
Abstract
Emerging data suggest tantalizing links between cancer and systemic inflammatory rheumatic syndromes. In scleroderma, patients may have an increased risk of cancer, secondary to chronic inflammation and damage from the disease, malignant transformation promoted by immunosuppressive therapies, a shared susceptibility to both cancer and autoimmunity, or a common inciting exposure. However, it is increasingly recognized that a subset of patients develop cancer around the time that scleroderma clinically manifests, raising the question of cancer-induced autoimmunity. In this review, we discuss data suggesting a mechanistic link between cancer and the development of scleroderma, and the clinical implications of these findings.
Introduction
As in many of the systemic inflammatory rheumatic diseases, patients with scleroderma have an increased risk of cancer compared to the general population. This risk increase may reflect a number of mechanisms including chronic inflammation and damage from scleroderma or its immunosuppressive therapies leading to malignant transformation. In many instances, cancer diagnosis shortly precedes the development of scleroderma, suggesting that cancer therapies or malignancy itself may promote the development of the autoimmune disease. Emerging data demonstrate that a subset of patients identified by distinct autoantibodies likely have cancer-induced autoimmunity. In this review, we explore these potential links between cancer and scleroderma, discuss new data supporting a paraneoplastic model of scleroderma pathogenesis, and suggest future directions for research.
Evaluation of cancer risk and potential risk factors for cancer in scleroderma
Most epidemiologic studies have demonstrated an elevated age- and sex-adjusted risk of cancer in patients with scleroderma compared to the general population (1–2–3–4–5–6–7–8–9–10–11–12–13–14), similar to that observed across the spectrum of the autoimmune rheumatic diseases (15–16–17–18–19). Data from observational cohorts, national databases, and meta-analyses have suggested that the extent of this risk may vary from a 1.2- to a 4.2-fold increased risk of cancer, with one US study not identifying an increased risk (20). While it is beyond the scope of this article to comprehensively review all articles on cancer risk in scleroderma, a representation of these epidemiologic studies is shown in Table I.
Risk of cancer in scleroderma from cohort studies, national registries, and systematic reviews and meta-analyses
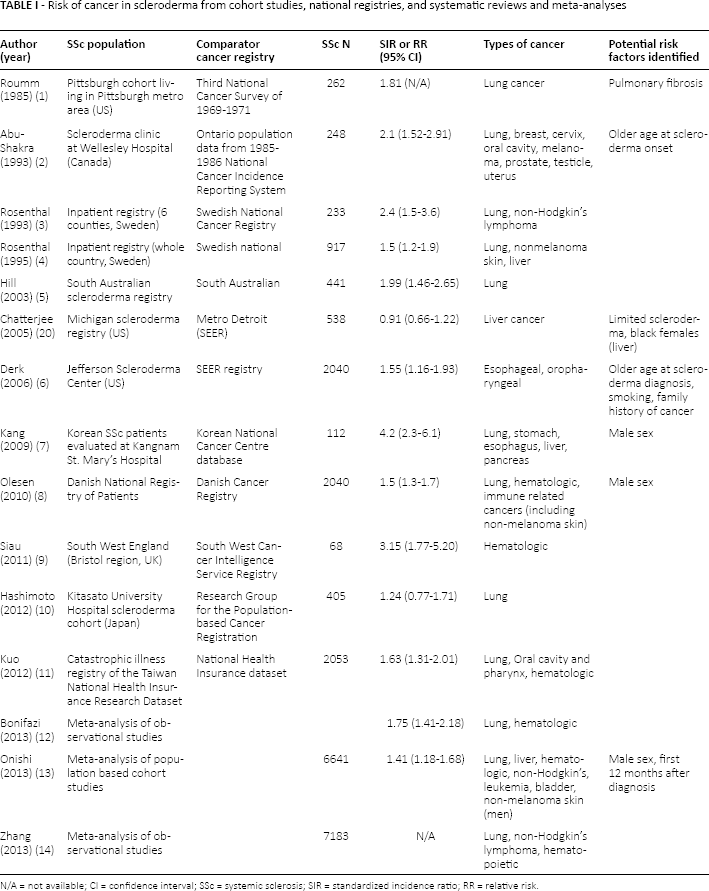
N/A = not available; CI = confidence interval; SSc = systemic sclerosis; SIR = standardized incidence ratio; RR = relative risk.
As with other systemic rheumatic diseases, an increased risk of many tumor types has been appreciated in scleroderma, including lung, bladder, hematologic, melanoma, non-melanoma skin, liver, esophageal, tongue/oropharyngeal, and thyroid cancers (11, 21–22–23–24–25). To date, there has not been conclusive evidence of an increased risk of other sex-specific cancers such as breast, cervical, ovarian, uterine, prostate or testicular malignancies. While most studies have not detected an increased risk of breast cancer in scleroderma compared to the general population, a close temporal relationship between breast cancer and scleroderma onset has been frequently noted, raising the question of whether there is a mechanistic link between these conditions (1, 26–27–28–29).
Of great interest is whether there are demographic or scleroderma phenotypic characteristics that associate with an increased cancer risk in scleroderma, as these features may aid in risk stratification to identify patients who would benefit from targeted cancer screening. Some studies suggest that diffuse scleroderma (5), an older age at scleroderma onset (2, 30), male sex (7, 8, 13), and smoking (25) may be factors that associate with a higher risk of cancer, yet these findings have not been consistently replicated. In addition, target organ disease activity and damage, such as Barrett's esophagus from severe reflux, interstitial lung disease (ILD), overlap with primary biliary cirrhosis, or autoimmune thyroiditis, may increase the risk of cancers within those end organs (1, 2, 22, 31). While the data are strongest for an association between ILD and lung cancer risk (2, 7, 24), particularly among patients with anti-topoisomerase 1 autoantibodies, other studies have not confirmed this association (13, 25). Further research and multicenter collaboration is needed to better investigate potential risk factors for cancer in scleroderma in robust sample sizes.
Potential mechanisms linking cancer and scleroderma
The relationship between cancer and the autoimmune rheumatic diseases is likely complex and bidirectional (32). Cancers may precede or follow the diagnosis of a rheumatic disease, raising intriguing questions about the link between cancer and autoimmunity.
Cytotoxic, radiation and immuno-therapies for cancer may increase the risk of developing scleroderma. For example, patients treated with bleomycin, gemcitabine, paclitaxel and carboplatin for cancer have been reported to develop fibrosing syndromes that are similar to scleroderma or severe vasospastic phenomena and critical digital ischemia (33–34–35–36–37–38). Cutaneous and pulmonary fibrosis may be a late complication of radiation therapy, and case reports have described the development of de novo localized scleroderma after treatment for cancer (39–40–41). Whether scleroderma could be triggered by radiation exposure remains unknown and poorly studied. Lastly, the use of immunotherapies to treat a wide array of tumor types at earlier stages of disease is rapidly expanding (42), raising the question of whether these agents could trigger scleroderma or scleroderma-like disease. Immune checkpoint inhibitors (ICIs), which block negative costimulatory receptors or ligands on T cells and antigen-presenting cells, may result in nonspecific T cell activation. ICIs have been associated with the development of rheumatic immune-related adverse events (irAEs), including inflammatory arthritis reminiscent of rheumatoid arthritis, reactive arthritis, lupus nephritis, sicca syndrome, myositis, and vasculitis (42–43–44).
Conversely, cytotoxic therapies used to treat scleroderma are thought to increase the risk of subsequent cancer. Cyclophosphamide, an alkylating agent commonly used to treat severe cutaneous and pulmonary disease in scleroderma, is associated with an increased risk of hematologic and bladder cancers, particularly in smokers (45–46–47). The data regarding cancer risk with another commonly used drug, mycophenolate mofetil, are less clear. The most experience with this agent is from the transplantation literature where data conflict as to whether there is an increased risk of lymphoma and non-melanoma skin cancer (48–49–50–51). Recent data also suggest that primary CNS lymphoma risk is increased in post-transplant patients who are treated with mycophenolate mofetil (52). It is important to note that it is difficult to interpret the data from the transplantation literature as these patients are often on combination immunosuppressive therapies. Few reports are available on cancer risk with these agents in scleroderma specifically (53), but in our cohort, these and other immunosuppressive therapies commonly used to treat scleroderma were not associated with risk of cancer (30). However, it is possible that these agents may inhibit the ability to clear oncogenic viral infections and promote malignant transformation, as has been hypothesized in systemic lupus erythematosus (32, 54). Another aspect of scleroderma management that may contribute to cancer risk is cumulative exposure to ionizing radiation from medical tests, such as high-resolution chest computed tomography (CT) screening in scleroderma (55). In this regard, efforts to develop imaging protocols that have high sensitivity and diagnostic accuracy while reducing radiation exposure are critical to mitigating this risk (56).
As described above, chronic inflammation and damage from scleroderma may increase the risk of subsequent malignancy. Other theoretical links between cancer and scleroderma include a shared genetic susceptibility to develop both diseases, or a common inciting exposure.
Case reports and case series describing a close temporal relationship between cancer and scleroderma onset have long raised the question of whether scleroderma may be a paraneoplastic disease in some patients. This has been observed across a wide range of tumor types but has been most notable with breast cancer (1, 26–27–28–29), where in one series, 61% of patients developed breast cancer and scleroderma within 12 months of each other. The description that scleroderma dramatically improves with treatment of the underlying cancer in some cases is intriguing also (57–58–59). These reports suggest that careful study of patients with a clustering of cancer and scleroderma may provide insight into the mechanisms linking the two diseases.
Insights from studies of the temporal relationship between cancer and scleroderma: the example of anti-RNA polymerase III antibodies
In an initial study of 23 scleroderma patients with cancer, we examined the temporal relationship between cancer and scleroderma to define whether any unique clinical features or autoantibody responses associated with a short cancer-scleroderma interval (60). Patients with RNA polymerase III autoantibodies had a significantly shorter cancer-scleroderma interval (median −1.2 years, range −2 to +1.3 years) than patients with anti-centromere (median +11.1 years, range −2 to +36.9 years) or anti-topoisomerase 1 (median +13.4 years, range +0.25 to +29 years) antibodies (p = 0.027). In addition, these patients had increased nucleolar expression of RNA polymerase III in their cancers, which was not evident in cancers from scleroderma patients with other autoantibody responses or in normal control tissues. These data suggested that scleroderma-specific autoantibody production may be a manifestation of an immune response to tumor antigens in a subset of scleroderma patients.
This initial observation has now been validated in several international scleroderma cohorts. Airo, and colleagues (61) examined the prevalence of cancer and the frequency of synchronous cancers in patients with RNA polymerase III autoantibodies compared to other autoantibody subgroups in an Italian cohort of 360 scleroderma patients (n = 16 with RNA polymerase III antibodies, 4.4%). Patients with RNA polymerase III autoantibodies had both a higher prevalence of cancer (43.8% vs. 10.9% of anti-topo and 8.6% of anti-centromere, p<0.001) and were more likely to have cancer coincident with scleroderma onset (18.8% vs. 0% in anti-topo and 0.4% in anti-centromere, p<0.001). Another confirmatory study was performed on an Australian cohort of 451 scleroderma patients, 69 of whom (15.3%) had RNA polymerase III autoantibodies. Compared to patients lacking this specificity, those with anti-RNA polymerase III antibodies had the same prevalence of cancer (13%) but a 4.2-fold increased risk of cancer (95% confidence interval [CI] 1.3-13.4) within 5 years of scleroderma onset (62). In a third confirmatory study, performed on a UK scleroderma cohort (n = 2177), patients with RNA polymerase III antibodies had a 5.8-fold increased risk of cancer (95% CI 3.1-10.9) within 3 years of scleroderma onset compared to patients lacking these antibodies (63). In particular, the risk of breast cancer within 3 years of scleroderma onset was noted to be 19-fold higher among patients with anti-RNA polymerase III antibodies compared to those with anti-centromere antibodies. Similar to the Italian cohort, but in contrast to the Australian data, the prevalence of cancer was also higher among patients with RNA polymerase III autoantibodies compared to those without these antibodies (14.2% vs. 6.3% in anti-topoisomerase 1 group and 6.8% in anti-centromere group; p<0.001). Recent findings from a study performed on a Japanese scleroderma cohort (n = 261), showed that patients with RNA polymerase III autoantibodies were more likely to have cancer (31.8% vs. 2.4% in anti-topoisomerase 1 (p<0.0005) and 5.8% in the anti-centromere group (p<0.005)) (64). The frequency of malignancies diagnosed up to 6 months before to 12 months after scleroderma onset was also higher in patients with RNA polymerase III autoantibodies (13.6% vs. 0% in anti-topoisomerase 1 [p<0.01] and 0.7% in anti-centromere [p<0.01]). Lastly, this relationship was validated in the EUSTAR cohort (65); the authors examined 158 anti-RNA polymerase III-positive patients compared with 199 anti-RNA polymerase III-negative controls, matched on age at scleroderma onset, sex, cutaneous subtype, and disease duration. Malignancies were more commonly diagnosed in patients who were positive for anti-RNA polymerase III antibodies (17.7% vs. 9.0%, p = 0.015). Within 2 years of scleroderma onset, 9% of anti-RNA polymerase III-positive patients had cancer compared to 2.5% of patients without this specificity (p = 0.007). The authors also performed an analysis restricted to patients with anti-RNA polymerase III antibodies; patients with a synchronous cancer were older at scleroderma onset, more often male, and more likely to have diffuse cutaneous disease than patients without a synchronous cancer.
Recently, we validated our initial findings (made on a cohort of 23 well-defined scleroderma patients with an associated malignancy) on a much larger cohort of 1044 scleroderma patients. In this follow-up study, we demonstrated a >5-fold increased risk of cancer within 2 years of scleroderma onset in patients with RNA polymerase III antibodies compared to those negative for these antibodies (OR 5.08, 95% CI 1.6-16.1) (30). Interestingly, patients lacking antibodies against centromere, topoisomerase 1, and RNA polymerase III (hereafter referred to as “CTP-negative”) antibodies also had a shortened cancer-scleroderma interval as they developed scleroderma at older ages. This subgroup is likely comprised of multiple autoantibody specificities, some of which may also associate with a close cancer-scleroderma relationship (see below).
Anti-RNA polymerase III antibodies are likely a marker of malignancy only in patients with scleroderma. In a pilot study of 50 breast cancer patients and 50 at-risk controls, all without rheumatic diseases, anti-RNA polymerase III antibodies were not identified in cases or controls (66). These data suggest that these autoantibodies are unlikely to improve risk stratification for breast cancer in the general population.
Mechanistic studies in patients with anti-RNA polymerase III autoantibodies suggest a model of cancer-induced autoimmunity
The co-occurrence of cancer and scleroderma in patients with anti-RNA polymerase III antibodies raised the intriguing possibility that genetic alterations in the POLR3A locus in tumors may initiate autoimmunity (67). This was addressed in a seminal study using tumors from 16 scleroderma patients, 8 of whom had antibodies against RNA polymerase III, and 8 of whom were either anti-centromere or anti-topoisomerase 1 antibody positive. Data from this study showed alterations in the POLR3A gene locus (somatic mutation and/or loss of heterozygosity) in 75% of cancers from patients with RNA polymerase III antibodies, but not in tumors from the other 8 patients.
Two different kinds of genetic mutations were noted. Three patients had somatic mutations in the POLR3A gene. Interestingly, these mutations changed a single amino acid in each case, with the changed amino acid being different in all 3 patients. Since POLR3A mutations are rare in cancer, it is possible that the anti-RNA polymerase III immune response may be initiated by such somatic mutations. Consistent with this, mutation-specific T cell immune responses were detected in two of the patients with somatic mutations in POLR3A. Loss of heterozygosity (LOH) was the second type of genetic mutation noted in the Joseph et al (67) study, with 62.5% of patients having LOH at the POLR3A gene locus. Since this loss of heterozygosity was not detected in scleroderma patients with anti-topoisomerase or anti-centromere antibodies, it is likely that the anti-RNA polymerase III antibody response is a participant in shaping the molecular evolution of the cancer.
There are several noteworthy aspects to these findings. It is important to recognize that the majority (>80%) of patients with scleroderma and antibodies against RNA polymerase III never have clinically detectable cancers. A possible explanation is that potent anti-tumor immune responses eliminate underlying cancers in most patients with scleroderma and anti-RNA polymerase III antibodies. A second interesting feature is that autoantibodies in the patients with mutated RNA polymerase III cross-react with the wild-type protein (67). This is evidence that the anti-RNA polymerase III immune response may be initiated against the mutated protein in the cancer, then subsequently spread to the wild-type protein present in self tissue. This cross-reactive immune response may result in autoimmunity if there is shared autoantigen expression in scleroderma target tissues. While this remains unknown in scleroderma, data from myositis suggest this possibility (68). In this study, the dermatomyositis-specific autoantigen Mi2 was highly expressed in adenocarcinomas commonly seen in dermatomyositis, and in regenerating myoblasts from myositis muscle. Such findings suggest that enhanced autoantigen expression in target tissues may serve as a feed forward loop that sustains the autoimmune response in these diseases.
Study of CTP-negative scleroderma patients identifies another autoantibody subset with cancer-associated scleroderma: anti-RNPC3 (U11/12)
Based on our prior findings showing that patients in the CTP-negative subset also have an increased risk of cancer around the time of scleroderma onset, we sought to identify novel autoantibodies within this subgroup. In our initial approach, we studied 16 CTP-negative scleroderma patients with a known short cancer-scleroderma interval and utilized Phage Immunoprecipitation Sequencing (PhIP-Seq) for autoantibody discovery (69). This high throughput epitope identification method identified autoantibodies against RNA Binding Region Containing 3 (RNPC3), a 65 kDa component of the minor spliceosome complex, in 4/16 (25%) of this patient subset. In this study, a comparator group of 32 scleroderma sera with anti-RNA polymerase III antibodies was included (with and without cancer); anti-RNPC3 antibodies were not detected in the comparator group (0/32). An immunoprecipitation based assay was used to confirm these PhIP-Seq findings.
As we had selected our initial study population based on a short cancer-scleroderma interval, we sought to validate these findings in our larger cohort of scleroderma patients with cancer (70). Among 318 scleroderma patients with cancer, 12 patients (3.8% of overall cohort or 12.2% of CTP-negatives) were positive for anti-RNPC3 autoantibodies. Relative to patients with anti-centromere antibodies, patients with RNA polymerase III autoantibodies and anti-RNPC3 autoantibodies had a >4-fold increased risk (odds ratio [OR] 4.3, 95% CI 1.1-16.9) of cancer within 2 years of scleroderma onset. Fifty percent of the cancers observed in this group were breast cancers, suggesting that mammography may be important in this patient population. Anti-RNPC3 autoantibodies were not identified in other rheumatic diseases or cancer patients without rheumatic disease, indicating that these autoantibodies are specific to scleroderma and not biomarkers of cancer more broadly. Further work is necessary to define whether genetic or post-translational alterations of RNPC3 are present in cancer tissues from these patients, as was observed for patients with anti-RNA polymerase III antibodies and cancer.
Implications for cancer screening and scleroderma therapeutics
The data in scleroderma suggest that unique subsets of patients may benefit from enhanced cancer surveillance at disease onset. We have previously proposed an approach to cancer screening in scleroderma that includes comprehensive physical examination and age- and sex-appropriate testing such as testicular and digital rectal examination, mammography, Pap smear, and colonoscopy (71, 72).
Further testing should be considered, tailored to each individual's unique risk factors (Tab. II). Lastly, patients with anti-RNA polymerase III antibodies and perhaps those with anti-RNPC3 antibodies, those who are older when they develop scleroderma, or patients with aggressive or atypical features may require additional testing such as CT of the chest, abdomen and pelvis or whole-body PET-CT.
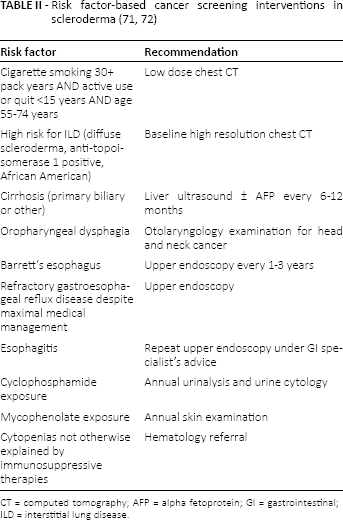
CT = computed tomography; AFP = alpha fetoprotein; GI = gastrointestinal; ILD = interstitial lung disease.
The EUSTAR group has also generated recommendations for cancer screening in patients with anti-RNA polymerase III antibodies by conducting a web-based Delphi exercise including 82 EUSTAR center experts (65). Suggestions include screening for synchronous malignancies, particularly breast cancer in women and screening for other malignancies based on age and sex. A period of 2-5 years of tight cancer surveillance was recommended.
It is important to note, however, that all of the above recommendations are based on expert opinion, rather than a robust evidence base. Prospective studies are needed to identify the optimal approach to cancer screening in patients with new-onset scleroderma that maximizes detection while minimizing harm and costs from over-screening (32).
In aggregate, the data suggesting a model of cancer-induced autoimmunity raise the question of whether early cancer diagnosis and therapy could induce remission of scleroderma. A recent case of a patient with anti-PM/Scl-positive diffuse scleroderma and myositis with a coincident pancreatic neoplasm, supports this possibility (57). This patient had evidence of increased nuclear expression of the 100 kDa component of the PM/Scl complex in her cancerous tissue compared to normal pancreatic tissue. She was rapidly weaned off her immunosuppressive therapy after resection of her cancer, with improved cutaneous and muscle disease. Such striking cases demonstrate the need to prospectively study the effects of cancer therapy on scleroderma outcomes.
Summary
Recent data suggest that unique patient subsets identified by distinct autoantibodies may have paraneoplastic disease. While the cancer-scleroderma interface is most prominent in patients with anti-RNA polymerase III autoantibodies, these cancer-immune interactions likely extend to patients with other scleroderma autoantibodies such as anti-RNPC3. Further investigation to define the relevant autoantigens that associate with cancer-induced autoimmunity will lay a critical foundation to define the population of patients who may benefit from targeted malignancy screening. Early identification and treatment of cancer in patients with new-onset scleroderma may hold the potential to improve scleroderma outcomes.
Footnotes
Financial support: This work was funded in part by the National Institutes of Health (K23 AR061439), the Scleroderma Research Foundation, the Donald B. and Dorothy L. Stabler Foundation, and the Jerome L. Greene Foundation.
Conflict of interest: None of the authors has financial interest related to this study to disclose.