
Abstract
Purpose
To compare complication rates in patients who have port-a-catheters inserted and left accessed for immediate use and those who have ports inserted but not accessed.
Methods
In this retrospective, IRB-approved study, medical records of patients who received a port catheter between 9/2009 and 2/2010 were reviewed. The data collected included patient demographics, diagnosis, procedure and complications. The patients were categorized into two groups: accessed (patients in whom the port was accessed with a Huber needle for immediate intravenous use and the patient left the procedure area with needle indwelling) and control (patients in whom the ports were not accessed). Complications were classified according to Society of Interventional Radiology guidelines. Results are given as mean ±SD. Statistical analysis was performed with student t test and statistical significance was considered at P<.05.
Results
A total of 467 ports were placed in 465 patients (Men: 206); 10.7% in the accessed group (n=50, age: 60±13.9) and 89.3% in the control group (n=417, age: 59±13.5). There were no statistically significant differences in patient demographics between the groups. The overall complication rate was 0.6% (n=3). Two complications (hematoma causing skin necrosis and thrombosis of the port) occurred in the control group and one (infection) in the accessed group. Infection rates after procedures were 2% (1/50) in the accessed group and 0% (0/417) in the control group. There was no statistically significant difference in overall complication (P=.1) and infection (P=.1) rates among the groups.
Conclusions
Leaving the port accessed immediately after placement does not increase the risk of infection or other complications.
Keywords
Introduction
Percutaneously placed port catheters provide an effective way of primary venous access for administering intravenous chemotherapy, long-term medications and fluids (1).
Infection related to the central venous catheter, which may be peri-procedural or may be related to subsequent catheter access, can have a significant impact in the delivery of healthcare to patients. Infection can lead to the removal of the venous access catheter often requiring long-term IV antibiotics and eventually the placement of a new catheter. Port-catheters, which are embedded within the subcutaneous tissue, are often connected to a central vein via a subcutaneously tunneled catheter. Infection of a port can be devastating to the patient as it can lead to its removal and the inability to close the incision site to allow wound healing by secondary-intention.
Although implantable venous access ports are associated with low rates of infection when compared to other types of catheters such as dialysis catheters or peripherally inserted central venous catheters (2), there is a need for constant surveillance for catheter-related infection as detailed by the guidelines provided by the Standards of Practice committee of the Society of Interventional Radiology
(SIR) (3) and U.S. Center for Disease Control and Prevention (CDC) (4).
Central line-associated bloodstream infections are still a major issue in U.S. hospitals, with an estimated occurrence of 41 000 cases each year, resulting in prolongation of hospital stay, increased cost and associated mortality risks (4). Given the cost and morbidity associated with central-line associated bloodstream infections, these complications are monitored monthly in our institution, in compliance with the policies endorsed by the Joint Commission and Center for Medicare and Medicaid (5, 6).
Cancer patients may require utilization of port catheters immediately after their insertion for several reasons including: need for urgent chemotherapy, convenience and to reduce clinical visits to the hospital. Accessing the port immediately after implantation may contribute to the risk of infection and hematoma. There is little data on complication rates when ports are accessed for immediate use during peri-procedural time. Thus, the purpose of this study is to compare the incidence of complications in patients who have ports inserted and left accessed in the interventional radiology suite for immediate use and those who have a port inserted but not immediately accessed.
Materials and Methods
Patient selection
In this retrospective, IRB-approved and HIPAA- compliant study, the requirement to obtain informed consent from the study subjects was waived and the research was limited to the use of health/medical records. A search for patients who underwent chest port catheters was conducted by means of the divisional scheduling software (Hi-IQ; ConexSys, Albion, Rhode Island), and all patients who underwent chest port implantation between September 2009 and February 2010 were included in this study. The data collected included patients' demographics (age, sex) diagnosis, procedure and immediate complications. Follow-up data were collected for three months following port placement to assess complications.
Study groups
The study cohort was divided into two categories: control and accessed groups.
The control group included patients who had their chest ports implanted but not utilized immediately. The accessed group consisted of patients who required administration of IV medications immediately after port placement. The accessed group included inpatients and outpatients who needed to commence chemotherapy on the same day of port placement and have their ports accessed upon completion of the procedure in the operating room with a Huber needle. The needle was then left indwelling for immediate use.
In our clinical practice, it is customary to leave ports accessed for immediate use if patients required immediate intravenous access for chemotherapy or if the patients are inpatients; however, most of our patients undergo port implantation days before commencing intravenous therapy.
Procedure technique
All patients had coagulation parameters assessed within one month of the procedure and any coagulopathies were corrected so that the international normalized ratio (INR) was <1.5 and the platelet count was ≥ 50 000. Procedures were performed with intravenous moderate sedation (n=464), per hospital protocol with fentanyl citrate and midazolam hydrochloride; or with general anesthesia support (n=3), based upon the patient's American Society of Anesthesiologists (ASA) physical status classification. Prophylactic preprocedure antibiotics were administered in all patients in the form of either 1 g of cefazolin or 600 mg of Clindamycin, administered intravenously within one hour of the procedure.
All ports were placed by the interventional radiology service according to a standard protocol. Operators included interventional radiology (IR) attending physicians, and IR fellows, experienced procedural nurse practitioners and radiology residents under direct attending physician supervision.
Procedures were performed using strict sterile technique that included skin preparation with 2% Chlorexidine, maximal sterile barriers and gown, cap, mask and gloves. The preferred access for implantable port-a-catheter placement was the right internal jugular vein followed by the left internal jugular and subclavian veins. The target vein was punctured using direct ultrasound guidance and a 21-gauge micropuncture set. After gaining central venous access and placing a guidewire, serial dilatation of the venotomy site was performed and an 8 French peel-away sheath was introduced over the guidewire. Using combined sharp and blunt dissection, a subcutaneous pocket was then created in the anterior chest wall along with a subcutaneous tunnel for catheter placement. The catheter was then introduced through the peel-away sheath and was positioned with the tip at the cavo-atrial junction. The peel-away sheath was then removed and the catheter was trimmed and connected and secured to the port stem. The subcutaneous pocket incision was closed with interrupted/running 3-0 Vicryl subcuticular sutures and interrupted 3-0 Vicryl subcutaneous sutures. Steri-strips were placed over incision and a sterile dressing applied. All ports were terminally flushed with 4 mL – 5 mL of 100 units per mL of Heparin. All patients received post-procedural instructions to avoid strenuous activity and heavy lifting for seven days, and to keep the dressing dry for three days after the procedure. The access Huber needle was inserted in patients who required immediate IV therapy upon completion of the procedure and a dressing was applied over the needle.
Contraindications for port implantation included: sepsis or unaccounted fever of >24 hours duration, active skin infection, coagulopathy/chronic anticoagulant use, severe thrombocytopenia, venous thrombosis involving the jugular vein, subclavian vein and/or superior vena cava and bevacizumab (Avastin) administration within two weeks before or after port implantation.
Classification of complications
Complications were classified according to the SIR outcomes system (7). Major complications result in admission to hospital for therapy (for outpatient procedures), an unplanned increase in the level of care, prolonged hospitalization, permanent adverse sequelae or death. Minor complications result in no sequelae; they may require nominal therapy or a short hospital stay for observation (generally overnight).
Statistical analysis
The incidence of complications between the two groups was compared using a Student t test, and a P value less than .05 was considered statistically significant. Results are given as mean ±SD.
Results
Patients' characteristics
A total of 467 ports were placed in 465 patients. There were 259 women and 206 men with a mean age of 59 years. Fifty ports (50/467, 10.8%) were placed in 50 patients in the accessed group and 417 ports (417/465, 89.2%) in 415 patients in the control group. The procedural indications were cancer (head & neck, gastrointestinal and gynecologic tumors) in 99% and non-oncologic purposes (long-term central venous access for antibiotics and frequent infusion therapies) in 1%. There were no statistically significant differences in patient demographics, indications and underlying diseases between the two groups (Tab. I).
Patient Characteristics in both Groups
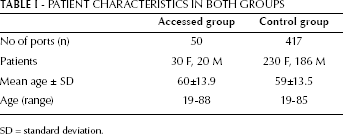
SD = standard deviation.
Procedures
A total of 467 implantable chest ports were placed, with access via the right internal jugular vein (n=398), left internal jugular vein (n= 68) and right subclavian vein (n=1). The distribution of devices implanted is given in Figure 1.
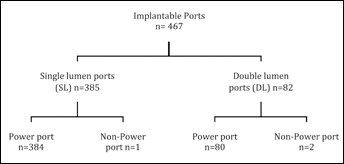
Schematic representation of the types of implanted devices.
Complications
The overall complication rate was 0.6 % (n=3). According to the SIR classification, all three complications were considered major. Two complications (hematoma causing skin necrosis and port thrombosis) occurred in the control group and one (port infection) in the accessed group (Fig. 2). The latter occurred 17 days after port implantation in a patient who presented with fever and bacteremia. The port was removed and catheter tip cultures demonstrated colonization by staphylococcus aureus. The other two complications were treated with removal of the port in the patient who developed skin necrosis; and anticoagulation treatment for the patient who developed venous thrombosis.
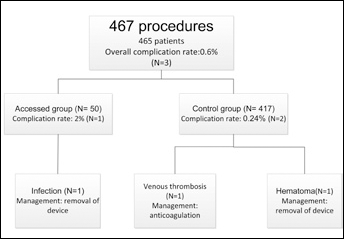
Schematic representation of all complications and outcomes per group.
Infection rates after port placement were 2% (1/50) in the accessed group and 0% in the control group (0/417). There was no statistically significant difference in the overall complication (P=.1) and infection rates (P=.1) among the groups.
Discussion
Given the impact of healthcare associated infections, it is very important to monitor complication rates associated with image-guided procedures. Central venous infection rates are considered an important quality indicator and close monitoring of infection rates should be part of the clinical care responsibilities of the interventional radiologist. According to the SIR, the overall procedure threshold recommended for major complications related to image-guided central venous access (subclavian, jugular, and peripheral approaches) is 3% and the suggested threshold for catheter placement-related sepsis is 2% (2). Specific major complication thresholds for venous access via the subclavian and jugular approaches are: pneumothorax (3%), hemothorax (2%), hematoma (2%), perforation (2%), air embolism (2%), wound dehiscence (2%), procedure-induced sepsis (2%) and thrombosis (8%) (2).
Infectious complications occurring beyond the immediate post-insertion period are typically unrelated to the method of placement, but instead reflect access related complications or simply the presence of a colonizable foreign body.
Contamination of the port can occur by the following mechanisms: the reservoir and internal lumen of the catheter may be contaminated at the time of the implantation or during access for infusion therapy; the port may become infected as a result of a prolonged period of access for infusion; hematogenic seeding of the intravascular portion of the catheter from a distant site may occur; and poor or inappropriate wound care may lead to infection (8).
The risks of immediate port-access after placement are related to the proximity of accessed needle to the suture line and disruption of the normal healing process adjacent to the port by attempts to place or remove the Huber needle.
These factors may increase the risk of infection and hematoma involving the port pocket. Peri-procedural catheter-related infections can be prevented with the use of correct technique and maximal sterile-barrier precautions (use of mask, cap, sterile gown, sterile gloves and large sterile drape) (9). However, the effect of immediate port-access on the rates of infection and other complications is not known.
In our study, the overall complication rate related to port placement was 0.6% (n=3). Of these complications, one (n=1, 0.2% overall rate) was related to infection, requiring removal of the port. Subsequently, catheter-related bacteremia related to staphylococcus aureus infection was confirmed, based on cultures obtained from the removed device. In the past, the overall complication rate following image-guided port placement was reported to be 8.7%, including infections and port migrations (8). When compared with other published data, the incidence of complications in our study is well below the reported 5% incidence of port placement-associated infection in an academic center (10); our results are more consistent with recent publications demonstrating a very low infection rate of less than 1% (11). Many factors affect the rate of complications experience of the operator, use of peri-procedural antibiotic prophylaxis and post-procedural wound care. One study demonstrated no statistical difference in procedural complications during central venous access placement when comparing radiology practitioner assistants, IR faculty members, IR fellows and residents (10). The use of antibiotics during the port placement procedure has been recently questioned in a study that reported no difference in infection rates regardless of whether or not antibiotic prophylaxis was used (11). In addition, that study reported that 12.5% of the patients undergoing port placement had their devices accessed on the same day for chemotherapy with no increased risk for infection (11). Our study does not demonstrate statistically? significant difference in infection rates whether the port is accessed peri-procedurally according to a standard protocol with the use of prophylactic antibiotics.
The limitations of this study include its retrospective nature, discrepancy in terms of number of patients included in each group, variable experience of the operators, use of prophylactic antibiotics in both groups and the lack of information as to how long the port remained accessed in the inpatient population. Furthermore, because of the low incidence of infection, a much larger study would be necessary to have sufficient power to draw definite and unequivocal conclusions on this subject. Nonetheless, this study still has its value and merit by raising this important clinical question, which is relevant to daily practice, while awaiting confirmation of its results by larger future trials.
The results of this study highlight the importance of addressing clinical practice concerns, such as whether or not there is an increased risk of complications if ports are used for immediate chemotherapy or TPN, and they may reassure clinicians and patients that implantable ports can be used on the same day of the implantation procedure without additional risk for infection.