
Abstract
The fast-paced growth of Onco-Nephrology reflects the unique connection that exists for kidney disease and cancer in clinical medicine. This area of sub-specialization combines the knowledge and skills of a number of specialty groups that span all corners of medicine. Nephrologists, oncologists, urologists, intensivists, pharmacologists, and palliative care specialists are all important players in this arena. In this issue of the Journal of Onco-Nephrology, a series of papers addressing the various forms of kidney disease that develop in patients with cancer is presented as part of the Onco-Nephrology Highlights section. These papers are based on the Onco-Nephrology Symposium that took place at the MD Anderson Cancer Center in Houston, Texas, USA. I hope you find these 4 papers educational and practical in your provision of care to patients with cancer and kidney disease.
On October 14, 2016 in Houston, Texas, the 1st Annual MD Anderson Cancer Center Onco-Nephrology Symposium took place. The symposium chairs, Drs. Sheldon Chen and Farhad Danesh, with the organizing committee, put together an excellent program with expert faculty. This timely conference demonstrated the importance of this rapidly growing field, which has been dubbed Onco-Nephrology. This area of sub-specialization combines the unique knowledge and efforts of a number of specialty groups, including nephrologists, oncologists, urologists, pharmacologists, intensive care specialists, and palliative care specialists (1).
As healthcare providers practicing in this clinical arena, we must evolve high-level competence in caring for cancer patients who develop kidney disease. To accomplish this feat, we must expand our understanding of the pathophysiology of kidney disease that occurs in patients with cancer. Also, clinicians must gain the appropriate knowledge and clinical skills that will allow a competent approach to the diagnosis and management of the particular type of kidney injury that develops in cancer patients (2). Acquiring these clinical skills will allow us to handle the overwhelming majority of kidney diseases that develop in cancer patients (3).
While the entire series of Onco-Nephrology Symposium lectures were outstanding and highly educational, 4 presentations were ultimately chosen to represent the diversity of topics covered by the expert faculty. Cancer-related hyponatremia, kidney lesions associated with multiple myeloma, cancer-related chronic kidney disease (CKD), and erythropoietic-stimulating agent (ESA) use in anemic cancer patients with CKD were chosen for the Onco-Nephrology Highlights in this issue of the Journal of Onco-Nephrology.
The first article in this issue focuses on a common electrolyte abnormality associated with cancer—hyponatremia. Drs. Palmer and Clegg eloquently discuss the epidemiology, pathophysiology, causes, clinical approach to and management of cancer-associated hyponatremia (Tab. I) The authors recommend a thoughtful, clinical approach to hyponatremia that allows classification in various categories. The various causes of hyponatremia in patients with cancer, including the syndrome of inappropriate antidiuretic hormone secretion (SIADH), endocrinopathies, edematous disorders, drugs, and pneumonia, are discussed (Tab. I). Included in the discussion is the mechanism and management of cancer-associated hyponatremia. Importantly, the authors cover both acute and chronic hyponatremia therapy as well as handling hyponatremia overcorrection.
Hyponatremia associated with cancer
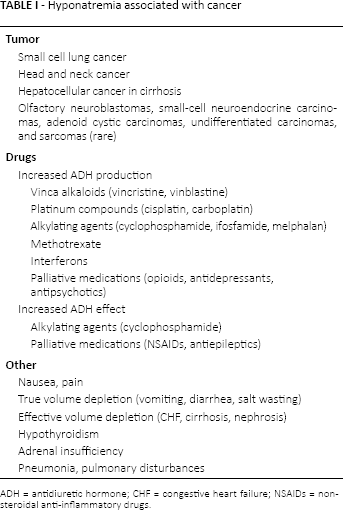
ADH = antidiuretic hormone; CHF = congestive heart failure; NSAIDs = nonsteroidal anti-inflammatory drugs.
The next important subject discussed in this compendium of articles is the many adverse renal effects of multiple myeloma. In his lecture entitled “Multiple myeloma and the kidney,” Dr. Amit Lahoti and colleagues review the various kidney lesions that occur in the setting of myeloma. He begins with a brief introduction of myeloma and kidney disease and follows with a description of the pathogenesis of kidney lesions – noting that inherent properties of immunoglobulins and light chains promote kidney injury. As noted in Table II, there are a number of kidney lesions involving the glomerulus, tubulointerstitium, and vasculature that ultimately cause acute and chronic kidney injury, proteinuria, and metabolic disturbances. Figure 1 demonstrates the most common kidney lesion seen with myeloma-cast nephropathy. Dr. Lahoti also provides insight into the pathophysiology underlying these kidney lesions, associated clinical findings, and the appropriate therapy for these myeloma-related kidney diseases. In the case of the latter, he briefly reviews important and effective antimyeloma medications and the current role of extracorporeal therapies (plasmapheresis and high cut-off hemodialysis).
Kidney lesions associated with multiple myeloma
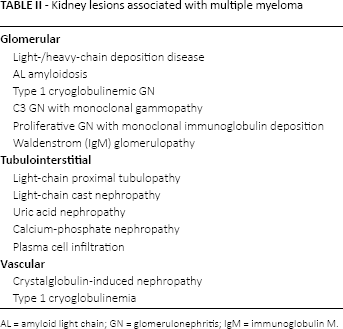
AL = amyloid light chain; GN = glomerulonephritis; IgM = immunoglobulin M.
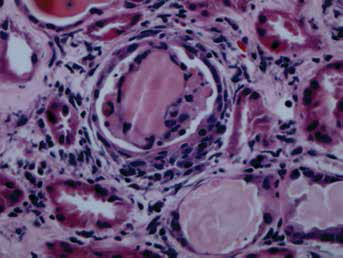
Cast nephropathy in a patient with multiple myeloma and acute kidney injury. Note the cellular reaction around the fractured cast containing myeloma paraprotein.
As noted by the lecture title, “CKD as a complication of cancer,” Drs. Selamet and Abudayyeh describe the bi-directional connection between CKD and cancer. The paper introduces this connection, and describes CKD prevalence in cancer for the readers. The various causes of CKD in patients with cancer follows, with a focus on the various anticancer agents that lead to nephrotoxicity, including AKI, CKD, and electrolyte/acid-base disorders. The risk for cancer development in patients with CKD, in particular dialysis patients and organ transplant patients, is discussed. Finally, the increased cancer mortality observed in CKD patients is reviewed for the readers.
As noted by the title, “ESA use in CKD and cancer” is an enigma that most nephrologists struggle with when caring for their anemic cancer patients with underlying CKD. Dr. Steven Fishbane and colleagues review the available data underlying this complicated issue. As clinicians caring for these patients, we have to contend with balancing the ravages of uncorrected symptomatic anemia with the potential risk of death, thromboembolic disease, and cancer progression when an ESA is employed. The paper by Fishbane and colleagues note that data concerning the risk of cancer progression associated with ESA therapy is likely overstated by guidelines and expert opinion; however, this association is still inconclusive. Until we have more information, it is reasonable to cautiously approach ESA therapy in CKD patients with active cancer or a previous history of cancer. Addressing reversible causes of anemia, such as iron supplementation in those who are iron deficient, and eradication of infection, will likely improve anemia. Some patients may require transfusion with packed red blood cells to manage symptomatic anemia while avoiding ESA exposure. A potential approach is suggested in Figure 2, which demonstrates an algorithm for the use of ESAs in patients with cancer and kidney disease that are suffering from anemia.
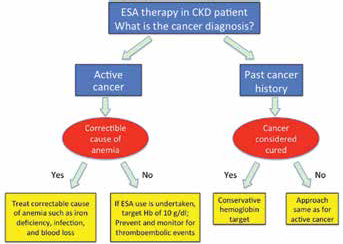
Approach to ESA use in the treatment of anemia in CKD patients with cancer. The flow diagram shows 3 different pathways of ESA therapy for CKD patients depending on their cancer history (active cancer and past history of cancer). CKD = chronic kidney disease; ESA = erythropoietic stimulating agent.
I hope the journal readers find this series of papers from lectures delivered at the 1st Annual MD Anderson Cancer Center Onco-Nephrology Symposium educational and of practical value. This will improve the provision of care for commonly encountered onco-nephrology problems similar to those discussed in this Onco-Nephrology Highlights.
Footnotes
Financial support: None.
Conflict of interest: None.