
Abstract
Purpose
Removal of cytokines is relevant for dialysis patients as they are suspected to promote cardiovascular complications. The objective of this study was to benchmark membranes with different permeability profiles under standardized in vitro test conditions using miniaturized devices with respect to their ability to remove cytokines from human serum and to lower cell activating potential.
Methods
In vitro dialysis was used to dialyze cytokine enriched serum in 3 independent experiments per tested membrane. IL-6 in the serum and dialysate was measured at defined times by enzyme-linked immunosorbent assay. IL-8, IL-1β, IL-6 and TNF-α in dialysate were measured by immunoassay. Dialysate samples were subjected to cultured tubular epithelial cells or human fibroblasts to study cell activation via IL-6 generation. Dialysate samples were added to human whole blood with subsequent analysis of granulocyte and monocyte activation by detection of CD11b.
Results
IL-6 decreased in serum and increased in dialysate during in vitro dialysis. IL-8, IL-1β, and TNF-α were identified in dialysate. Dialysate added to cell cultures increased IL-6 concentration in culture medium or increased expression of CD11b. High cut-off membranes showed the strongest transfer of cytokines, albumin and total proteins from serum to dialysate and led to strongest cell activation. This effect was lower for medium cutoff membranes and lowest for conventional high-flux membranes.
Conclusions
This study demonstrated an in vitro test by which membranes were benchmarked with respect to cytokine and cell activation removal capacity. Cell activation levels could be influenced by the choice of membrane by altering cytokine concentration levels.
Introduction
Dialysis is a life-saving therapy for end-stage renal disease patients. Nonetheless, the mortality of these patients is higher than that of individuals without kidney failure, particularly due to cardiovascular complications (1). Chronic inflammation is suspected to promote cardiovascular complications (2). A variety of factors may be the root causes of chronic inflammation (3). Among them are the patient's comorbidities, the foreign surface contact of the patient's blood, uremia or contaminated dialysis fluid. A common observation in chronic inflammation is an increased concentration of pro-inflammatory mediators, particularly cytokines such as interleukin-8 (IL-8, Uniprot Entry P10145, 8.4 kD processed chain with 72 amino acids), interleukin-6 (IL-6, Uniprot Entry P05231, 20.8 kD processed chain with 183 amino acids), interleukin 1β (IL-1β, Uniprot Entry P01584, 17.4 kD processed chain with 153 amino acids) or tumor necrosis factor α (TNF-α, Uniprot Entry P01375, 17.4 kD processed chain with 157 amino acids, forming a homotrimeric structure of 52.2 kD) (4, 5).
The removal of cytokines by dialysis could potentially diminish inflammatory processes. Cytokines are among the mid-sized uremic toxins, in the molecular weight range between 8.4 kD of IL-8 and 52.2 kD of trimeric TNF-α. Conventional dialysis membranes have limited permeability to cytokines, with the consequence that cytokines are retained in the patient's blood. There have been many studies with dialysis membranes with larger pore sizes that investigated their effect on cytokine removal (6–8). This has been systematically reviewed (9, 10).
High cut-off (HCO) membranes (11) are widely employed today in acute treatments for efficient removal of free light chain proteins in patients with myeloma kidney (12, 13) and for elimination of cytokines in patients with septic acute kidney injury (14). Short pilot studies with HCO membranes have also been done in patients receiving chronic hemodialysis, targeting molecules associated with chronic inflammation (15, 16). A drawback of HCO membranes is their permeability of albumin which precludes their long-term use in a chronic hemodialysis prescription. Therefore a novel class of high-flux dialysis membranes with extended permeability, referred to as medium cut-off (MCO) membranes, was developed (17). The MCO membranes showed high clearance of mid-sized uremic toxins while retaining albumin that allows regular use for patients on chronic dialysis (18). The objective of this study is to benchmark membranes with different permeability profiles with respect to their cytokine removal capacity and their ability to remove cell activating potential from human serum under standardized in vitro test conditions using miniaturized devices.
Methods
Test items
The test items were mini-dialyzers with a standardized membrane area of 360 cm2 containing hollow-fiber membranes taken from Revaclear 400 (Revaclear) and Cordiax FX80 (Cordiax) conventional high-flux dialyzers; Theranova 400 (Theranova) and MCO-Ci 400 (MCO-Ci) high-flux dialyzers with extended permeability, and an HCO1100 high cutoff dialyzer (Tab. I). Membrane classification was based on dextran-sieving characteristics (11, 17).
Membranes studied
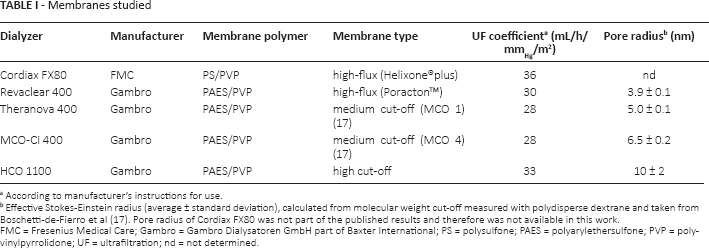
According to manufacturer's instructions for use.
Effective Stokes-Einstein radius (average ± standard deviation), calculated from molecular weight cut-off measured with polydisperse dextrane and taken from Boschetti-de-Fierro et al (17). Pore radius of Cordiax FX80 was not part of the published results and therefore was not available in this work. FMC = Fresenius Medical Care; Gambro = Gambro Dialysatoren GmbH part of Baxter International; PS = polysulfone; PAES = polyarylethersulfone; PVP = polyvinylpyrrolidone; UF = ultrafiltration; nd = not determined.
Blood donations by healthy donors
Whole blood was collected under medical supervision from healthy donors in accordance with ethical guidelines approved by Gambro Dialysatoren GmbH (part of Baxter International Inc.). Informed consent was obtained from all subjects. The principles outlined in the declaration of Helsinki were followed.
Cytokine-enriched serum
Cytokine-enriched serum was prepared from lipopolysaccharide (LPS)-activated human heparinized (30 U/mL) whole blood. Activation was performed for 6 hours at 37°C with 100 EU/mL final activity of LPS from E. coli O55:B5. Plasma was prepared by collecting the supernatant fraction of centrifuged blood. A sample of native plasma was collected before LPS activation. In a second step, cytokine-enriched serum was prepared by diluting the cytokine-enriched plasma 1:10 with human serum (Biomex). The prepared serum was divided into identical fractions and used as uniform test solutions for in vitro dialysis.
In vitro dialysis circuit
Mini-dialyzers were tested in an in vitro dialysis setup with cytokine-enriched serum and bicarbonate-based dialysis fluid. Bicarbonate dialysis fluid was prepared according to the manufacturer's instructions from concentrates D227 and D200 (MTN Neubrandenburg). For in vitro dialysis, 190 mL cytokine-enriched serum was recirculated at 10 mL/min on the blood side, and 190 mL dialysis fluid was recirculated at 25 mL/min on dialysate side in the countercurrent flow direction. No net ultrafiltration was applied, which was controlled by the fluid volume balance. The whole system was maintained at 37°C for 90 minutes, and samples were drawn at a defined time point during the experiment and stored frozen until further analysis. The in vitro dialysis circuit was the central element of the study; the overall design of the study is illustrated in Figure 1.
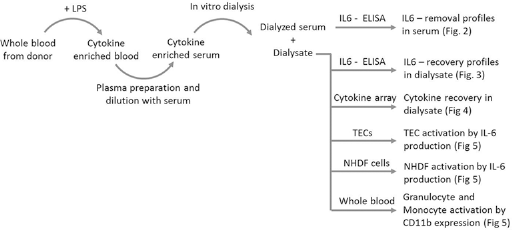
Illustration of the study design.
Cytokine and protein analysis
IL-6 was quantified using the IL-6 CytoSet ELISA kit (Invitrogen) with 96-well plates, analyzed on an Ultra Microplate Reader EL808 (BioTek Instruments). Additionally, the BD cytometric bead array for human inflammatory cytokines (BD Biosciences) was used on a FACSCalibur flow cytometer (BD Biosciences) to determine IL-8, IL-1β, IL-6 and TNF-α. Human serum albumin was quantified by nephelometry on a Siemens BN Prospec Analyzer with BN Prospec System reagent kits (Siemens). Total protein was determined on a cobas Mira™ clinical autoanalyzer (Roche Diagnostics) system with the total protein reagent kit based on the biuret method (Fisher Diagnostics) and protein standards as reference.
Tubular epithelial cell (TEC) cultures
Cells of the HK-2 (ATCC® CRL-2190™) cell line obtained from the human kidney proximal tubule were cultured in Keratynocyte SFM + Supplements EGF and BPE (K-SMF Kit) supplemented with 1% fetal bovine serum (Gibco, Life Technologies, 1.2 mM CaCl2, 4 mM KCI (Merck) and 0.1 mg/mL Meronem (AstraZeneca) in polystyrene cell culture flasks (BD Falcon) in a humidified incubator at 37°C and 5% CO2.
TEC bioassay
For the bioassay, the cells were seeded in 6-well cell-culture inserts (BD Falcon) at a density of approximately 20,000 cells/cm2. The cell culture medium was refreshed every 2-3 days until the cells reached a confluent state. After 7 days, the cell culture medium was exchanged with 5 mL diluted sample or control (2 mL in the insert and 3 mL in the 6-well plate supporting the insert). To sterilize the samples, they were filtered through a 0.2 μm membrane and diluted 1:10 with prewarmed cell culture medium. The cells were incubated for 2 days in a humidified atmosphere at 37°C and 5% CO2. After incubation, the supernatant was collected and stored at −70°C for further analysis. Cells were detached using Accutase (PAA Laboratories), resuspended and used for cell analysis immediately thereafter.
Normal human dermal fibroblast (NHDF) culture
NHDF primary cells (Clonetics CellSystems) obtained from human skin were cultured in DMEM (Lonza) supplemented with 10% fetal bovine serum, 100 U/mL penicillin and 100 μg/mL streptomycin (Gibco, Life Technologies) in polystyrene cell culture flasks (BD Falcon) in a humidified incubator at 37°C and 5% CO2.
NHDF bioassay
For the bioassay, the cells were seeded in 24-well tissue culture plates (BD Falcon) at a density of approximately 6,250 cells/cm2. The cell culture medium was replaced after 1 day with 450 μL fresh medium and 150 μL sample filtered through a 0.2-μm sterile filter. The cells were incubated for 3 days in humidified air at 37°C and 5% CO2. After incubation, the supernatant was collected and stored at −70°C for further analysis. Cells were detached using Accutase (PAA Laboratories), resuspended, and used for cell analysis immediately thereafter.
Cell analysis
Cells were counted with a CASY® TTC cytometer (Schärfe System) containing a dielectric cell analyzer to discriminate among live cells, dead cells and debris.
Whole blood activation with flow cytometric analysis
Human whole blood was collected in sterile containers from healthy donors and anticoagulated with 10 IU/mL sodium heparin (Ratiopharm). Each 100 μL sample was filtered for sterility with a 0.2 μm membrane and gently mixed with 900 μL of whole blood. The blood-containing tubes were incubated with loosened caps for 3.5 hours in a humidified incubator at 37°C and 5% CO2. The incubation was stopped by 10 mM EDTA (Merck).
Cells were stained with monoclonal mouse anti-human CD14 fluorescein isothiocyanate (CD14-FITC)- and monoclonal mouse anti-human CD11b phycoerythrin (CD11-PE)-labeled antibodies (BD Pharmingen™). Immunoglobulin IgG1 and lgG2a FITC- and PE-conjugated antibodies were used as isotype controls. For this purpose, 10 μL of CD14-FITC and CD11b-PE were added to 50 μL of whole blood sample. Isotype controls were used accordingly. Samples were gently vortexed and incubated at 2°C to 8°C for 30 minutes. Next, 1 mL of BD FACS™ Lysing Solution was added to each test tube to lyse erythrocytes. The tubes were vortexed and incubated at room temperature for another 10 minutes in the dark, then centrifuged, and the supernatant was discarded. Cells were washed with 3 mL CellWASH, fixed with CellFIX solution and analyzed within 24 hours in a FACSCalibur™ flow cytometer using the CellQuest™Pro Software (BD Biosciences).
Statistics
For each membrane type, 3 independent runs of in vitro dialysis were performed. If not otherwise stated, numbers are given as mean values ± standard error. Statistical analysis was performed using SigmaPlot (Version 12.5, Systat Software). One-way analysis of variance (ANOVA) was used to detect differences in data sets. Pairwise multiple comparisons were performed using the Holm-Sidak method. The Shapiro-Wilk test was used to verify normality. In cases where the normality of data was not given, ANOVA on ranks with the Student-Newman-Keuls method was applied. Differences between 2 data sets were considered with a significance level of p = 0.05. Pearson correlation was used for correlation analysis with a significance level of p = 0.05 to identify significant relationships between variables.
Results
Sample characterization
Simulated in vitro dialysis treatments were conducted, and samples were collected before the experiment and after 15, 30, 60 and 90 minutes of dialysis from the blood and dialysate sides. IL-6 concentrations were determined. The starting IL-6 concentration in the uniform serum preparation was 8,526 ± 229 pg/mL IL-6 concentrations in the serum plotted versus time of experiment showed a steady decrease of IL-6 in all cases but one (Fig. 2). The treatment with the HCO1100 membrane resulted in the steepest decrease. In the treatments with Cordiax, the IL-6 concentrations remained on the starting level. The treatments with Revaclear resulted in a slight decrease, and Theranova and MCO-Ci showed almost identical degrees of IL-6 decrease with steepness between the results from Revaclear and HCO1100. IL-6 concentrations in the corresponding dialysate samples plotted versus time of experiment showed a steady increase in IL-6 in all cases (Fig. 3). The dialysate samples showed a clear order of concentration increase, which was strongest for treatments with HCO1100 membranes and decreased in the order MCO-Ci, Theranova, Revaclear and Cordiax. The dialysate samples collected after 90 minutes were used to measure the concentrations of IL-8, IL-6, IL-1β and TNF-α as well as human serum albumin and total protein. Measurable concentrations were detected for all these cytokines and proteins (Fig. 4; see Supplementary Table I available online as supplementary material at www.artificial-organs.com). In all cases, the cytokine and protein concentrations were highest after the HCO1100 treatment and decreased in the order MCO-Ci, Theranova, Revaclear and Cordiax.
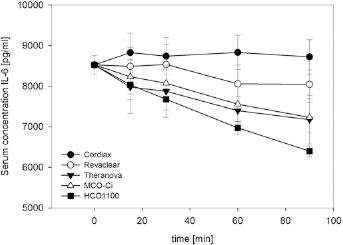
IL-6 serum concentrations displayed as mean value ± standard error of 3 independent experiments versus time.
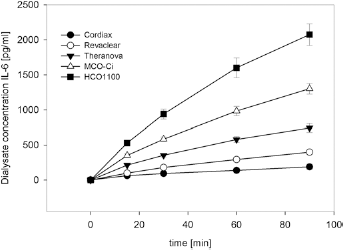
IL-6 dialysate concentrations displayed as mean value ± standard error of 3 independent experiments versus time.
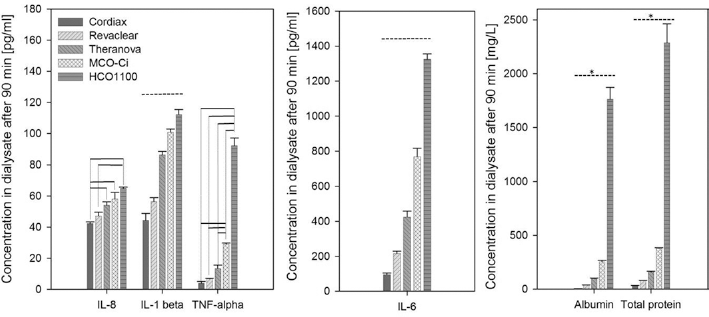
Concentrations of cytokines and proteins in dialysate samples after 90 minutes displayed as mean value ± standard error of 3 independent experiments. Horizontal lines indicate significant differences. Solid horizontal lines reflect individual pairwise differences tested by Holm-Sidak. Dotted horizontal lines represent all pairwise differences tested by Holm-Sidak. Dotted horizontal lines with an asterisk represent all pairwise differences tested by Student-Newman-Keuls method.
Statistical analysis revealed pairwise differences at a significance level of p = 0.05. For the IL-1β, IL-6, human serum albumin and total protein dialysate concentrations, all pairwise comparisons showed a significant difference. For IL-8 and TNF-α significant differences in pairwise comparisons were mainly identified when the open pore membranes HCO1100, MCO-Ci and Theranova were compared against Revaclear or Cordiax.
Bioassays
Dialysate samples collected after 90 minutes of in vitro dialysis were tested in bioassays to investigate the cell activating capacity removed from the serum samples. Untreated dialysis fluid was used as a control for the matrix effect. Diluted native plasma with total protein concentration of 2,551 mg/L was used as a control to rule out unspecific cell stimulation by increased total protein concentration. In the TEC cell and NHDF cell systems, the effect of the samples was consistently higher than the dialysis fluid and the native plasma control sample, which remained at a background level (Fig. 5; see Supplementary Table II available online as supplementary material at www.artificial-organs.com). In the whole blood assay, the samples collected from HCO1100 and MCO-Ci resulted in stronger CD11b activation of granulocytes, and for monocytes, the samples collected from HCO1100, MCO-Ci, Theranova and Revaclear resulted in stronger CD11b activation compared to the dialysis fluid control (Fig. 5).
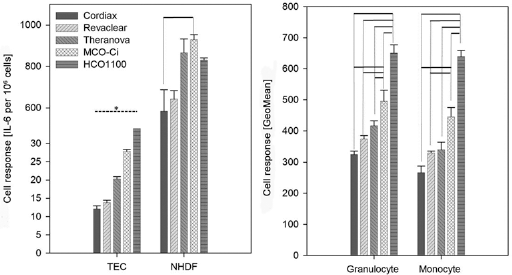
Bioassay cell signals after incubation of cells with dialysate samples after 90 minutes displayed as mean value ± standard error of 3 independent experiments. Horizontal lines indicate significant differences. Solid horizontal lines reflect individual pairwise differences tested by Holm-Sidak. Dotted horizontal line with an asterisk represents all pairwise differences tested by the Student-Newman-Keuls method.
Throughout all bioassays, the cell signals induced by dialysate samples increased in the order Cordiax, Revaclear, Theranova, MCO-Ci and HCO1100, with only 1 exception in the NHDF bioassay system, in which HCO1100 samples did not produce the largest cell activation signal. Pairwise differences were revealed by statistical analysis. In the TEC bioassay system, all pairwise differences were found to be statistically significant, whereas in the NHDF bioassay system, there was only 1 significant difference between MCO-Ci and Cordiax. In the whole blood assay, significant differences were only found for HCO1100 and MCO-Ci when compared to membranes of lower permeability.
Correlations
Correlation analysis was performed using the Pearson method to identify significant relationships between cytokine concentrations in dialysate samples collected after 90 minutes and cell activation levels. Significant relationships with positive correlation coefficients (cc) and p value <0.05 were identified between the TEC response and IL-8 (cc 0.982, p = 0.0028), IL-1β (cc 0.899, p = 0.00748), TNF-α (cc 0.909, p = 0.0325), and IL-6 (cc 0.987, p = 0.00175), between NHDF response and IL-1β (cc 0.899, p = 0.0378), between granulocyte activation and IL-8 (cc 0.963, p = 0.00849), IL-1β (cc 0.914, p = 0.0297), TNF-α (cc 0.967, p = 0.00729), and IL-6 (cc 0.998, p = 0.000129), and between monocyte activation and IL-8 (cc 0.932, p = 0.0213), TNF-α (cc 0.979, p = 0.00366), and IL-6 (cc 0.990, p = 0.00128).
Conclusions
Dialysis membranes were benchmarked based on their cytokine removal capacity and ability to remove substances with cell activating capacity. This property may be relevant to addressing the issue of chronic inflammation in dialysis patients. A standardized testing system was used to allow a true membrane comparison over a broad range of permeability profiles.
Standardization was achieved using an in vitro test system with miniaturized devices. Two major findings emerged from this study. The first is the consistent pattern of cytokine permeability shown by the amount of IL-6 removed from the serum (Fig. 2) and recovered IL-6, IL-8, IL-1β and TNF-α in the dialysate (Figs. 3 and 4). The permeability was always highest for HCO1100 membranes, sequentially followed by MCO-Ci, Theranova, Revaclear and Cordiax. The differences between membranes were most obvious for the middle-molecular-weight range molecules IL-6, at 20.8 kD, and IL-1β at 17.4 kD. MCO-Ci and HCO1100 showed superior removal capacity for the largest cytokine under investigation: TNF-α with 52.2 kD. For IL-8, at 8.4 kD, a similar removal capacity was expected with all tested membranes; however, HCO1100, MCO-Ci and Theranova were found to be superior to Revaclear and Cordiax. However, the promising effect of increased cytokine removal capacity of membranes with increased pore size occurred alongside increased removal of human serum albumin and total proteins. These 2 effects need to be counterbalanced when considering clinical applications.
The second major finding was that the pattern of cytokine permeability was reflected in the cell activation levels found in the bioassays (Fig. 5). This reflection was most obvious for the TEC system, with the highest cell activation capacity found in dialysate samples from HCO1100 membranes, sequentially followed by MCO-Ci, Theranova, Revaclear and Cordiax, and all pairwise comparisons were found to be statistically significant. The identified statistical correlation between cell signals and cytokine concentrations corroborates the commonly found sequential order of membrane efficiency. The NHDF system showed a trend towards differential cell responses following a consistent pattern; however, this finding could not be supported by statistical analysis. In the NHDF system the pattern of cell response could not be resolved as clear as in the TEC system. Additionally, NHDF cells produced much higher levels of IL-6 compared to the TECs. The suggested interpretation of these observations is that NHDF cells responded strongly to activating agents in the collected dialysate samples and were close to the maximum response level where differences in the dose-response behavior could not be clearly resolved anymore. The TECs, however, showed a response on a weaker level where differences in the activating dose still resulted in different cell response levels.
Although the different membranes resulted in different concentrations of human serum albumin and total protein in the collected dialysate samples, this cannot explain the different levels of cell activation, because the native plasma control sample did not result in increased cell activation at all. The granulocyte- and monocyte-based whole blood assays also followed the same trend as the TEC system; however, this finding could only be partially supported by statistical analysis.
The high CD11b levels in the dialysis fluid control samples were surprising. The absence of proteins in the control sample and a dilution-based effect on leukocyte activation could be a potential explanation.
These findings are highly consistent with published research on membranes with increased permeability and their potential to remove inflammatory capacity. Uchino et al demonstrated increased cytokine removal by membranes with increased permeability, which were called super high flux, when used in hemofiltration mode (7) or in hemodialysis mode (6, 8). Fiedler et al showed increased reduction of proinflammatory cytokines by HCO1100 when compared to conventional high-flux membranes; even though this study failed to demonstrate the hypothesized reduction of monocyte activation (15). In the other study, Girndt et al confirmed increased reduction of proinflammatory cytokines and demonstrated the dampening of leukocyte activation by HCO1100 treatments (16). Similarly, the study by Girndt, Zickler et al showed a reduction in procalcific activity when patients were treated with HCO1100 and cytokine levels were lowered (19).
While the reported studies above used real dialyzers in clinical in vivo settings, this study used miniaturized devices, which allowed a high degree of standardization and comparability while neglecting effects of dialyzer geometry. In this study a low sample number of 3 independent experiments was chosen. This allowed the amount of human serum used as test fluid to be kept low while at the same time making it possible to demonstrate the differences in the benchmarked membranes with sufficient evidence.
Another limitation can be seen in the application of cytokine-enriched serum produced by the LPS stimulation of whole blood. This approach was chosen to represent the serum of chronically inflamed dialysis patients under standardized conditions; however, it does not represent the full uremic milieu of a dialysis patient. The serum IL-6 level in this study was 8,526.6 ± 229.2 pg/mL at the beginning of in vitro dialysis while uremic concentrations are in the range of 8.6 ± standard deviation of 3.7 pg/mL (20). This is a difference of 3 orders of magnitude; however, the relative removal properties should not be impacted by the different baseline concentration levels. This assumption is also supported by the fact that the findings of this study are in consistent agreement with findings in clinical studies mentioned above. Although human serum albumin and total protein concentrations in dialysate samples were reported in this study, this does not allow a prediction of albumin loss in a real clinical treatment but can only be interpreted within the experimental setup of this in vitro study.
In conclusion, this study demonstrated an in vitro test system by which membranes can be benchmarked with respect to their cytokine and cell activation removal capacity, and the findings support the hypothesis that cell activation levels can be influenced by the choice of membrane by altering cytokine concentration levels. As dialyzers with extended permeability become available to nephrologists, more laboratory investigations are needed to characterize the new membranes and eventually clinical studies must determine whether the dialyzer-driven removal of cytokines will result in lower inflammatory tissue responses and benefits for the patients.
Footnotes
Acknowledgments
The authors thank the team Members of MTO and MD (Baxter International Inc.) for providing the testing materials.
Conflict of interest: All authors are employees of Baxter International Inc.
Meeting presentations: The content of the manuscript was presented as a poster abstract and poster at the Meeting of the American Society of Nephrology, held in Chicago from November 15-20, 2016.