
Abstract
Purpose
The quality of evidence supporting the use of therapeutic plasma exchange (TPE) in the treatment of individual diseases and disorders is often limited. Since we have experienced a growing variety of indications in our center we decided to make an inventory of our TPE population.
Methods
Single-center retrospective inventory of adult TPE-patients during a 7-year period to determine the evolution of indications for TPE, the response to treatment, and the existing evidence supporting TPE in specified settings.
Results
During a period of 84 months, 72 patients underwent 638 sessions of TPE in 91 episodes. There was no shift in frequency of TPE or level of indication. Our population consisted of 69 patients. A level I indication was seen in 41 patients (59.4%), while 14 (20.3%) had a level II indication, 8 (11.6%) had a level III indication, one had a level IV indication (1.4%) and 5 patients suffered from a condition not mentioned in the guidelines (7.2%). The response rate was inversely correlated with the level of evidence after exclusion of these 5 patients (category I 97.6%, category II 71.4%, category III 50%, category IV 0% response, p<0.01).
Conclusions
There was no shift in frequency of TPE or level of indication in our center. Controversial indications should be carefully evaluated on an individual basis and a trial of TPE cannot be solely ruled out because of lack of evidence.
Introduction
The quality of evidence supporting the use of therapeutic plasma exchange (TPE) in the treatment of individual diseases and disorders is often limited. Since many of the conditions are rare, it is unlikely that randomized controlled trials (RCT) will ever be performed (1). As we experienced a growing variety of indications in our center we decided to make an inventory of our TPE population, to determine the types of disorders for which TPE was performed and to compare the results of treatment with the level of evidence supporting TPE.
Materials and Methods
We report a single center retrospective inventory of all adult TPE patients during a 7-year period (March 2005 to February 2012). The Antwerp University Hospital is a regional tertiary referral hospital. TPE is performed at the dialysis unit of the department of Nephrology-Hypertension and/or the department of Intensive Care Medicine (ICU). Apheresis is performed for therapeutic indications such as leukapheresis in acute leukemia, and hematopoietic stem cell apheresis for transplantation as well as in the setting of a clinical trial (apheresis of monocytes in cancer vaccines). Retrospectively available data on patient characteristics, their indication for TPE, the level of evidence for every indication, additional treatment, result of treatment and survival were obtained from our central patient data system. Partial response to treatment was defined as amelioration of clinical and/or laboratory measures. Complete response was defined as complete recovery of clinical and relevant laboratory measures. We also documented the number of TPE sessions and the number of episodes of TPE (defined as a new series of sessions at least one month after the last session). Indications and level of evidence were determined according to the definitions and guidelines on the use of therapeutic apheresis published by the American Society for Apheresis (ASFA) in 2010 (2). Indication categories are reported in Table I and grading recommendations in Table II. Approval of the Institutional Review Board (IRB) was not required for this study. Data were analyzed using SPSS 20. Continuous data were expressed as mean and standard deviation. Possible differences in response and outcome were studied using chi-squared test (x2).
Indication Categories *
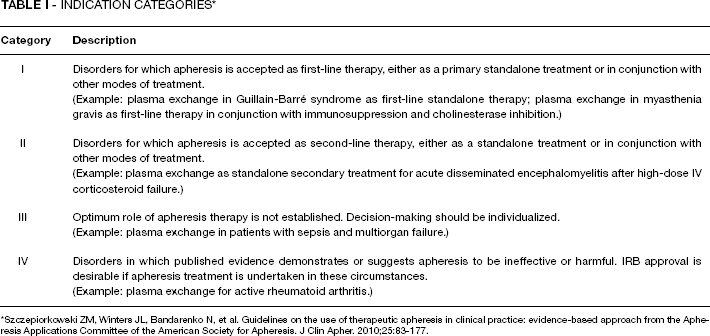
Szczepiorkowski ZM, Winters JL, Bandarenko N, et al. Guidelines on the use of therapeutic apheresis in clinical practice: evidence-based approach from the Apheresis Applications Committee of the American Society for Apheresis. J Clin Apher. 2010;25:83-177.
Grading Recommendations *
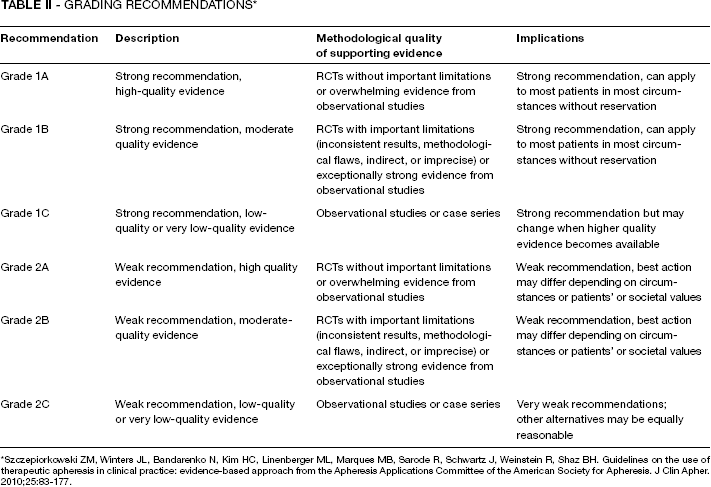
Szczepiorkowski ZM, Winters JL, Bandarenko N, Kim HC, Linenberger ML, Marques MB, Sarode R, Schwartz J, Weinstein R, Shaz BH. Guidelines on the use of therapeutic apheresis in clinical practice: evidence-based approach from the Apheresis Applications Committee of the American Society for Apheresis. J Clin Apher. 2010;25:83-177.
Results
Patient characteristics
During the 84-month study period, 72 patients underwent a total of 638 sessions of TPE in 91 episodes. Three patients were excluded. One patient was excluded because an initial diagnosis of hemolytic uremic syndrome (HUS) was afterwards changed to malignant hypertension associated thrombotic microangiopathy (TMA); another patient was excluded because of inconsistencies in the diagnosis and one patient because the initial diagnosis of chronic inflammatory demyelinating polyradiculopathy was later changed to a hereditary neuropathy.
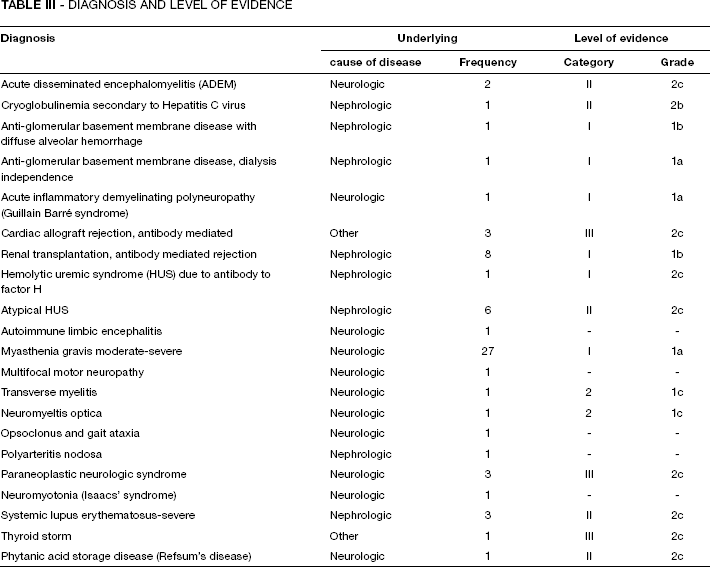
In our population 36 patients (52.2%) were male and the mean age at the first session was 51.8 (∓18.0) years. The majority of patients (N = 50, 72.5%) were treated in the dialysis department, whereas 19 patients (27.5%) were treated in the intensive care unit. Mean number of treatment episodes was 1.3 (range 1-7, median 1) and mean number of TPE sessions was 9.0 (range 1-140, median 5). Diagnoses and their frequencies are reported in Table III together with the level of evidence considering the indication for TPE. In 41 patients (59.4%) TPE was performed based on a level I indication, in 14 (20.3%) there was a level II indication, in 8 (11.6%) a level III indication, whereas 1 patient had a level IV indication (1.4%) and 5 patients suffered from a condition that was not included in the guidelines (7.2%).
Diagnosis and Level of Evidence
Outcomes
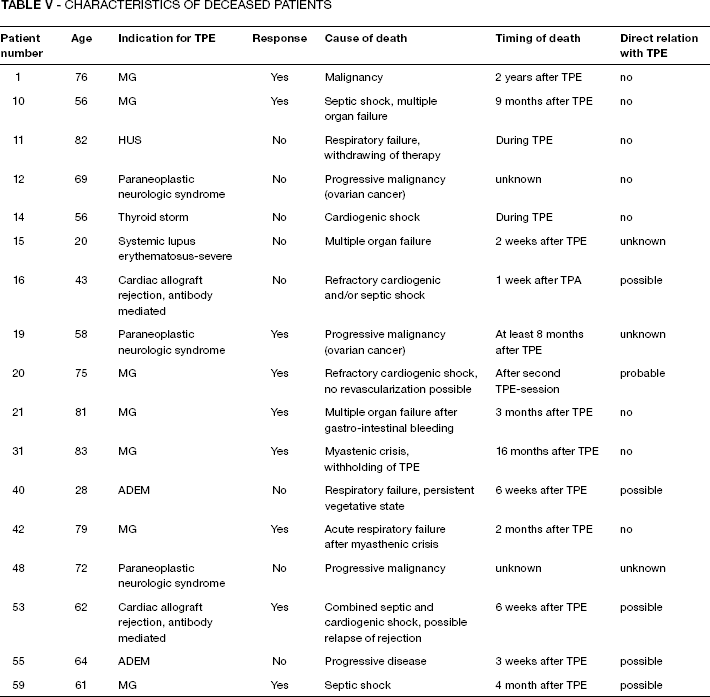
We found no trend in number of treatments per year or distribution or category of indication (Tab. IV). A complete response was observed in 17 patients (24.6%). A partial response was seen in 42 patients (60.9%) and 10 patients (14.5%) experienced no response. During a follow-up period of 4 to 89 months, 18 patients (26.1%) died. The characteristics are reported in Table V. We tried to evaluate the role of TPE in the cause of death (see Tab. V). There was no difference in response or survival between sexes (p = 0.22 and p = 0.83, respectively). Patients treated at the dialysis unit had a better rate of survival (71.1% vs. 47.4%, p<0.05) when compared to patients treated in the ICU, consistent with a less severe state of illness. In patients with a (partial or complete) response we observed a better survival rate compared to non-responders (84.7% vs. 10.0%, p<0.01).
Epidemiology

Characteristics of Deceased Patients
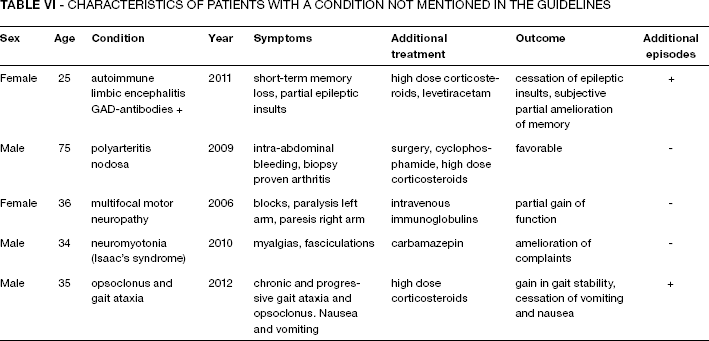
When considering categories of indication we found no difference in response (100% no indication vs. 85.7% category I-III, p = 0.35), probably because of the small number of patients with conditions not rated in the guidelines. These 5 patients are further categorized in Table VI. When these 5 patients with a diagnosis not mentioned in the guidelines are excluded, the response rate is inversely correlated with the level of evidence (category I 97.6%, category II 71.4%, category III 50%, category IV 0% response, p<0.01).
Characteristics of Patients with a Condition not Mentioned in the Guidelines
Discussion
In our population we see no trend in change of frequency or class of indication over the years. Our distribution of indications is similar as reported in the studies by Lankford et al (3) and Yeo et al (4) (our population 79.7% category I and II, 7.2% not rated, population Lankford 75-88% category I and II and 3-9% not rated and population Yeo et al 77% category I and II, 9% not rated).
With respect to non-rated conditions, autoimmune limbic encephalitis is thought to be a channelopathy, and a potential reversible component to it has been suggested. Although several treatment algorithms implement TPE for this condition, there is no randomized controlled trial evidence supporting its effectiveness (5, 6). As with our patient who presented with this disease, evaluation of clinical evolution is partially based on subjective measures, which complicate the evaluation of treatment.
TPE is also performed in patients with severe polyarteritis nodosa (PAN) (7) but authors tend to be more restrictive by citing one published RCT that did not show any benefit (8). In our patient suffering from PAN, however, we did see a benefit of combined immunosuppressive therapy and TPE. As for multifocal motor neuropathy, the underlying pathological mechanisms are unclear, but IgM autoantibodies against the ganglioside GM1 may cause changes in nodal and perinodal structures that compromise nerve conduction. Prednisolone and plasmapheresis are ineffective in most patients and may even exacerbate symptoms and are therefore not recommended (9). Nevertheless, in our patient we did see an amelioration of complaints, however subjective this improvement may be.
Neuromyotonia is another autoimmune channelopathy and TPE has been described as a second line therapy after anticonvulsants (6).
As for the case of the patient with opsoclonus and gait ataxia no clear evidence was found.
All cases considered to be non-rated indications had a favorable outcome, which suggests that in individual cases and after careful evaluation of indication and possible risks, TPE can be of benefit even in the absence of good evidence. The main problem with these diseases is the fact that many complaints can only be measured subjectively and the treatment never consisted of TPE alone.
As compared to the report of Yeo et al (4), our all-cause death is relatively high: 26.1% (our study) versus 11% (Yeo). However, Yeo does not report the time of follow-up and he questions whether mortality should be attributed to the severity of disease, suggesting TPE as the direct cause of death. In our population, however, there was only one death that was associated with TPE with a high probability - in a patient suffering from cardiac ischemia and cardiogenic shock after TPE, possibly because of fluid shifts (Tab. V, patient 20). Another five deaths were possibly caused (among other reasons) by infectious complications; therefore, a role of TPE cannot be ruled out (Tab. V, patients 10, 15, 16, 53, and 59). In theory, by removing immunoglobulins and complement, TPE can lead to an immunosuppressed state. However, literature on this subject is sparse and controversial. In a randomized controlled trial Pohl at al found no differences in infectious complications between patients treated with a regimen with or without TPE for severe lupus nephritis (10). Data on complications such as allergic symptoms, hypocalcaemia, catheter-related infections or fluid overload were not adequately documented.
TPE is usually applied in combination with other therapies such as corticosteroids or cyclophosphamide. Recent studies also suggest a benefit for the combination of TPE and rituximab in for example refractory thrombotic thrombocytopenic purpura (TTP) (11); and, with less firm evidence, bortezomib and TPE in multiple myeloma with cast nephropathy (12).
Novel techniques are gaining interest and evidence is augmenting. Potential gain is a decrease in side effects by a more selective treatment. Immunoadsorption is promising in ABO-incompatible transplantation, for example (13). Novel monoclonal antibodies such Eculizumab, which prevents complement C5 activation, may also appear to be of great benefit (14).
Our data were reviewed using the ASFA guidelines and although recent and well documented when concerning scientific evidence, a possible flaw is that the committee behind these guidelines includes physicians with training in pathology, hematology, and pediatrics but not in nephrology or neurology. As such, nephrologists are regularly confronted with a dilemma when not making the primary diagnosis but still being responsible for performing the definitive therapy, with all its attendant risks (4).
Conclusions
Besides well-known indications for TPE with strong evidence, for many diseases the indication for TPE is controversial or even obscure. In our population the response rate is indeed inversely correlated with the level of evidence, but only after exclusion of the patients with a diagnosis not mentioned in the guidelines. We suggest that controversial indications be carefully evaluated on an individual base and that a trial of TPE cannot be solely ruled out because of lack of evidence. This means that in these settings a careful, multidisciplinary review of all determining factors is obligatory and treatment under a research protocol is preferred. Newer techniques such as immune-adsorption are promising but can not be considered standard of care yet.