
Abstract
Purpose
About 8 years ago, we approached an intraoperative transluminal angioplasty (ITA) performed during the arteriovenous fistula (AVF) creation, to treat arterial or venous stenosis diagnosed by a preliminary ultrasound examination. Objective of this study is to validate the efficacy of ITA.
Methods
Early failure (EF) and failure to mature (FTM) were evaluated in 69 AVFs with ITA created in 58 patients in the last 3 years. In the same period, 160 patients received 188 AVFs without ITA and were considered control group. Of the two groups, age, comorbid factors, sex, primary and secondary patency rate (PR) were also analysed.
Results
The two groups were homogeneous for gender and age (70.4 + 11.1 years of ITA group vs. 66.3 + 14.4, p = 0.059). The incidence of diabetes, heart disease and peripheral artery disease was higher in the ITA group (43% vs. 17%, p<0.0001, 35% vs. 6%, p<0.0001 and 56% vs. 15%, p<0.0001, respectively). EF and FTM occurred in seven and eight cases in the ITA group and in 15 and 13 cases in the controls, respectively. Total failure occurred in 24% of ITA group and 14% of the controls (p = 0.2). The primary PR at 6, 12 and 24 months was 78%, 72% and 59% for ITA group and 85%, 78% and 78 % for control group (p<0.01). The secondary PR at 6, 12 and 24 months was 91%, 86% and 80% for ITA group and 95%, 95% and 92% for the controls (p<0.01).
Conclusions
Our ITA approach has allowed satisfactory results in patients at a high risk of AVF failure.
Introduction
Chronic maintenance haemodialysis (HD) requires stable and repetitive vascular access (VA). In order to achieve the best outcome in HD, it is widely accepted that the arteriovenous fistula (AVF) represents the optimal VA according to the K-DOQI guidelines (1). The order of preference for AVF placement in patients with kidney failure who will become HD dependent is, first, the wrist (radial-cephalic) primary AVF (evidence). Early failure (EF) and failure to mature (FTM) are frequently complications of distal AVFs (2). The incidence of EF and FTM has been reported to be as high as 20-50% (3-7). The high prevalence of diabetes and atherosclerosis in elderly uremic patients starting HD has led to the increase in the risk of AVF EF and FTM caused by pre-existing arterial diseases (8-11). Sclerotic lesions and small caliber of veins contributes to increase the incidence of EF and FTM (12, 13). The extensive use of upper limb ultrasound examination before performing the AVF creation, as recommended by the K-DOQI guidelines, allows better results by optimizing vessel selection, excluding vessel unsuitable for AVF creation (9). To reduce the incidence of EF and FTM and to increase the number of vessels suitable to create distal AFVs, about 8 years ago, we started up a technic of intraoperative transluminal angioplasty (ITA). At the beginning, we used the aid of interventional cardiologist to standardize the procedure. The ITA was used to dilate arterial stenosis diagnosed during preoperative ultrasound mapping (14, 15); later, the technique was also applied to the vein sclerotic or with focal stenosis (Fig. 1). Objective of this study is to validate the efficacy of ITA; so, EF and FTM of AVFs were evaluated in all patients undergoing ITA during the creation of a distal AVF from August 2010 to December 2013.
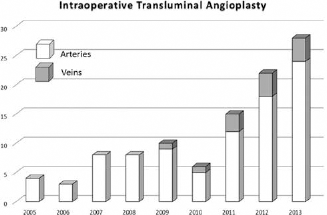
Numbers of intraoperative transluminal angioplasties performed in the years.
Patients and Methods
From August 2010 to December 2013, 218 consecutive patients receiving 257 AVFs in the middle and distal third of the forearm in our centre were analysed. Fifty-eight patients underwent the creation of 69 AVFs with ITA. In 58 cases ITA was performed on the radial artery, in 11 cases on the cephalic vein. In six cases, the ITA was performed contemporary on the radial artery and the cephalic vein. The series of 160 patients who underwent the creation of 188 AVFs without ITA in the same period were considered the control group. Primary end-points were the EF and the FTM of each AVF. Secondary end-points were the primary and secondary patency rate. EF and FTM were considered the thrombosis of the AVF within 3 months and the maturation not enough to permit routine two needles dialysis with adequate blood flow within 3 months of AVF creation, respectively. The primary patency was considered the interval from the time of access placement until any surgical intervention designed to maintain or reestablish patency or access thrombosis. The secondary patency was considered the interval from the time of access placement until access abandonment, with the creation of a new AVF in another district or a creation of a new VA (graft or CVC), including intervening manipulations or revision designed to maintain or reestablish functionality in thrombosed access. Revision of AVF was defined in accordance with recommended standard (16). All the AVFs were created by the same interventional nephrologist. Among ITA-group and control group, age, sex and comorbid factors were analysed. ITA was performed during AVF creation, using the arterial or venous incision, necessary because of the anastomosis, to introduce the necessary devices for the angioplasty (14, 15). All patients underwent preoperative sonographic mapping. Diagnostic criteria of arterial stenosis considered the presence of stenosing plaques, detected in B-mode and confirmed by colour Doppler. Once the stenosis has been identified, its length and diameter were measured; then, the diameter of the vessel immediately upstream and downstream was evaluated. These measurements, useful for calculating the percentage of stenosis, were necessary to establish the dimensions of the angioplasty ballons. The degree of the stenosis was calculated using the formula shown in brackets [{(% stenosis = reference stenosis – stenosis diameter)/reference diameter) × 100}]. All stenosis higher than 20% were treated with ITA. Arteries with multiple plaques were included in the ITA group regardless of the percentage of stenosis. Veins and arteries resistant to the hydrostatic dilatation during the surgical procedure also underwent ITA. Hydrostatic dilatation of vessels was performed after the exposure of the radial artery and the cephalic vein by cannulation of vessels with a small needle, after the clamping of vessels injecting saline solution (Fig. 2). The resistance to hydrostatic dilatation was due to sclerosis and calcifications of arterial wall and sclerotic lesions of veins (Fig. 3). The angioplasty was performed with balloons (SAVVY CORDIS, Jhonsos & Jhonson, Ireland) of diameter 1 mm greater than that of the vessel to be treated, using a 4-French valved introducer and a 0.018-inche guide wire. A long segment of vessel, from the elbow to the site of anastomosis, underwent angioplasty. The size of balloons used was from 3 to 4 mm. The inflation pressure required to dilate the vessels ranged from 6 to 10 atm. Ultrasound guidance was used in case of focal stenosis to control the correct position of balloon in the stenosis area and the efficacy of angioplasty. Side effects were valuated. The statistical analysis was performed by t-test, χ 2 test and Kaplan-Mayer survival table.
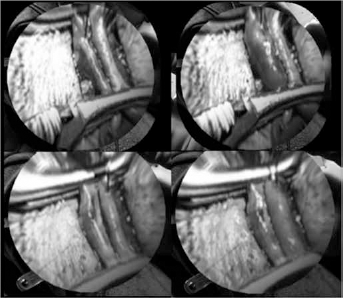
Hydrostatic dilatation (left before, right later) of a vein (up) and an artery (down) performed by cannulation of the vessels with a small needle, after the clamping and after injecting saline solution.
Results
The characteristics of patients are reported in Table I. The two groups were homogeneous for gender and age (70.4 + 11.1 years of ITA group vs. 66.3 + 14.4, p = 0.06). In the ITA group, the incidence of diabetes (43% vs. 17%, p<0.0001), heart disease (35% vs. 7%, p<0.0001) and peripheral artery disease (56% vs. 15%, p<0.0001) was higher. The patients with severe lower limb ischemic lesions (gangrene or amputation) were seven in the ITA group and none in the control group (p<0.0001). Of 69 AVFs of the ITA group, 55 (80%) were localized in the distal thirth of forearm and 14 in the mean thirth of forearm. Of 186 AVFs of the control group, 147 (79%) were localized in the distal thirth of forearm and 39 in the mean thirth of forearm. Table II summarizes the results. EF occurred in seven cases in the ITA group and 15 in the controls (p = 0.59). FTM occurred in eight cases in the ITA group and 13 in the controls (p = 0.23). Total failure occurred in 24% of the ITA group and 14% of controls (p = 0.2). No side effects occurred. The primary patency rate at 6, 12 and 24 months was 78%, 72% and 59 % for the ITA group and 85%, 78% and 78 % for the control group (p<0.01) (Fig. 3). The secondary patency rate at 6, 12 and 24 months was 91%, 86% and 80 % for the ITA group and 95%, 95% and 92% for the control group (p<0.01) (Fig. 4).
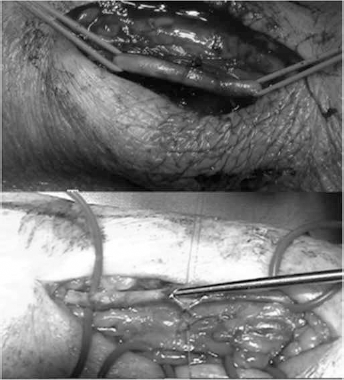
Examples of a vein (up) and an artery (down) resistant to hydrostatic dilatation.
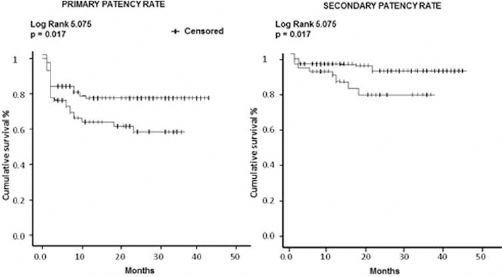
Primary and secondary patency rate.
Characteristics of patients

Results

Discussion
In recent years, high prevalence of diabetes, atherosclerosis and advanced age of uremic patients starting hemodialysis has led to the increase in the risk of VA failure caused by pre-existing arterial diseases or venous lesions, including both EF and FTM. EF and FTM are more frequently complications of distal AVFs (2). The use of suboptimal arteries and veins for AVF creation is an important limitation to increase the prevalence of distal radio-cephalic AVFs as recommended by the NKF-DOQI guidelines (1). The extensive use of upper limb ultrasound examination before performing the AVF creation allows better results by optimizing vessels selection (9) but does not increase automatically the prevalence of distal AVFs. To rescue suboptimal arteries and veins diagnosed by ultrasound examination or with evident resistance to hydrostatic dilatation and to increase distal AVF creation, we started up the technique of ITA. The outcomes of our experience can be considered satisfactory. The ITA group showed the same incidence of EF and FTM as that of controls, despite the fact that the two populations had a risk of AVF failure completely different. In fact, in the ITA group, was higher the incidence of diabetes (43% vs. 17%) (p<0.0001), cardiovascular disease (35% vs. 7%) (p<0.0001), peripheral arterial diseases (56% vs. 15%) (p<0.0001) and incidence of severe lower limb ischemic lesions (gangrene or amputation) was higher. A bias of our statistical analysis is the different number of cases of the two groups. Other authors have shown that the intraoperative angioplasty may be an option to be used in clinical practice to dilate small veins reporting good outcomes (17, 18). In our experience, we used angioplasty only in case of focal venous stenosis and when the vein is diffusely sclerotic. Other authors have reported three cases of central vein stenosis correction by traditional radiological angioplasty during the AVF creation (19). Good outcomes were reported performing radial, brachial and ulnar artery PTA in HD patients with access thrombosis, insufficient blood flow and severe upper limb ischemia (20). Other experience showed positive effects with PTA of the forearm artery and veins in nonmaturing autogenous distal fistulas for haemodialysis (21-25). Some of these experiences can be considered comparable to our ITA experience. In fact, the average interval from the surgical creation to the endovascular treatment of these relationships was 3.5 ± 1.7 months (21-25), so it is likely that some arterial lesions were existing prior to the creation of AVFs. In one of the reports, the authors admitted that patients with diabetes mellitus and distal arm arteriosclerosis had not been evaluated at the time of access creation because surgeons thought these pathologies would not prevent access development (22).
Regarding the primary and secondary patency rate, we observed better results in the control group. In absolute terms, the primary and secondary patency rates of the ITA group at 2 years, 59% and 80%, respectively, can be considered a satisfactory outcome, considering the high risk of fistula failure of the patients and that the AVFs were located in the distal forearm.
An important ITA advantage is the absence, in our experience, of side effects and the low invasiveness of the technique. In fact, compared with PTA performed later, the creation of AVF, which requires cannulation of a nonmatured vein on an artery and contrast medium usage, ITA is simple and easy to perform.
Conclusion
However confirmed by many studies, the endovascular treatment is an important option to reduce the FTM and the EF of AVF caused by arterial diseases or small calibre of veins. Many authors perform the PTA after the creation of fistulas. When the arterial or venous stenosis are pre-existing the AVF creation the ITA can be considered a technique with low invasiveness compared to the PTA. In conclusion, our approach with ITA can be considered valid and worthy of being continued, having allowed us to obtain the same clinical success rate of AVFs in two populations that, given the incidence of comorbidities, had a completely different risk of AVF failure.
Footnotes
Conflict of interest: The authors have no conflict of interest.