
Abstract
Purpose
Relatively small radial artery may be challenging for cannulation. We investigated whether a distal tourniquet would inflate the proximal radial artery and therefore facilitate cannulation in adults.
Methods
There were two stages of the study. The first was to measure the characteristics of radial artery by ultrasound imaging before and after tourniquet in volunteers. The second was a prospective, randomized, double blind study. Forty patients (American Society of Anesthesiologists I-III) who needed artery cannulation during operation were enrolled. Patients were assigned into two groups: loosen or tightened tourniquet for proximal radial artery cannulation by traditional palpation technique. The primary endpoints were the success rates and time of first attempt success by traditional palpation technique. The time of success after two to three attempts, failure rates and complications were collected.
Results
For volunteers, the distal tourniquet significantly expanded the cross-sectional up-forward diameter (p<0.001) and the area (p<0.05), but had no effect on cross-sectional lateral-lateral diameter or circumference of proximal radial artery (p>0.05). The success rate of first attempt was higher in the tighten group (75%) than in the loosen group (15%, p<0.05), but the time for success of first attempt/two to three attempts was similar (19.33 ± 1.12/62.11 ± 37.03 sec loosen group vs. 19.07 ± 12.75/45.55 ± 8.98 sec tightened group, p>0.05). Both groups had same failure rates of 10%. No complication was observed.
Conclusions
Distal tourniquet could inflate the proximal radial artery and facilitate palpation of radial artery cannulation.
Introduction
Radial arterial catheterization is an indispensible technique for doctors, required in many hospital settings, including the emergency department, intensive care unit and operating room (1). Indications for arterial cannulation include the need for continuous blood pressure monitoring, frequent arterial blood gas analysis and repeated blood sampling for laboratory evaluation. Radial artery catheters are inserted traditionally by anatomic palpation skills. However, radial artery is relatively small, resulting in difficulty in palpation and cannulation.
The average diameters of radial artery for adults at 2 cm proximal to the styloid process of the radius are about 2 mm (2), while the inserted catheter could range from 0.9 to 1.5 mm. In hypotensive patients, the radial artery may even be flattened, making the cannulation difficult, even if the insertion attempt were successful. Further attempts may cause risks and complications such as radial artery occlusion, pseudoaneurysm, infection, hematoma and arterial spasm (3).
Our hypothesis was that if the diameter of radial artery is enlarged, the arterial cannulation success rates could be increased. Coming from routine practice that the proximal tourniquet helps the distal vein vessels bulking, we hypothesized that dismal tourniquet may inflate the proximal radial arterial vessels and facilitate artery cannulation. To testify our hypothesis, we designed the study with two tests: the first was to test the inflating effect of tourniquet in volunteers by ultrasound images; the second was to test the benefits of tourniquet on artery cannulation in patients who require continuous blood pressure monitoring during major operations.
Materials and Methods
Study design
A prospective, randomized, double blind study design was chosen. The institutional review board of Shanghai Jiaotong University-affiliated Shanghai Sixth People's Hospital approved the study and waived additional consent form other than anesthesia consent form in which the risks and possible consequences of artery cannulation were explained (approval No. 2014-19, IRB referral person: Prof. Jia Wei Ping, Shanghai Sixth People's Hospital).
Study protocol
There are two stages in the study: The first stage was to check the inflation effect of distal tourniquet on the parameters of proximal radial arteries in volunteers. Volunteers who did not need radial artery cannulation, aged between 20 and 80 years, men or women, were eligible for the study. The exclusion criteria included patients with peripheral vascular diseases and previous surgeries on the hand or arm. All the attendants were informed and agreed to the procedure.
To inflate the artery, a tourniquet was placed distally next to the right ulnar styloid process tightly for at least 10 sec to mimic the preparation time of radial artery cannulation. Because the vast majority of Chinese are right handed, the study used right radial artery only. The arteries were measured using a Sonosite Probe 9L (6 MHz) ultrasound (S-Nerve; SonoSite, Bothell, WA), at 1 to 2 cm proximal to the radial styloid process, the most common site for vascular access in radial procedures. Images were taken and saved as short video clips in short axis view by a single experienced operator before and after the tourniquet was tightened at the same site. Another anesthesiologist who did not know which image was with tightened tourniquet and which was not analyzed the images.
When the measurements were taken, a maximized artery image, that is, the time of impulse of the artery, was chosen for each radial artery. Parameters of radial artery included the cross-sectional up-forward diameter, cross-sectional lateral-lateral diameter, circumference and the inner crossover area of the artery. The demographic data of volunteers included age, weight, height, gender and body mass index (BMI).
The second stage was to test whether the tourniquet could improve the success rate of radial artery cannulation in patients after induction of general anesthesia.
During December 2013 and March 2014, patients who were assumed to require continuous blood pressure monitoring underwent general anesthesia for major elective orthopedic operation and were included in this prospective randomized double blind study. Subjects with peripheral vascular disease, histories of hand or wrist surgery were excluded. After obtaining written anesthesia informed consent, patients were randomized to two groups with sealed envelope technique according to loosen and tightened tourniquet.
Radial artery cannulation was performed by traditional palpation technique on the right radial artery, after the induction of general anesthesia to minimize the unpleasant feeling for the patients. The induction of general anesthesia included 1% propofol 1.5 mg/kg, fentanyl 3 mcg/kg, vecuronium 0.15 mg/kg. A 3-year experienced attending anesthesiologist who was blind to the tightness of tourniquet performed all cannulations at the time between tracheal intubation and start of surgery. Standard 20-G i.v. cannula (B. Braun, Germany) was used. The whole procedure followed strict sterile rules.
A stopwatch was used to calculate the time from skin puncture after the palpation of the artery to successfully connecting with a monitor. The collecting data included the success rate of first time attempt, the time for first attempt success. The success rates of two to three attempts and the time cost for success were calculated. After three failure attempts, a different insertion site was used and it was defined as a failure, even if it did not reach the artery. Failure was also defined when the needle reached artery but the cannulation was unsuccessful. At this time, the insertion site was changed and the tourniquet was taken away in either loosen or tightened group. The failure rates were counted and the complications such as hematoma and distal ischemia were also observed for 24 hours. Other collected data included the age, gender, weight, height, operation name, baseline blood pressure and blood pressure at the time of artery cannulation.
Sample size estimation
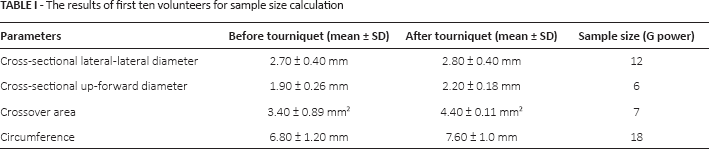
For the first stage, after obtaining mean diameters, area and circumferences of the first ten volunteers in the study (Tab. I) and assuming a two-sided α value of 0.05 (sensitivity 95%) and a β value 0.20 (study power: 80%), we determined that at least 18 patients were required (G Power, www.statisticalsolutions.net). We recruited 36 volunteers for the study.
The results of first ten volunteers for sample size calculation
For the second stage, the mean attempt in the loosen tourniquet group was 1.77 ± 0.73 and in the tightened tourniquet group 1.16. A sample size of 20 in each group would have 96% power to detect a difference in means of 0.61 (the difference between the two groups), assuming that the common SD is 0.73, and using a two group Student's t-test with a 0.05 two-sided significance level (G power, www.statisticalsolutions.net).
Statistical analysis
Unless otherwise stated, data are presented as mean ± SD. The proportions of successful insertion at the first attempt were tested by means of Fisher's exact test. Mann-Whitney tests were applied in the comparisons of the number of attempts. The paired student i-test was used for the comparison of parameters of radial artery before and after the tourniquet in the first test. Independent student i-test was used in the second test; p<0.05 indicated significance. Statistical analysis was performed using SPSS for Mac, version 17 (SPSS Inc., Chicago, IL).
Results
The inflate effect of distal tourniquet on the proximal radial artery
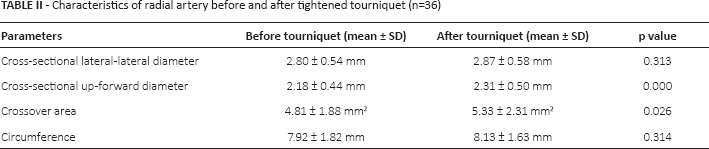
There were a total of 36 volunteers (18 male and 18 female) enrolled in the study. Their mean age was 65.78 ± 8.15 years, the mean weight was 65.72 ± 7.82 kg and the mean height was 163.47 ± 6.53 cm with the mean BMI at 24.65 ± 3.07. The parameters of radial artery before and after tightened tourniquet are listed in Table II. The radial artery's cross-sectional up-forward diameters and the inner crossover areas were enlarged significantly after the tightened tourniquet while the cross-sectional lateral-lateral diameter and circumference were unchanged. Figure 1 shows a typical ultrasound short axis view of radial artery before and after the tourniquet in a volunteer.

Typical short axis ultrasound images of radial artery at 1-2 cm to the right radial styloid process before and after tourniquet tightening.
Characteristics of radial artery before and after tightened tourniquet (n=36)
Distal tourniquet facilitated success rates of first insertion attempt for radial artery cannulation
All the artery cannulations were successful and all the patients were under continuous blood pressure monitoring during their operations. The demography of the patients enrolled in the study is listed in Table III. Most patients were undergoing elective revision of total hip replacement and pelvic internal fixation. The blood pressures at the time of artery cannulation (postinduction) were significantly lower than those before the operation due to the induction of anesthesia.
Patient characteristics
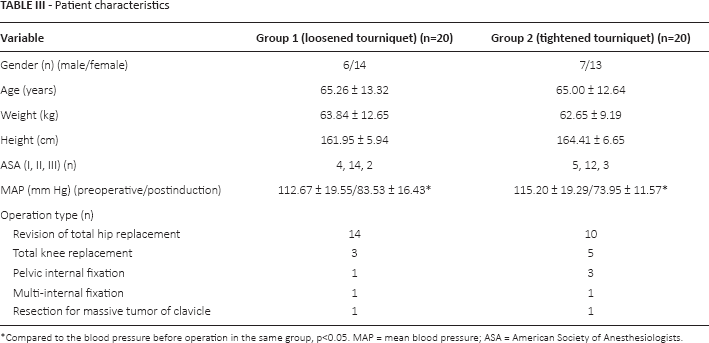
Compared to the blood pressure before operation in the same group, p<0.05. MAP = mean blood pressure; ASA = American Society of Anesthesiologists.
The success rates and time of first and two to three attempts in both groups are listed in Table IV. There was a significant difference in success rates of first attempt between the two groups, p = 0.024. The odds ratio of success rates of first attempt between the two groups was 0.13 (two-sided). There was no significant difference for the average time for first-time attempt success, neither the time for two or three attempts success between the two groups. But for the loosen tourniquet group, the time for two or three attempts success was significantly longer than that for first attempt success (62.11 ± 37.03 vs. 19.33 ± 1.12 sec, p<0.05). The average attempts for successful cannulation in the loosen tourniquet group was 1.77 ± 0.73 while it was 1.16 ± 0.63 in the tightened group.
Number of success in first attempt and two or three attempts and their time cost
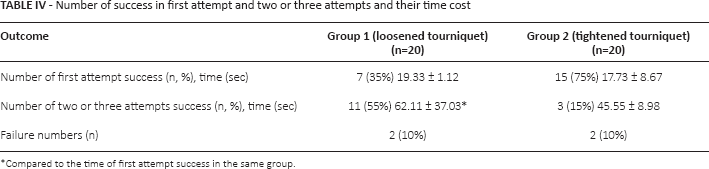
Compared to the time of first attempt success in the same group.
In both groups, no patient suffered from hematoma or distal ischemia after the operation due to long pressure on the insertion sites, at least 3 min if the artery was reached but the cannulation failed.
Discussion
Our studies testified that a tightened distal tourniquet could inflate the proximal radial artery through expansion of the cross-sectional up-forward diameter and the inner crossover area, and these changes could facilitate successful radial artery cannulation for patients under general anesthesia.
To our knowledge, this is the first study testing the inflation effect of distal tourniquet on proximal artery. Similar to the proximal vein tourniquet enlarging the distal vein as a routine practice for vein cannulation, the distal tourniquet produced a similar effect on the proximal artery. Our ultrasound images showed that with the tightened tourniquet, the cross-sectional up-forward diameters and the inner crossover areas were significantly enlarged while the cross-sectional lateral-lateral diameter and circumference were unchanged. These results indicated that the artery tends to be round because of the inflation effect of the tourniquet.
Because of the inflation effect, the success rates of first attempt significantly improved in our clinical setting. The facilitation of the tourniquet has several advantages. First, it inflated the artery, making the palpitation easier for the performers. In the tightened tourniquet group, there were only two attempts for success, while there were several three attempts in the loosen tourniquet group. Second, the inflated artery with prolonged cross-sectional up-forward diameters gave more space for the cannulation. This is especially helpful in hypotensive patients whose arteries are flatter/collapsed. In clinical practice, we often face situations where there was flush of blood in the needle, indicating the needle reached artery, but the cannulation failed due to the flatter artery. The advantages of the distal tourniquet are prominent in patients under general anesthesia when the blood pressure was significantly lower than their pre-operative blood pressure.
There are several methods to elevate the blood pressure that could be of benefit for artery cannulation. First using medications such as dopamine and adrenaline, but most of these medicines increase the blood pressure by contraction of peripheral blood vessels, which may, in turn, further reduce the crossover area of radial artery. Second, increasing the fluid load. For hypovolemic patients this is essential. But it takes a while for blood pressure to be back to normal and fast massive fluid infusion may have several other complications such as congestive heart disfunction. The tightened tourniquet could quickly, if not immediately, inflate the proximal radial artery with almost none systemic effect.
The success rates of first attempt in the loosen tourniquet group were consistent with other researchers’ results of about 34% in palpation technique (4, 5). Our success rates of first attempt in the tightened group improved significantly and almost reached that success rate in ultrasound-guided group described in an early publication (4). The reason we did not use ultrasound to facilitate the radial artery cannulation was because the design of the study was a double-blinded strategy. With the help of ultrasound, only single-blinded protocol could be used. Due to similar results between tourniquet and ultrasound, we are interested to compare the effect of the two in the future.
In recent literature, ultrasound has been used successfully to facilitate radial artery cannulation in adults (6), children (7) and even in infants (8). However, ultrasound machines may not be available everywhere. A tourniquet is a cheap, simple tool available in almost every clinical settings and it can be used for both vein and artery cannulation.
The disadvantages of the distal tourniquet should be noted. First it was placed close to the insertion site, which may interfere with the performance. So it needs practice for performers to get used to the tourniquet. Second, once there is a failure of cannulation with an artery insertion, the bleeding of the artery could be more severe under the tourniquet; therefore, it should be removed immediately, just as in the situation when a vein cannulation failed.
Conclusion
A distal tourniquet inflates the proximal radial artery by enlarging the cross-sectional up-forward diameter and area of the artery. This, in turn, could facilitate the success rates of radial artery cannulation. This tool is particularly useful when ultrasound machine is not available.
Footnotes
Financial support: None.
Conflict of interest: None.