
Abstract
Questions have been raised whether there is a lack of appropriate training in access creation and maintenance, and if training juniors in arteriovenous (AV) fistulas may affect the outcome. A survey was undertaken to study “experts” opinion in access training using a closed questionnaire. The majority of “experts” consented that there is a lack of appropriate training in access creation and maintenance in a great extent, although they located the main deficit regarding access training in the pre-operative planning and decision making.
Regarding the second question, a literature search revealed only four studies, comparing the outcomes of AV fistulas created either by consultant surgeons or trainees. A meta-analysis performed revealed that 1-year patency rate was not statistically significant different among access procedures created either by consultants or trainees. Access surgery shares the same basic principles with vascular surgery and provides a valuable workload for the trainees and is a necessity to become a building component in all “core” vascular curricula; the required skills can be acquired with the trainees operating independently simple cases, as the latter is not leading to suboptimal outcomes.
Introduction
It is generally accepted that high-quality patient care can only be provided if physicians are well prepared for this task through training during their residency. Training in vascular access influences attitudes towards proper planning, increases the use of autologous arteriovenous fistulas and avoids central venous catheter insertion whenever possible. However, the question “what is the best training for vascular access surgery” has not an easy answer. As “a problem put is half solved”, we set questions raised regarding training in “experts” and investigated whether training juniors in access surgery may affect the outcome in the existing literature.
The view of “experts”
To investigate experts’ point of view regarding access training, a closed questionnaire was developed, consisting of six different questions using the existing free software SURVEYMONKEY® (Tab. I). The questionnaire was sent to members of the editorial board of the Journal of Vascular Access or to invited speakers in the annual course of the Vascular Access Society with available e-mails (n = 49). The target group consisted of vascular surgeons, access surgeons, nephrologists and interventional radiologists from Europe, USA and Japan and all were considered “experts” in the field of access. Of the 49 “experts” contacted, 32 (65%) completed the survey.
Experts’ answers in the questionnaire
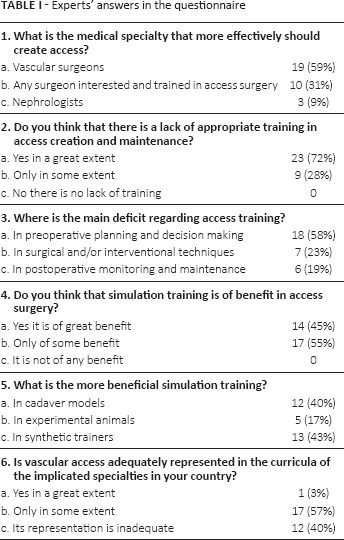
In the first question, the vast majority (90%) of the respondents pointed out who is the target population to be trained to create access. Vascular surgeons as well as any surgeon interested and trained in access surgery were voted as those who more effectively could create access (Tab. I). However, the decision what specialty should perform access surgery depends mostly on local conditions. In areas where vascular surgeons are few or unwilling to create access, other surgical specialties or nephrologists take over. Vascular surgeons were the most common surgical specialty performing access procedures across the countries included in the Dialysis Outcome and Practice Patterns Study (DOPPS); however, notably, country differences were evident and in Italy nephrologists performed the most vascular access procedures in the majority of facilities (85%), while in USA, 31% of facilities were served by general surgeons (1).
The influence of creator's specialty on access type selection was found not significant in a previous study (2), and although that impact on access outcomes has not been addressed in comparative studies, there are authors reporting excellent outcomes of AV fistulas created by nephrologists (3, 4). In contrast, creator's level of training was found in DOPPS affecting significantly the type of access placed; for every doubling of the number of fistulas placed during training, there was a 2.2 higher odds of placing a fistula instead of a graft in practice (1). In addition, the risk of primary fistula failure was 34% lower when placed by surgeons who created more than 25 vs. less than 25 AV fistulae during training (1).
In the second and third questions, the majority of “experts” (72%) consented that there is a lack of appropriate training in access creation and maintenance in a great extent, although they located the main deficit regarding access training in the pre-operative planning and decision making (58%) and in a lesser extent in the absence of skills in surgical and interventional techniques (23%) (Tab. I).
There is a concern about surgical competence of young vascular surgeons due to the reduced training time because of the working hours’ reduction, as a result of the implementation of the European working time directive (5). With this restricted training time, virtual-reality simulation has become important for surgical or endovascular training and helps reducing the negative impact on technical learning curves (6, 7). Evaluation of the acquired skills following such simulation should be performed and an important aspect is the use of objective structured assessment of technical skills rating scales (OSATS) (7). Dialysis access simulators can range from simple anastomosis suturing technique learning devices to pulsatile dialysis access box simulators or computer-designed simulators to practice interventional procedures and relevant skills can be learned in the simulation environment before exposing patients to procedures (8, 9).
It is interesting that experts’ view in the fourth question regarding simulation training in access surgery is that the latter is only of some benefit (55% of answers), probably thinking that long-time apprenticeship in contact with senior surgeons, nephrologists and interventional radiologists cannot be replaced. However, on the contrary, a sufficient number of experts (45%) believe that simulation training is of great benefit in access surgery. Simulation training in cadavers and in synthetic trainers was of equal benefit according to experts’ opinion (40% vs. 43%), although simulation in experimental animals was considered inferior (Tab. I).
In the last sixth question, 40% of experts consider that access surgery is not adequately represented in the curricula of their specialties, while 57% consider that it is represented but only to some extent. However, access surgery will represent a larger part of the total vascular surgery workload in the future, as the need for renal replacement therapy increases and the open vascular procedures decline in favour of endovascular ones (10). In agreement with this, the annual average access procedures performed by residents in USA were 18 in 2001 and increased to 34 in 2007 (11); additionally Fitridge et al have suggested access surgery to be included as a separate module within the new Australasian curriculum for vascular and endovascular surgery with 10% of the total training time to be spent on it (12).
The effect of juniors’ training on outcome
Questions have raised that juniors creating AV fistulas may have suboptimal outcomes harmful on patients’ health. A literature search revealed only four non-randomized studies, comparing the outcomes of AV fistulas created either by consultant surgeons or trainees with conflicting results (13–16). Three studies found no statistically significant effect (13–15), while in one the trainees’ outcomes were inferior to the consultant's ones in a significant level (16) (Tab. II). A meta-analysis was performed using the random effects model because apparent heterogeneity existed between studies (I 2 = 55%). Patency rates were extracted from Kaplan-Meier graphs in the corresponding articles, and the outcome events represented the number of failures in 1 year. The pooled effect of the four included studies was that 1-year patency rate was not statistically significant different among access procedures created either by consultants or trainees (Fig. 1), confirming that patient care regarding AV fistula creation appears safe and of equal quality when delivered by residents. However, it is of notice that in all the included studies, the pre-operative examination and planning was made by the consultants, illustrating that a successful access is based more in a detailed pre-operative assessment rather than in a technically perfect surgical performance. Access surgery is an opportunity for juniors to operate independently (with the consultant available in the hospital if required) allowing acquisition of required surgical skills at no patients’ cost.
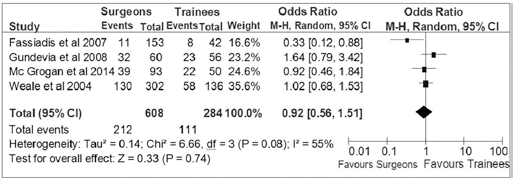
Forest plot with a pooled estimate (♦) of 1-year patency in AV fistulas created by consultants vs. AV fistulas created by trainees. Odds ratios are shown with 95% confidence intervals. (Analysis with the free RevMan 5.2 software, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark; 2012).
Characteristics of the included studies
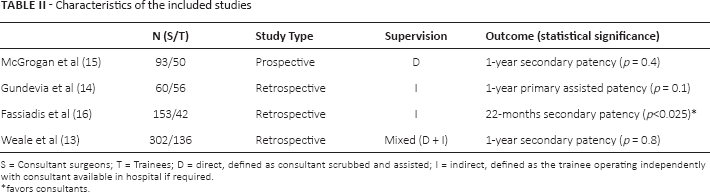
S = Consultant surgeons; T = Trainees; D = direct, defined as consultant scrubbed and assisted; I = indirect, defined as the trainee operating independently with consultant available in hospital if required.
favors consultants.
Discussion
In vascular surgery but especially in access surgery, putting the stitches in the right place is the easy technical part, based on the well known principles. However, strategic planning starting with early referral and including the proper selection of the dialysis modality, the type and site of access and when to maintain, salvage or abandon the access represent the key components to be learned (8, 10). Terms such as “steal”, “maturation” and “recirculation” are unique in access surgery; also, redo procedures are the rule and not the exception in contrast with the rest modules in vascular surgery, rendering all theoretical aspects of access surgery within vascular surgery curricula mandatory. In order to eliminate the deficit in access surgery training—a finding confirmed and in the survey performed—a customized training course with examinations at the end has been proposed (8). The examinations, written and oral, should be validated to ensure trainee's competency in theory and in their ability to choose the best access algorithm in given patients’ scenarios. Passing the examination successfully will lead to certification in access surgery (8). Nevertheless, it is of question whether theoretical knowledge is all we need to measure and require from a young surgeon to verify that he/she is able to carry out his/her professional functions effectively. Tests of knowledge currently dominate most institutional examinations and although important represent incomplete tools, as there is more to practice in medicine—and in access surgery—than knowing (17).
In order to bridge the gap between theory and practice, simulation models in access surgery can be used (18). Following the aviation safety models, patients and public no longer accept the John Dewey's “learning by doing” training theory, as it leaves any inadvertent learning curve cost on patients’ side. Consequently, simulation training has definitely the benefit of skill acquisition before exposing patients to procedures and when performed on largely realistic cadaver arms was found superior to simple plastic models after assessment of the gained skills (19). The assessment of the acquired knowledge and skills at the end of the training period is of paramount importance and a more valid indicator for trainees’ competence should be based on their outcomes rather than the number of procedures performed or years spent in a teaching hospital (9).
Miller describes nicely the four levels of competence measurements, including assessment of knowledge (the trainee “knows” access in theory), “knows how” indicating he/she is competent to choose the best access algorithm in given patients’ scenarios, performance (“shows how” in cadaver or other simulation), and “does” creating an AV fistula in a patient (17) (Fig. 2).
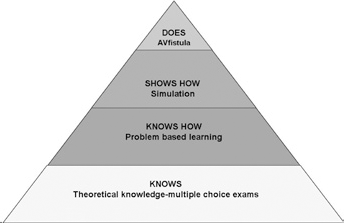
The Miller's pyramid of competence acquisition (Inspired by Miller GE (17)).
The ideal facility for access creation has not been clearly defined and obviously interferes with training. A centralized access centre is more likely to afford expensive infrastructure, to permit the creation of all spectrum of procedures and the appropriate management of all types of complications. However, centralization of access services may lead to overspecialization with a negative effect in the access surgery workload and training opportunities in the average vascular surgery departments. Access surgery uses very similar open or interventional techniques with many other vascular procedures (e.g. anastomoses, stents, grafts) and is able to provide the volume of work necessary for a rapid improvement of trainees’ learning curves, apart from somehow less demanding, as in most cases, the vessels are close to the surface and more easily handled. Access surgery additionally allows trainees to get familiar with micro-instruments, magnifying loops and colour Doppler ultrasound practice. As access surgery shares the same basic principles with vascular surgery and provides a valuable workload for the trainees, it is a necessity to become a building component in all “core” vascular curricula.
In conclusion, the best training in access surgery should be based on systematic theoretical knowledge of all the related aspects with an emphasis on the pre-operative assessment and planning, as a successful access is based more in a detailed pre-operative assessment rather than in a technically perfect surgical performance. Access surgery training should be completed with acquisition of the necessary skills with the trainees operating independently simple cases, as the latter is not leading to suboptimal outcomes.
Footnotes
Financial support: The authors have no financial disclosures to make.
Conflict of interest: The authors have no conflict of interest.