
Abstract
Background
Esophagectomy after pneumonectomy has been rarely reported, mainly due to the technical difficulty in performing this surgical approach. Conventional intubation to the contralateral respiratory passage is technically challenging, while the homolateral respiratory tract is absent, making oxygenation impossible.
Methods
To overcome this problem, we used venoarterial (VA) extracorporeal membrane oxygenation (ECMO) which can help achieve gas exchange despite the collapsed lung and provide a clear unobstructed surgical field for esophagectomy.
Results
We obtained satisfactory outcomes with VA ECMO in our treated patient.
Conclusions
This technique may be an excellent option for the treatment of complex situations such as esophagectomy after pneumonectomy.
Introduction
Esophagectomy after pneumonectomy has been rarely reported, mainly due to the technical difficulty in performing this surgical operation. The conventional treatment strategy is thought to be at high risk intraoperatively, because it is not easy to obtain an adequate operative view or to achieve adequate arterial oxygenation. In order to overcome these limitations, we developed a new technique which is valuable for treatment of this complex situation. In this report we present the case of an adult patient who underwent esophagectomy after left pneumonectomy, with successful utilization of venoarterial (VA) extracorporeal membrane oxygenation (ECMO).
Clinical summary
A 72-year-old man presented with frequent episodes of dysphagia for 1 month. His medical history included non-small cell cancer of the left lung treated by pneumonectomy 12 years ago. Endoscopy (as shown in Fig. 1) and biopsy demonstrated lower esophageal squamous cancer. Endoscopic ultrasound showed that the cancer invaded the muscularis propria and several enlarged lymph nodes. Computed tomography (CT) of the chest revealed marked displacement of mediastinal structures into the left side of the chest (Fig. 2). CT of the abdomen and abdomen ultrasound examination showed nothing significant. Pulmonary function tests revealed a forced expiratory volume (FEV1) of 1.55 L (87% predicted) and diffusion lung capacity of oxygen (DLCO) of 75% predicted. As the clinical data indicated surgical resectability, the decision was made to proceed with esophageal resection.

Endoscopy demonstrated a lower esophageal cancer.
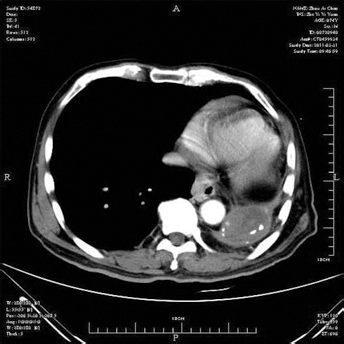
Computed tomography of the chest demonstrates shift of mediastinal structures into the left side of the chest.
Technique
Given the anatomical and physiological changes associated with the pneumonectomy, a combined, right, posterolateral, muscle-sparing thoracotomy and upper abdominal incision approach (Ivor-Lewis incision) was selected, assisted by ECMO. The patient was in a supine position, and the abdomen was entered through a subcostal muscle-cutting incision. After the stomach was mobilized, a gastric conduit was created, with a linear stapler parallel to the greater curve, and the fundus was removed with a portion of the lesser curvature. In addition, a complete lymphadenectomy was performed.
The patient was prepared for VA ECMO consisting of a Maquet Rotaflow pump and a Maquet BE-PLS 2050 oxygenator (Maquet, Suzhou, China). The cannulas were inserted into the right femoral artery (20 F) and vein (24 F) as shown in Figure 3, flushed with heparin, and clamped proximally. The cannulas were then connected to the mechanical ventilation (Bio-Console® 560; Medtronic, Minneapolis, MN, USA) which was filled with sodium chloride physiological solution. After confirming all the interfaces, the device was unclamped gently and progressively for several minutes to minimize the hemodynamic effects. Activated coagulation time (ACT) was maintained at the level of 110 s to 130 s (heparin dose was about 1/8 of the full dose, approximately 50 IU/kg body weight). After that, the oxygen source was attached and the blood flow rate through the device was maintained between 2.5 l/min and 3.0 l/min during the surgery process.
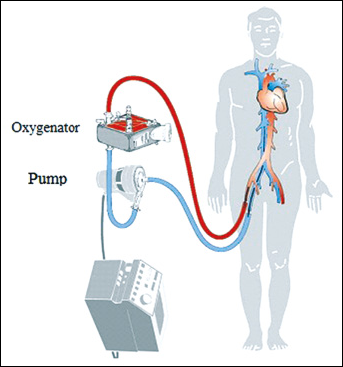
VA ECMO: Blood is pumped from right femoral vena through oxygenator and returned into a femoral artery.
Once ECMO was established, the patient was placed in the left lateral decubitus position and a right posterolateral muscle-sparing thoracotomy was performed through the fifth intercostal space. The mediastinal pleura that overlies the esophagus was incised, the azygos vein was divided, the intrathoracic esophagus was mobilized, and then the en bloc resection of the surrounding peri-esophageal tissue was performed, including mediastinal lymph node dissection. Finally an esophagogastric anastomosis was performed in the chest by proximate circular stapler (Johnson & Johnson/Ethicon, Shanghai, China).
The patient underwent uneventful and rapid esophagectomy with little blood lost. ECMO was discontinued 1 hour postoperatively when the vital signs of the patient became normal (BP: 120/61 mmHg, HR: 88/min, SPO2: 100%, PaO2: 84 mmHg, PaCO2: 40 mmHg). The patient was transferred to the ICU for respiratory care and monitoring of complications. He was discharged from the ICU 2 days postoperation and from the hospital 14 days postoperation.
Discussion
The incidence of esophageal cancer in patients with a previous history of lung cancer is rather low, ranging from 0.05% to 0.5% (1, 2). The incidence is even lower of patients who have undergone esophagectomy with a previous history of pneumonectomy. Esophagectomy after pneumonectomy is a surgical challenge (3). In this report, we developed a novel technique by using ECMO to support esophagectomy in order to reduce the risk for the patient intraoperatively. Our goal was to keep regular gas exchange while maintaining the surgical field unobstructed during operation. Some of the factors we took into consideration are listed below.
Left thoracotomy
With the conditions presented by this patient, it is common for us to think about whether the surgery can be done well by left thoracotomy incision because the left lung has been removed, resulting in sufficient space for the operation. But the reality was quite the opposite in this case: based on CT, the patient had a left collapsed chest cavity and an obviously displaced heart, which would make a left-sided approach difficult due to the poor view and limited operation space.
Transhiatal esophagectomy
As mentioned above, since left thoracotomy incision was not available, a transhiatal esophagectomy theoretically became more desirable in order to avoid the postpneumonectomy space. There was one report on a patient with post-right-upper lobectomy in which this strategy was used to perform an esophagectomy (4). In our case, the situation was quite different, as our patient underwent a pneumonectomy instead of a lobectomy, and the adhesion was much more severe, making transhiatal esophagectomy technically not feasible because of anatomic changes and adhesions after pneumonectomy and nodal dissection.
Right thoracotomy incision without artificial lung
A previous report described this method for esophagectomy (3). Advantages of a right thoracotomy approach in patients who had a previous left pneumonectomy include excellent exposure of the esophageal cancer lesion and lymph nodes. But in the process, it is difficult to maintain satisfactory lung ventilation.
Right thoracotomy incision with cardiopulmonary bypass (CPB)
With the specific points described above, we needed to think of a strategy which could provide both adequate exposure and en bloc tumor resection. To achieve this goal, the solitary lung must be out of ventilation. One possibility is to use cardiopulmonary bypass (CPB), and as we knew, CPB establishment often needs a median sternotomy incision during horizontal position. However, an esophagectomy is extremely difficult to do via this incision and position. Besides, CPB needs systemic heparinization which might cause bleeding, sometimes becoming fatal. In addition, CPB leads to blood cell destruction (5). Lastly, in the use of CPB, the salvaged autotransfusion during esophagectomy may result in the tumor spreading systematically (6). Thus, CPB assistance was not an optimal option for this patient.
Right thoracotomy incision with assisted by ECMO
ECMO is a type of extracorporeal circulation that supports the lungs, heart, or both for days to weeks in patients in intensive care with reversible life threatening respiratory or cardiac disease (7, 8). It is widely recognized that to maintain normal gas exchange perioperatively, especially intraoperatively, is a huge challenge to the performance of an esophagectomy after pneumonectomy. Conventional intubation to the contralateral respiratory passage is impossible while the homolateral respiratory tract is absent, which makes oxygenation impossible. By using ECMO we would have adequate exposure for resection, and the esophagectomy could be performed uneventfully. Moreover, ECMO requires lower levels of anticoagulation and can be used without systemic anticoagulation to reduce the risk of major bleeding. All of these factors allowed the patient to have an uneventful perioperative course and benign prognosis.
Choice of VA ECMO
VA ECMO provides both gas exchange and circulatory support. Our patient had undergone a pneumonectomy 12 years previously, which caused mediastinal shift and dense adhesions. During esophagectomy, mediastinal shift, adhesion tissue separation and heart pull led to inadequate ventilation and circulatory instability. In order to maintain satisfactory lung ventilation and circulatory output, VA ECMO was used in the patient. The advantage of this method is that it gives excellent support for the heart and the lungs.
In this case, cannulation of VA ECMO was inserted into the femoral vein and artery. The ECMO flow rate was adjusted to the minimum needed to provide adequate gas exchange and circulation support. ECMO flow range was about 1/3~2/3 of total circulating output, which is sufficient to support the heart and pulmonary function.
Conclusions
Based on the successful outcome, we believe that ECMO might become a new reliable appliance for trachea surgery, especially in esophagectomy after pneumonectomy.