
Abstract
Purpose
Many novel materials have been developed such as composite resin, ceramic, zircon or metal-supported ceramic for use in aesthetic restoration of primary teeth and permanent teeth with extensive crown damage. The aim of the present study was to compare microtensile bond strengths on materials using the microtensile bond strength test.
Materials and methods
The microtensile bond strength on the primary tooth dentin was measured on extracted primary teeth using an indirect method and fracture patterns were evaluated.
Results
The analysis of bond strengths using the Mann-Whitney U-test did not show significant difference between the rank averages of the compomer and composite resin (p = 0.741). The dentin sections, from which test samples were obtained, contributed to the bond strength; dentin samples obtained just above the pulp had lower bond strength, and the difference was statistically significant (p = 0.005). The adhesive type fracture was the most prevalent fracture type for both materials.
Conclusions
When the chemical, physiological, and micromorphological differences between primary and permanent teeth are taken into consideration, the success of the materials used for restorations can be different between primary and permanent teeth. Therefore, materials used in the dentistry must be evaluated separately for primary teeth.
Introduction
With technological developments, there has been a growing interest in recent years in restoring tooth color in the back teeth so as much as in the front teeth. Many novel materials have been developed such as composite resin, ceramic, zircon or metal-supported ceramic for use in aesthetic restoration of the primary teeth and permanent teeth with extensive crown damage.
It is known that composite resins are widely preferred due to the fact that composite resins allow for more conservative and direct placement compared to other materials, and restoration is completed in only 1 session (1). In addition to the known disadvantages of the composite resin restorations, discoloration or secondary caries in the tooth tissue may occur as the result of micro-leakage, which may even cause undesired conditions that lead to tooth loss (2–4). The large size of the cavities and preparation (5), binding agents used, mounting materials (6), filling materials (7, 8), and restoration techniques (9, 10) considerably affect the occurrence of micro-leakage. Extra-oral polymerization of the resin composite or the use of layering technique in the restoration of large size cavities can avoid polymerization shrinkage and associated problems (11). An incomplete polymerization process is also among the factors affecting the success of the treatment. Secondary polymerization by heat- and/or pressure-curing strengthens the physical properties of the material, the process that prevents the formation of monomers and associated problems that could arise (11). Inlay/onlay systems using composite resin or ceramic blocks combine the advantages of the 2 methods.
In pediatric patients, cavity preparations that do not fit traditional cavity preparation rules can be performed in large caries. The isolation problems during restoration, limited working time and limited compliance due to the young age of the patient, and consequently the increased number of sessions pose a problem in the treatment of pediatric patients. It has been emphasized that indirect restorations would minimize the abovementioned problems due to a lower risk of contamination, shorter time spent in the clinic, and the possibility of performing cementing for multiple restorations (12, 13).
The aim of the present study was to compare microtensile bond strengths and fracture types of compomer and composite materials using the microtensile bond strength test on primary teeth onlay restorations with different dentine depths.
Materials and methods
Microtensile bond strength on the primary tooth dentin was measured on extracted primary teeth that were restored with compomer and composite resin materials using an indirect method and fracture patterns were evaluated.
Preparation of the teeth
The test samples, 10 recently extracted, sound, primary molar teeth were collected and placed in 10% formol solution. The periodontal tissues and other clutter on the teeth were removed using a curette. The teeth were polished with a pumice and plaster-alcohol, and the roots of the teeth were dissected to 2 mm apical of the enamel-cement junction using a diamond separator in water as the coolant. The crown section of the teeth was attached to 2 × 2 × 3 mm acrylic resin blocks (Panacryl; Ethicon/Johnson & Johnson) with cyanoacrylate resin (Pattex; Henkel).
The crowns of the teeth were dissected from the occlusal surface to the pulp parallel to the occlusal surface using a diamond separator in the water. The smear layer on the dentin surface was removed with 600-grit rubber to obtain a standardized flat surface. The samples were randomly assigned to 2 groups (n = 10) according to the restorative materials to be used in the study (Filtek™ Z250; 3M ESPE, and Dyract eXtra; Dentsply).
Preparation of restorations
A hybrid composite and compomer was used in the preparation of the onlay restorations. Same-sized molds were used to prepare 3 mm-thick onlays. Glass cement was placed at the bottom of the mold having 2 openings in both sides. Three layers of composite and compomer material were placed in the molds over a clear tape using cement spatula, and each layer was light-cured for 40 seconds (Blueswan). Prepolymerized onlay restorations were placed in a Lumamat 100 polymerization furnace for the secondary polymerization.
Group I
Using the third program of the polymerization furnace, composite onlay restorations were subjected to secondary polymerization for 25 minutes, including the preliminary program for 10 minutes, heat-curing for 10 minutes and cooling for 5 minutes.
Group II
Using the second program of the polymerization furnace, the compomer onlay restorations were subjected to secondary polymerization for 11 minutes including the preliminary program for 10 minutes and cooling for 1 minute.
Attachment of the restorations
An 8-mm round-shaped adhesive tape was placed on the teeth surface before the cementation procedure in order to ensure a fixed film thickness of 100 μm for resin cement and to provide a homogeneous resin cement layer. Multilink resin cement was mixed at a ratio of 1:1 and applied on the tooth surface. Then, the prepared onlay restorations were placed on the resin cement and light-cured from all directions for 40 seconds.
Measurement of microtensile bond strength
Rod-shaped samples with a surface area of 1.00 ± 0.03 mm were obtained from the dentin section of each material above and lateral to the tooth pulp. The samples were examined under stereomicroscopy (SZ-PT Olympus) at x 20 magnification, and a total of 48 samples (25 samples from the Z250 composite group and 23 samples from Dyract eXtra group) were selected.
Before performing the microtensile bond strength test, the bond surface area of each sample was calculated. Rod-shaped samples were attached from both sides to the microtensile test device (Bisco) using cyanoacrylate adhesive. The samples were placed in a test device with a loading speed of 1 mm/min, and subjected to the microtensile strength test.
The values were obtained in Newton (N) units, and then converted to mega pascals (MPa) using the following formula: MPa = N/mm2 (surface area).
All samples were kept moist during the preparation and test procedures.
Fracture analysis
Fractured surfaces of the dentin-composite rods in each group were examined under stereomicroscopy (Olimpus SZ 40) at x 220 magnification, and images of the surfaces were acquired.
The types of failure were recorded as adhesive, cohesive or mixed type.
Statistical analysis methods
The SPSS version 18.0 software package was used in the statistical analysis of the data. Nonparametric and Mann-Whitney U-test were performed, since the values obtained in the study did not meet the conditions for performing parametric tests.
Results
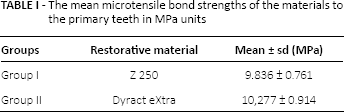
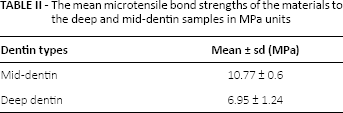
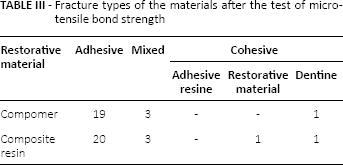
In the evaluation of the microtensile bond strength of the 2 restorative materials used in the onlay restoration of primary teeth with extensive substance loss, the mean microtensile bond strengths of the materials in MPa units are presented in Tables I and II with standard deviations. The analysis of bond strengths using the Mann-Whitney U-test did not show significant difference between the rank averages of the compomer and composite resin (p = 0.741). The dentin sections, from which test samples were obtained, contributed to the bond strength; dentin samples obtained just above the pulp had a lower bond strength, and the difference was statistically significant (p = 0.005). The fracture data of the materials are presented in Table III. The adhesive type fracture was the most prevalent fracture type for both materials.
The mean microtensile bond strengths of the materials to the primary teeth in MPa units
The mean microtensile bond strengths of the materials to the deep and mid-dentin samples in MPa units
Fracture types of the materials after the test of microtensile bond strength
Discussion
It is a striking finding that studies investigating the bond strength of restorative materials used in dentistry mainly focus on permanent teeth, and there are fewer studies conducted on primary teeth (14–17). It is suggested that the success of the materials could be different between primary and permanent teeth when the chemical, physiological, and micromorphological differences between the primary and permanent teeth are taken into consideration (18–21). Therefore, materials used in dentistry must be evaluated separately for primary teeth.
In the test method developed by Sano et al (22), the use of samples with a small surface area (0.25–1 mm2) provides more homogeneous stress distribution. The method also possesses other advantages; for instance, more than 1 sample can be obtained from an individual tooth, the adhesive type fracture is observed mostly, and the method allows regional measurement of the bond strength. Because of these features, microtensile tests are commonly employed (21, 23, 24). In the present study, we used this microtensile test method to evaluate the bond strength between the restoration and the dentin tissue.
When compared to enamel, binding to dentin tissue is more problematic since the dentin tissue has a mixed chemical composition from organic and inorganic substances and it exhibits different characteristics in different layers. Various studies have indicated that strength of binding to different dentin regions and structures may differ in cases where human teeth are used (25–27). In the present study, deep and mid-dentin samples were subjected to the microtensile bond strength test, and samples obtained from the deep dentin section exhibited lower bond strength compared to mid-dentin samples.
Dentin tissue is known to exhibit regional differences in the structure, and the size of the dentin channels vary in enamel-dentin and pulp border (28, 29). The dentin channels measure 2.5 μm in the pulp border, 1.2 μm between the pulp and enamel-dentin border, and 900 nm in the enamel-dentin border (30). During cavity preparation, the flow of dentin lymph from the open channels into the cavity occurs at a higher rate in deep dentin regions. The flow of dentinal fluid may also affect the polymerization of the adhesive resin, and different bond strength values have been reported from the different dentin sections (25). In addition, the closer the binding is to the tooth pulp, the lower the calcium level is and the amount of intertubular dentin where the binding occurs, and this may be the reason for low bond strength values in the deep dentin. This becomes more important in the case of primary teeth.
The mean bond strength of the onlay restorations using the indirect method was 10.277 ± 0.914 MPa for Dyract eXtra compomer restoration and 9.836 ± 0.761 MPa for Filtek Z 250 composite restoration. We were unable to find a study in the literature investigating the microtensile bond strength of the compomer and composite resin polymerized using an indirect method in the restoration of primary teeth.
In the studies where polymerization were performed by a direct method, bond strength to primary teeth for Filtek Z 250 ranges from 7.60 to 32.80 MPa (17, 31–33), and bond strength to primary teeth for Dyract eXtra compomer materials ranges from 8.67 to 18.03 MPa (15, 33, 34). A wide range of bond strength reported for resin materials may be caused by the test technique used and the use of different binding systems. In the present study, mean bond strength values obtained for composite and compomer resin materials fall into this range. Although there is a standardized procedure to follow in microtensile bond strength studies, external factors such as room temperature and moisture can affect the results, along with other factors in the preparation and testing of the samples such as dentin depth, tooth type and storing conditions. Thus, it is quite difficult to compare studies addressing this subject. On the other hand, providing detailed information in studies about the teeth, materials, the preparation of the samples and the procedure prior to testing, data collection and evaluation would facilitate comparing the studies and determining the source of the differences.
Fracture analysis followed by the bond strength test is particularly important to indicate the reliability of the measured bond strengths of the adhesive systems. The common occurrence of cohesive failures precludes accurate measurement of the binding between adhesive system and the dentin (22, 35). Cohesive failures are caused by defective parts in the dentin or restorative material and irregular stress distribution in these defective parts; therefore, adhesive type fractures are desired that accurately reflect bond strength.
In the present study, the failure types related to the restorative material included adhesive (81%), cohesive (6%) and mixed (12%) type. Composite and compomer resin materials exhibited a comparable number of mixed-type fractures. Adhesive resin did not exhibit cohesive failure. Composite resin material exhibited cohesive failure in 1 sample. Cohesive failure was observed in 1 dentin sample in each group. The higher occurrence of adhesive type fractures in the present study suggests that adhesive systems realistically reflect the bond strength.
Conclusions
In the present study evaluation of the microtensile bond strength of the 2 restorative materials used in the onlay restoration of primary teeth using an indirect method is similar for both materials and the samples obtained from the deep dentin section exhibited a lower bond strength compared to mid-dentin samples.
Footnotes
Financial support: This study was supported by the Süleyman Demirel University through the Scientific Research Projects Coordination Unit. Number of project: 1852-D-09.
Conflict of interest: None of the authors has financial interest related to this study to disclose.