
Abstract
Background
In pediatric continuous renal replacement therapy (CRRT) patients, accurate ultrafiltration (UF) measurement is essential, as both over- and under-UF may result in suboptimal outcomes. Traditionally, CRRT has relied on scale-based UF measurements; however, the recent development of a continuous volumetric balancing system has allowed for the advent of scale-less CRRT.
Methods
To assess the accuracy of the volumetric balancing system, we designed a continuously measuring digital scale, which accounted for dialysate use and collected effluent, allowing us to independently measure UF volume and compare it with the machine reported UF volume.
Results
In four low weight (6.9-16.7 kg) pediatric CRRT patients, we measured the UF volume over 20 separate runs, comprising a total of 318 hours. Over this time, the total measured UF volume was 50,550 mL ± 296 mL, whereas the total reported UF volume was 50,733 mL, a difference of 183 mL ± 296 mL (0.6 ± 0.9 ml/h), or 0.4 ± 0.6%. For each patient, over 48-112 hours per patient, the differences between the total measured and total reported UF volumes ranged from -7.8 ± 1.7 ml/h to +9.7 ± 1.8 ml/h, or -6.0 ± 1.3% to +5.4 ± 1.0%.
Conclusions
In low-weight, pediatric CRRT patients, the scale-less continuous volumetric balancing system delivers accurate ultrafiltration.
Introduction
In pediatric acute kidney injury (AKI) patients, continuous renal replacement therapy (CRRT) is widely used to manage fluid and electrolyte abnormalities. Studies have shown that both fluid overload (1) and hypotension (2) at dialysis initiation are independent risk factors for mortality in pediatric CRRT patients. It is likely that continued intradialytic fluid overload and/or hypotension is also associated with poor outcomes in this population. As such, proper volume management, appropriate ultrafiltration (UF), and the accurate measurement of UF during CRRT are important, as both under-UF, possibly resulting in fluid overload, and over-UF, possibly resulting in hypotension, may lead to suboptimal outcomes. Smaller patients are especially at risk, as slight UF errors may result in relatively large changes in fluid balance and/or hemodynamic status.
In order to achieve the appropriate UF volume during CRRT, scale-based technology, allowing for the direct measurement of ultrafiltrate, has traditionally been used. However, a CRRT machine (NxStage® System One™, Lawrence, MA) that utilizes a scale-less, continuous volumetric balancing system has been available for use since 2004 (3). Within the machine cartridge, coupled replacement fluid and waste pumps continuously fill dual volumetric balancing chambers, while a UF pump enables net fluid removal (4). In vitro simulations have demonstrated the accuracy of the volumetric balancing system; however, it has not been evaluated in vivo in low weight pediatric patients, a population in which inaccurate UF may be most likely to adversely affect clinical status. Thus, in order to assess the in vivo accuracy of the volumetric balancing system in small pediatric patients, we designed a continuously measuring digital scale, which accounted for dialysate use and collected effluent, allowing us to independently measure UF volume and compare it with the UF volume reported by the dialysis machine. We hypothesize that the volumetric balancing system UF is accurate to within 10% of our gravimetric UF measurements.
Materials and Methods
We constructed a two-tier, hanging, continuously measuring digital scale (Fig. 1). The digital scale (25 kg capacity or 45 kg capacity Salter Brecknell® ElectroSamson™ models (Fairmont, MN, USA), with manufacturer-reported accuracies of ±0.02 kg and ±0.05 kg, respectively) hung from a six foot tall aluminum pole on wheels. From the scale's hook, we hung a two-tier, multi-armed IV pole that was able to hold dialysate bags and effluent collection bags.

In order to assess the accuracy of the scale-less volumetric balancing system, we designed a two-tier, hanging, continuously measuring digital scale.
Up to four 5-liter Prismasate™ dialysate solution bags (Gambro, Daytona Beach, FL, USA) were hung from the upper level of the IV pole. At all times, the only dialysate running into the machine was from the dialysate bags hanging from the scale. From the bottom level, up to four 5-liter bags were hung to collect the dialysate effluent (Fig. 2). We connected the effluent drainage line to the effluent collection bags using the branched dialysate tubing. As we connected the effluent drainage line to the effluent collection bags, we noted the weight displayed on the digital scale, ensuring that all of the bags were freely hanging and not in contact with the scale apparatus pole. We also noted the time, as shown on the machine's display. Several hours later, at the end of the run, we noted the digital scale weight and the machine time, then disconnected the effluent line from our collection bags. As only dialysate hanging from the scale flowed into the machine, and as all effluent was collected in our collection bags, the difference between the weight at the beginning of the run and the weight at the end of the run represented the weight of ultrafiltrate removed from the patient. Using the machine's on-screen history function, we calculated the reported UF over the same time period, then compared our directly measured UF weight to the UF volume reported by the machine.

Dialysate solution bags were hung from the top level, and effluent collection bags were hung from the bottom level. This scale design accounted for dialysate use and collected effluent.
In order to validate the accuracy of our scale, in one patient, we also used a 20 kg capacity digital infant scale, accurate to ±0.005 kg, to directly measure UF weight. Before each run using the infant scale, full dialysate bags and empty effluent collection bags were weighed on the infant scale. At the end of the run, the empty dialysate bags and full effluent collection bags were again weighed on the infant scale. The difference between the weight at the beginning of the run and the weight at the end of the run represented the weight of ultrafiltrate removed from the patient, which we compared to the UF volume reported by the machine over the same time period.
Four pediatric continuous veno-venous hemodialysis (CVVHD) patients were enrolled in the study; all were on the NxStage® machine with the hemofilter 400. For each patient, multiple runs were conducted. For each run, the measured UF weight (X) was calculated as the difference between the scale weight at the end of the run (A ± a) and at the beginning of the run (B ± b); the associated additive error (x) was calculated as follows:
This study was approved by the institutional review board, and consent was obtained from the parents of the study participants.
Results
Table I shows patient characteristics and CRRT parameters. Ordered UF rates varied and were changed as needed by the patient's primary care team; over the course of the study, actual ultrafiltration rates ranged from approximately 15 to 21 ml/kg per h. Four to six runs were conducted for each patient, ranging in length from 4 h to 26 h, with a total of 20 independent runs. The runs occurred at various times of day, with various start and stop times. During the runs, there were no interruptions of CRRT or clinically significant events. Table II shows the differences between measured and machine reported UF, for each run, for each patient, and cumulatively.
Patient Characteristics And Crrt Parameters
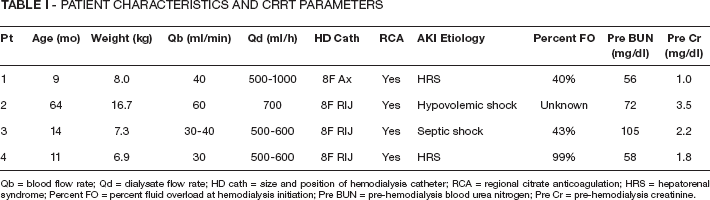
Qb = blood flow rate; Qd = dialysate flow rate; HD cath = size and position of hemodialysis catheter; RCA = regional citrate anticoagulation; HRS = hepatorenal syndrome; Percent FO = percent fluid overload at hemodialysis initiation; Pre BUN = pre-hemodialysis blood urea nitrogen; Pre Cr = pre-hemodialysis creatinine.
Over the cumulative 318 h that data was collected, the measured UF volume was 50 550 ± 296 mL, and the reported UF volume was 50 733 mL; the difference was 183 mL ± 296 mL (0.6 ± 0.9 ml/h), or 0.4 ± 0.6%. For each of the 20 runs, the reported UF volume correlated well with the measured UF volume (r = 0.99) (Fig. 3). The Bland-Altman plot shows little systemic bias (mean difference of only +1.7 ml/h) and little proportional bias (r = 0.22) (Fig. 4). Among the enrolled patients, the individual differences between machine reported UF and measured UF ranged from -7.8 ± 1.7 ml/h to +9.7 ± 1.8 ml/h, or -6.0 ± 1.3% to +5.4 ± 1.0% (machine reported UF volumes ranging from 6% less than to 5.4% greater than the actual UF volumes). These UF discrepancies translated into percent fluid balance errors for each patient ranging from -9.9 ± 2.2% (over 93 h) to +5.8 ± 1.1% (over 48 h).
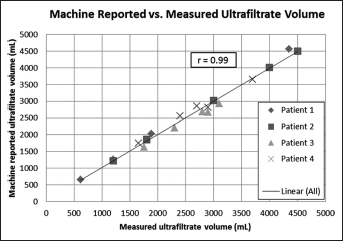
Correlation of the machine reported and measured ultrafiltrate (UF) volumes.
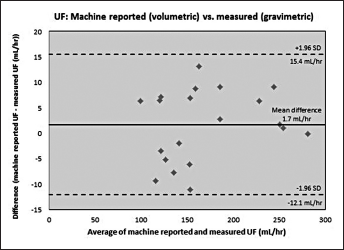
Bland-Altman plot comparing the differences between the machine reported (volumetric) and measured (gravimetric) ultrafiltrate (UF) values. Mean bias is denoted by the solid line, and the limits of agreement are denoted by the dotted lines.
For the patient in whom we also used the infant scale, accurate to ±5 grams, we conducted eight independent runs, ranging in length from 7 h to 20 h. The total run time was 108 h, over which the measured UF volume was 15 605 ± 25 mL, and the reported UF volume was 15 712 mL; the difference was 107 ± 25 mL (1.0 ± 0.2 ml/h), or 0.7 ± 0.2%, thus showing our hanging scale apparatus to be as accurate as the infant scale (data not shown).
Discussion
In order to optimize outcomes and minimize continued fluid overload and/or hypotension, recent attention has focused on eliminating the potential for either inadequate or excessive ultrafiltration during CRRT. Our novel, two-tier, continuously measuring digital scale allowed us to assess the ultrafiltration accuracy of a volumetric balancing fluid management system. This in vivo study demonstrates that this volumetric balancing system provides accurate ultrafiltration, over prolonged periods of time, in small pediatric CRRT patients.
Appropriate fluid management in low-weight pediatric AKI patients is critical. Observational studies of pediatric AKI patients requiring CRRT have found that fluid overload (1, 5–7) at CRRT initiation is associated with increased morbidity and mortality. In a multicenter prospective study of 297 children requiring CRRT, Sutherland et al found that patients with at least 20% fluid overload had an adjusted mortality rate over eight times that of patients with less than 20% fluid overload (1). As excessive fluid administration may contribute to fluid overload and suboptimal outcomes in AKI patients, fluid should be considered a drug, with dose modifications made based on AKI etiology (prerenal vs. intrinsic) and AKI stage (early vs. established). The degree of fluid overload in AKI patients should be calculated and monitored over time. In this manner, quantifying fluid overload may help guide clinical management, aiding physicians in modifying IV fluid regimens, deciding when to initiate renal replacement therapy, and establishing ultrafiltration goals.
In addition to fluid overload, hypotension at dialysis initiation is a risk factor for morbidity and mortality in pediatric CRRT patients (2). Furthermore, intradialytic hypotension, which may be contributed to by excessive ultrafiltration, is associated with increased morbidity and mortality in dialysis patients (8, 9). As such, ultrafiltration rates and fluid status goals much be constantly re-assessed, aiming to avoid both inadequate and excessive ultrafiltration, which may contribute to continued fluid overload or intradialytic hypotension, respectively, resulting in worsened clinical outcomes.
Appropriate ultrafiltration management in CRRT patients depends on accurate ultrafiltrate measurement. In vitro simulations of the volumetric balancing system, targeting 4 kg of net fluid removal over 12 h to 24 h, found that daily fluid balance was accurate within 0.5 kg, and that the average hourly fluid balancing accuracy was 9.2 ± 14.8 ml/h (10). Although smaller UF volumes were targeted in our patients, our in vivo results are similar to these simulations. Furthermore, the percentage UF differences for each run ranged from -8.4 ± 2.7% to +7.7 ± 1.4%, and for each patient ranged from -6.0 ± 1.3% to +5.4 ± 1.0%, all within the product specified UF accuracy of ±10% (11).
The patient percent fluid balance errors ranged from -9.9 ± 2.2% (over 93 h) to +5.8 ± 1.1% (over 48 h), representing an actual percent fluid balance ranging from 9.9% more negative to 5.8% more positive than that calculated with machine reported values. The hourly patient percent fluid balance errors ranged from -0.11 ± 0.02% to +0.12 ± 0.02%. As CRRT may be provided for days at a time, the additive effects of these percent fluid balance errors may become significant; however, it is unlikely that the magnitude and direction (positive or negative) of the hourly percent fluid balance error would remain constant over time. As shown in Table II, differences between machine-reported UF and measured UF values were positive for some runs and negative for other runs in two patients; they were positive for all runs in one patient, and negative for all runs in one patient. It is unclear why the differences were all positive in one patient and all negative in another patient, and given the small sample size, difficult to draw conclusions regarding this observation.
Run Data
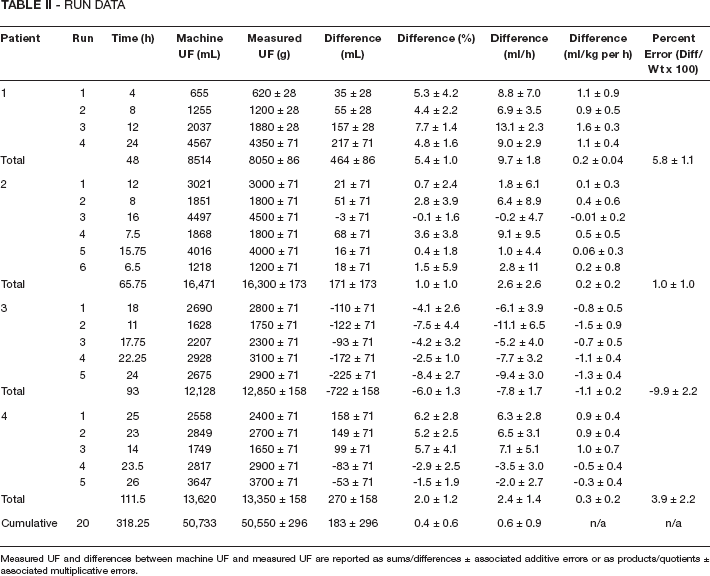
Measured UF and differences between machine UF and measured UF are reported as sums/differences ± associated additive errors or as products/quotients ± associated multiplicative errors.
Two technical issues with our scale design should be mentioned. Firstly, we did not account for the effluent in the tubing between the dialysis cartridge and the effluent collection bags. Although this was likely a relatively small volume of fluid, it may have contributed to slight underestimations of our gravimetric UF values. Secondly, we compared the measured UF weight to the reported UF volume, assuming that the effluent density was 1 g/ml. However, density varies with temperature; at room temperature (20-25°C), the density of water ranges from 0.9970 g/ml to 0.9982 g/ml. Yet, we cannot assume that the effluent had the same density as water. The effluent consisted of warmed, spent dialysate and ultrafiltrate, both containing unknown solute concentrations. Given that the temperature and biochemical composition of the effluent was unknown, the effluent density was also unknown, but unlikely to be 1 g/ml, therefore contributing to some error between the measured UF weights and reported UF volumes.
Our study had several limitations. We included only four patients; however, with these four patients, we conducted a total of 20 independent runs using the scale, amounting to 318 total hours of data. We were unable to assess the patients’ weight changes during the runs, as weights were not recorded upon run initiation and termination. Also, we did not assess how accuracy was affected by filter age, transmembrane pressure, or circuit pressures. Older filters, with likely more clotting, may result in less effective UF, requiring higher transmembrane pressures or longer dialysis duration in order to obtain the desired UF volume. However, the focus of our study was on how well the machine-reported UF values correlated with the actual UF volumes, regardless of how close these values were to the desired, programmed UF volumes.
Further studies of interest regarding the accuracy of the volumetric balancing system may include how the accuracy is affected by varying UF rates. During several runs, the ordered UF rates varied, changed as needed by the primary care team based on clinical status. In the setting of varying UF rates, it would be of interest to compare more instantaneous gravimetric and volumetric UF values; however, for each run, we recorded only total UF values, without noting hourly UF values during the run. Also, it may be of interest to assess how accuracy varies over the course of the day, as environmental temperatures change. As the majority of our runs lasted more than 12 h and occurred during different times of the day, we were unable to classify the runs as solely “daytime” or “nighttime,” or as “before noon” or “after noon,” in order to assess diurnal variation. Using our scale apparatus, we assessed the in vivo accuracy of the scale-less volumetric balancing system; however, we did not compare this machine to a scale-based CRRT system. Although future studies could explore this issue, given the UF accuracy demonstrated here, it is unlikely that a clinically significant difference would be found in favor of either system. However, there are some potential advantages in utilizing a scale-less system, such as the ability to pre-hang dialysate bags, or simply add bags as needed, and the lack of effluent collection required. Additionally, conventional scales are sensitive to movement and other environmental disturbances which may affect accuracy. Such practical comparisons were not addressed in the current study.
Conclusions
In summary, this study demonstrates that the in vivo ultrafiltration accuracy of the volumetric balancing system is comparable to in vitro studies and within the limits of the product-specified UF accuracy. Although future studies are needed in order to explore the possible practical advantages of using a scale-less CRRT system, the volumetric balancing system provides accurate UF in the management of small children with acute kidney injury.
Footnotes
Ackowledgements
We thank Omar Morales, of the Ronald Reagan UCLA Medical Center Clinical Engineering department, for his help in the design and construction of the scale apparatus.