
The potential risk of thrombocytopenia associated with the use of e-beam sterilized dialyzers highlighted in the study by Kiaii et al (2) in a small percentage of their patients remains relatively speculative and definitely inconclusive.
The combination of variability in patient-specific factors and subtle differences in dialyzer membrane properties and manufacturing processes may contribute to the idiosyncratic nature of the problem. Furthermore, the largely retrospective nature of the Canadian study and the incomplete data on dialyzer characteristics further complicate the interpretation of the results.
We tried to elucidate these issues by studying prospectively for a 4-month period a well-controlled group under the same dialyzer for 20 months at the onset of the study period. We also detected a small percentage of probably genetically-related thrombocytopenic patients but this effect is not stable meaning that there is additional influence of some as yet undetermined factors such as medications or incurrent illnesses. Our study data do not support a continuously occurring thrombocytopenic effect in the affected patients.
In agreement with our findings, a recent prospective, randomized, controlled, cross-over study that investigated the platelet activating effects of e-beam sterilized polyethersulfone membranes in different dialysis modes (low-and high-flux HD, low- and high-efficiency postdilution HDF) demonstrated no significant changes in the platelet count during the treatments, similar to previous observations with steam or gamma-radiation sterilized dialyzers (4). Interestingly, this study included highly compatible, synthetic dialyzers made of identical membrane materials and, furthermore, used more subtle markers of platelet activation. Therefore, our own findings, together with those by Krieter et al (4), raise questions about the link between e-beam sterilization and thrombocytopenia reported in the Canadian study (2). More studies and increased scientific vigilance are definitely needed to determine whether and how the use of e-beam sterilization may impact the interaction between certain membranes and platelets and to identify the potentially susceptible patient population groups.