
Abstract
The monitoring of ionic dialysance in hemodialysis allows early detection of arterio-venous fistula stenosis. One limitation to the practical use of ionic dialysance is that the analysis is very time consuming on a majority of normal cases.
The purpose of the study is to evaluate the utility of an expert system reproducing a human analysis and allowing continuous monitoring of the ionic dialysance by helping the physician to focus his or her expertise on the abnormal cases.
The method is based on a Bayesian model that analyzes the blood flow rate, the ionic dialysance, and the venous and arterial pressures measured on the extra corporeal circuit.
The clinical evaluation was performed on 90 dialysis patients at the hospital dialysis center of Saint Brieux in France with a history of at least four consecutive months of validated recording. The retrospective automated analysis was evaluated in comparison to vascular access problems identified from invasive investigation or treatment. The sensitivity of the automated analysis is 92% with a specificity of 75%.
As a conclusion we suggest that this expert system could be used in a continuous vascular access monitoring procedure consisting in a weekly review of the patient population at the dialysis center. The patients with the highest risk score need a further investigation of their historical data and their medical history in order to decide whether or not to perform an invasive intervention.
Keywords
Introduction
In hemodialysis, ionic dialysance is an indicator of small-solute clearance based on a conductivity measurement in the inlet and outlet dialysate. The continuous monitoring of ionic dialysance has been proposed successfully in hemodialysis patients as a tool for early detection of arteriovenous fistula stenosis in order to prevent the fistula thrombosis that may lead to the loss of the fistula as a vascular access (1, 2). This situation may require the long-term use of a central catheter with detrimental outcomes on the patient morbimortality.
We have set up a surveillance procedure based on the weekly overview of a combination of historical graphs of independent parameters giving a reflection of the function of the vascular access. These include the blood flow rate, the ionic dialysance, and the venous and arterial pressures measured on the extra corporeal circuit. These parameters are measured repeatedly, automatically, and non-invasively on dialysis monitors at each dialysis session. They are recorded on a database that is processed by Vascontrol software (Gambro Industries, Meyzieu, France). This software permits a rapid review of a big population of dialysis patients in order to identify the few patients with aspects suggesting a fistula stenosis. The analysis is done by a trained operator who is able to identify the aspects typical of vascular access dysfunction. This surveillance procedure has been implemented successfully in the early detection of arteriovenous fistulae dysfunction (3-6).
The increased amount of collected data from medical devices can help to improve care quality. This is the case for ionic dialysance, which can allow early detection of arteriovenous fistulae dysfunction. Nevertheless, this raises the problem of the time and expertise required for the identification of the suspicious aspects and therefore the need for new tools for efficiently analyzing the data. Expert systems are tools for helping in data management by reproducing an expert analyzing process on a large amount of data, thus allowing the practitioner to focus on the abnormal cases.
An expert system has been developed in order to detect automatically if the fistula is failing by simulating human analysis for identifying the suspicious aspects in the measured parameters.
This expert system was validated in a retrospective study on a population of dialysis patients on which all the significant vascular access events on the arteriovenous fistula were carefully recorded. The vascular access parameters measured on the dialysis monitor were downloaded into the Exalis Database.
Materials and Methods
In this section we present an expert system based on a Bayesian model to classify hemodialysis sessions according to the risk related to an arteriovenous fistula.
Background on Bayesian models
Bayesian models allow a macroscopic formalization of diagnostic tasks in which indicators are represented as random variables and inference rules are described by conditional probabilities. In the Bayesian interpretation, the probability is the belief that one has in the relevance of a hypothesis. The probabilistic approach allows for reasoning under uncertainty (7) and for fusing prior knowledge with new clinical information in order to evaluate the current state of the patient.
The model we use, called the Hidden Markov Model (HMM) (8), is formally defined by a set of random processes, corresponding to the clinical inputs (Yt) that are observed and to the state of the patient (Xt) that is considered as hidden. The clinical inputs (Yt) are conditioned by the state variables (Xt) and the relation between them is described by the conditional probability P(Yt | Xt). The dynamics of the process, evolving on a discrete time base, is defined by the conditional probability P(Xt+1 | Xt). A graphical representation of a HMM is given in Figure 1. Here we make the Markovian hypothesis that the current state is fully conditioned by the previous state or, in other words, that the current state is conditionally independent of the past, given the previous state:
Graphical representation of a Hidden Markov Model (HMM), defined as a hidden random process Xi conditioning an observed random process Yi. Each hidden variable Xi is conditioned by its temporal predecessor Xi-1.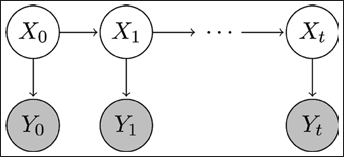

The conditional probabilities are called the parameters of the model and can be defined from expert knowledge or learned from a dataset. Inference algorithms allow the posterior probability P(Xt | Y0, Y1, …, Yt) to be evaluated, describing the belief one can have on the state of the patient given all the past and current clinical observations.
In an HMM the state variable (Xt) is discrete, whereas observations (Yt) can be either discrete or continuous. For a continuous (Yt) the parameters P(Yt | Xt) are probability densities, usually represented by a mixture of Gaussian distributions (a weighted sum of normal laws).
HMMs have been successfully used in the telemonitoring of patients treated by hemodialysis or peritoneal dialysis (9, 10).
Model for fistula diagnosis
The assessment of the arteriovenous fistula is made on a three-score scale that corresponds to the hidden state (Xt) of the model. The discrete possible values of Xt are:
score 0, no risk, score 1, mild risk, score 2, high risk.
The evaluation of Xt is made at the end of a dialysis session (Dt), considering the history in past sessions of four indicators:
The blood flow rate (QBt), The ionic dialysance (DIt), The venous pressures measured on the extra corporeal circuit (PVt), The arterial pressures measured on the extra corporeal circuit (PAt).
As illustrated in Figure 2, these indicators are filtered in order to generate two multi-dimensional inputs Y1t and Y2t for the Bayesian model:
Y1t is a four-dimensional vector composed of the four raw indicators Y2t is a three-dimensional vector composed of the daily variation of the dialysance, the daily variation of the arterial blood pressure, the daily variation of the venous blood pressure.
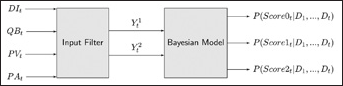
Global Process. The clinical indicators DIt QBt PVt and PAt are filtered in order to produce a sequence of observations Dt = (Y1t, Y2) representing the dialysis sessions as inputs of the Bayesian model.
The model and its parameters were adapted using a training database with 2 662 examples labeled by a single human expert. Each example of the database is composed of a sequence of dialysis session (D1,…, Dt) labeled with the corresponding risk score at the end (i.e., the value of Xt). The database was divided so as to keep 1 458 examples for the training and 1 204 for the validation. This is a usual practice for model adaptation so as to validate the model on samples that were not seen during the training.
The observation model is a Gaussian mixture composed of three multivariate Gaussian distributions for each one of the observations variables (Y1 and Y2). The Gaussian mixture model was adapted by maximizing the likelihood of the training samples with the Expectation Maximization algorithm. The dynamics of the model, defined by the transition probabilities, was tuned manually.
The model and its double blind validation against the human expert were presented in (11). The next section presents the analysis of the results obtained by the expert system on a retrospective study by comparing the score given by the model to the clinical reality in the medical history of the patients.
Validation of the expert system in a retrospective study of a dialysis patient population
This expert system was implemented retrospectively using the records of the patients included in the study. The main purpose of the automated analysis in a practical use is to eliminate the normal cases without producing false negatives. The expert system is said to be efficient when it delivers a score 2 in the period before a vascular access problem identified by an invasive investigation or treatment such as a fistulography or angioplasty (sensitivity criteria). The expert system is said to be efficient when it does not deliver a score 2 in periods without any problem in the vascular access (specificity criteria).
The clinical evaluation of the system was done on dialysis patients at the hospital dialysis center of Saint Brieuc in France who had a history of at least four consecutive months of validated recording on Exalis of the vascular access related parameters (QB, DI, PA, PV) between January 1, 2009 and June 30, 2010. On 90 patients with arteriovenous fistulae, that represents a total of 99 patient years of fistulae surveillance.
During the study period, among these patients there were 7 hospitalizations on 4 patients, 52 days of hospitalizations; 68 Doppler measures on 40 patients; 89 Transonic measures on 49 patients; 9 fistulographies on 8 patients; and 44 angioplasties on 31 patients.
On patients with arteriovenous fistula with focused analysis on periods with significant episodes involving vascular access (such as stenosis identification, thrombosis episode, fistulography, angioplasty, hospitalization for vascular access trouble), there were 49 episodes in 38 patients.
Results
Specificity and sensitivity calculations are detailed in Table I.
Sensitivity And Specificity Of Stenosis Or Thrombosis Identification
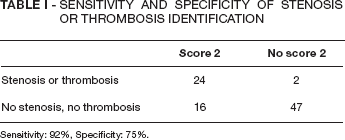
Sensitivity: 92%, Specificity: 75%.
Sensitivity criteria
True positives (Fig. 3)
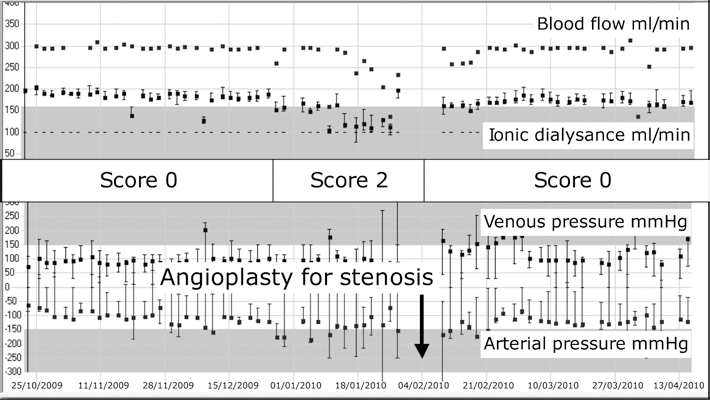
Example of true positive. Rapid decrease of ionic dialysance and big variations of arterial pressure from January 15 to February 1, 2010. Score risk 2 given by the expert system. Fistula was treated by angioplasty on February 4, 2010. The surveillance parameters returned to normal values.
In 24 cases, a score 2 of the expert system was reported before the onset of the fistula stenosis. The fistula was treated by angioplasty and access patency occurred either immediately or after a temporary period of single-needle treatment.
Two cases of full thromboses were predicted by the expert system. In these two cases, angioplasty was performed with restoration of fistula patency immediately in double-needle treatment and after a period of single-needle.
False negatives
One case of thrombosis was not anticipated by the expert system. This thrombosis was related to a sudden blood pressure drop. A thrombectomy was performed on a healthy blood vessel; the recovery of fistula patency was immediate after intervention with double-needle treatment, along with normal values of blood flow dialysance and extra corporeal pressures.
One case of sub-clavian stenosis was not detected by the expert system. Sensitivity = 24 / (24 + 2) = 0.92.
Specificity criteria
True negatives (Fig. 4)
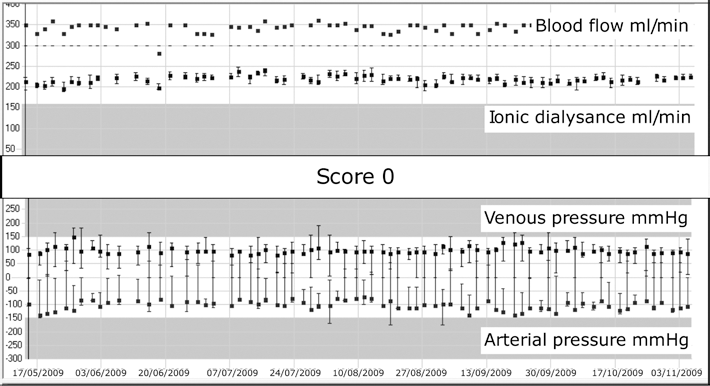
Example of true negative. Historical profile of blood flow, ionic dialysance, venous pressure and arterial pressure over a 6-month period. All the parameters are stable and in the normal range. Score risk 0 all the way through given by the expert system.
These included 47 patients without score 2 and without stenosis or thrombosis. In 16 of them, angioplasty was prescribed following clinical criteria, whereas the risk score of the expert system was 0, the angioplasty did not improve anything in the patency of the fistula:
2 cases of fistula aneurism 2 cases of fistula overflow 1 case of fistula infection 1 case of dialysance variability due to a blood pressure variability in a patient on daily dialysis 3 cases of forcasted surgical control of the fistula 1 case of dilatation with the goal to improve a low dialysance 1 case with edema and collateral circulation 1 case of vascular theft 1 patient starting dialysis treatment with fistula under maturation 3 cases of suspicion of stenosis not evidenced during intervention without any improvement after intervention. In the 31 others, no score 2 and no invasive intervention on the fistula.
False Positives
There were 16 patients with a score 2 and no stenosis, no thrombosis.
In five patients, score 2 was reported in a short period (less than one week), corresponding to a temporary, reversible difficulty in the fistula puncture.
Out of the other 11 patients who experienced a more prolonged score 2 period, there were three cases of switching to a single needle with an artefactual drop of blood flow, ionic dialysance, and drift of extra corporeal pressures; and three cases of a sustained decrease in ionic dialysance due to an increase of hematocrit related to the EPO prescription.
In five patients, score 2 was reported due to a significant decrease in ionic dialysance or drift of the extracorporeal pressures. The troubles disappeared without any intervention on the vascular access.
Discussion
The significant fistula dysfunctions reported during this study were all predicted by the expert system except one case of thrombosis that occurred suddenly following a blood pressure drop. This kind of thrombosis is classified as an accidental thrombosis, occurring on healthy blood vessels, without previous stenosis, following an external factor that could be in other cases a hemoconcentration or a compression. In 17 cases, angioplasty was prescribed on clinical criteria or in a prophylactic process, without any stenosis evidenced during the procedure. The sensitivity of the expert system was quite satisfying in this study.
Reggarding the score 2 occurrences in patients without any fistula dysfunction, most of them had a clear explanation for this in their recent medical history, and subsequently did not require any further invasive investigation. In the others, the score 2 was not explained by the medical history of the patients but by a big drift in the ionic dialysance and/or the pressures in the extra corporeal circuit. In these situations, the “human expert” would also have given a score 2. In any case, these drifts may lead to a detrimental situation that would require intervention or at least further investigation.
A drop in ionic dialysance makes the delivery of the right dialysis dose impossible. Too high venous pressures or too low arterial pressures make the implementation of the prescribed blood flow rate difficult.
Conclusions
The model we developed is not a mathematical model of a physiological phenomenon but rather a macroscopic model of a human medical way of reasoning. The goal is obviously not to replace human expertise but to make it possible for the practitioner to focus on abnormal cases, obviating the need to worry about the other cases that have been analyzed and considered normal by the expert system. The expert system tested in this clinical study proved to be an efficient tool for the early detection of arteriovenous fistulae stenosis. As a first step, the patients with score 2 identified automatically by this software deserve an in-depth investigation of the historical curves of the vascular access parameters combined with an investigation of the recent medical history. This would indicate whether to prescribe further invasive investigation or an intervention meant to prevent the onset of the fistula thrombosis.
The less critical cases without an urgent threat to the vascular access correspond to a situation the delivery of an adequate dialysis dose making impossible or difficult. In this respect, they deserve particular attention in order to identify the “weak point” of the fistula that could be a decreased access flow or a recirculation.
We suggest that this expert system could be used in a continuous vascular access monitoring procedure consisting in a weekly review of the patient population of the dialysis center. The patient population is ranked according the risk score. The patients with the highest risk score require further investigation of their historical graphs and their medical history in order to decide whether or not to perform an invasive intervention.
Footnotes
Acknowledgements
The author would like to thank Dr. Corina Stanescu, nephrologist at Hospital Yves Le Foll - Saint-Brieuc, France, for providing data and their retrospective validation.