
Abstract
Purpose
In the Netherlands, 86% of patients start renal replacement therapy with chronic intermittent hemodialysis (HD). Guidelines do indicate predialysis care and maintenance of a well-functioning vascular access (VA) as critical issues in the management of the renal failure patient. Referral to the surgeon and time to VA creation are important determinants of the type and success of the VA and HD treatment.
Methods and Results
Data from a national questionnaire showed that time from referral to the surgeon and actual access creation is <4 weeks in 43%, 4 to 8 weeks in 30% and >8 weeks in 27% of the centers. Pre-Operative ultrasonography and postoperative access flowmetry are the diagnostic methods in the majority of centers (98%). Most facilities perform rope-ladder cannulation with occasionally the buttonhole technique for selected patients in 87% of the dialysis units. Endovascular intervention for thrombosis is practiced by 13%, surgical thrombectomy by 21% and either endovascular or surgery by 66% of the centers. Weekly multidisciplinary meetings are organized in 57% of the units. Central vein catheters are inserted by radiologists (36%), nephrologists and surgeons (32%).
Conclusions
We conclude that guidelines implementation has been successful in particular regarding issues as pre-operative patient assessment for VA creation and postoperative surveillance in combination with (preemptive) endovascular intervention, leading to very acceptable VA thrombosis rates.
Introduction
Patients with end-stage renal disease (ESRD) need renal replacement therapy (RRT) with renal transplantation, chronic hemodialysis (HD) or peritoneal dialysis (PD). The key factor for successful HD is a functioning vascular access (VA) and it is widely accepted that the optimal choice for VA is an arteriovenous fistula (AVF). European and Dutch guidelines on VA do advise the use of autologous AVFs as the preferred type of access (http://www.vaat-chirurgie.nl/files/Richtiijn%20Shuntchirurgie%202011.pdf) (1). The use of arteriovenous grafts (AVG) or central vein catheters (CVC) as a last resort option is restricted to complicated patients with multiple failed AVFs. Successful AVF maturation and long-term function depend on several factors like patient demographics (age, comorbidities, presence of diabetes), time of referral for access operation and pre-operative vessel assessment. In addition, strict surveillance with preemptive surgical and/or endovascular intervention improves the outcome of AVFs and AVGs and may increase long-term patency rates.
The multidisciplinary Dutch guidelines on VA were published in 2011 and contain evidence-based recommendations on predialysis care, strategy for access creation and management of access complications (http://www.vaat-chirurgie.nl/files/Richtlijn%20Shuntchirurgie%202011.pdf). In addition, organization of access care and the need for multidisciplinary meetings are addressed (Tab. I). A multidisciplinary team approach, with involvement of dialysis nurses, vascular surgeons, nephrologists and interventional radiologists, is mandatory to achieve an optimal result of VA care.
Recommendations of the Dutch guidelines on hemodialysis vascular access
AVF = arteriovenous fistula; AVG = arteriovenous graft.
To search whether VA guidelines are implemented in the daily practice, a survey among Dutch dialysis facilities was performed concerning the strategy of VA planning and the management of access provision and maintenance in the Netherlands.
Incidence and prevalence of RRT in the Netherlands
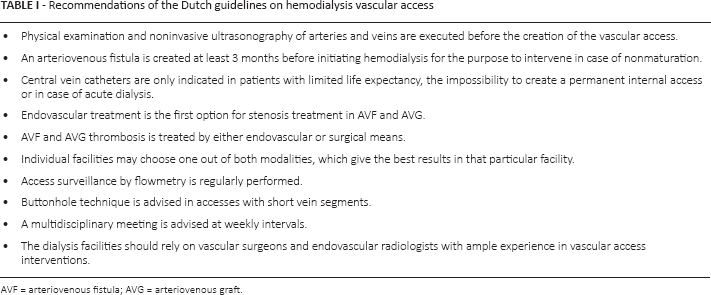
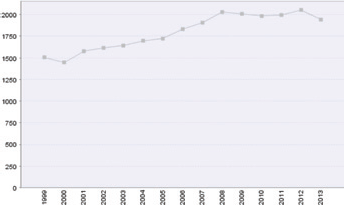
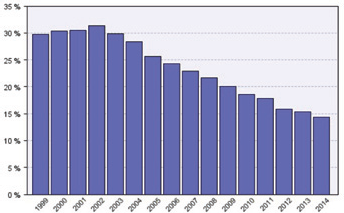
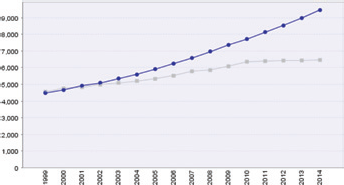
A total of 15,923 persons received RRT in the Netherlands on 1 January 2014 with 9,460 patients living with a functioning renal transplant and 6,463 prevalent patients having either HD (5539) or PD (924) treatment. The incidence of new patients with ESRD is 1,943 patients, which means an incidence rate of 115 patients per million population (data Renine 2014 [http://www.renine.nl)]. From 2008 to 2014, the incidence rate remained stable (Fig. 1) with a constant decline in PD patients (2008: 22%; 2014: 14% [Fig. 2]). The total number of dialysis patients remained stable from 2010 to 2014 (Fig. 3). The number of elderly patients grew substantially more as compared to the younger age groups (Fig. 4). RRT was performed in 73 adult and 4 pediatric renal units. Eight university, 53 hospital and 12 satellite dialysis units provided HD treatment, either in-center or home HD.
Incidence rate of new patients per year 1999-2013. Reproduced from www.renine.nl with permission from Nefrovisie/Renine. Accessed January 2015.
Percentage of PD patients of the total dialysis population on 1 January 1999-2014. Reproduced from www.renine.nl with permission from Nefrovisie/Renine. Accessed January 2015.
Number of prevalent patients on 1 January 1999-2014. HD and PD patients (grey line) and patients with a functional renal transplant (blue line). Reproduced from www.renine.nl with permission from Nefrovisie/Renine. Accessed January 2015.
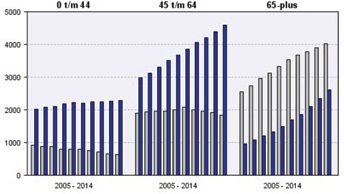
Number of patients with RRT on 1 January 2005-2014 according to age groups (years). Blue column: patients with functional renal transplant; grey column: patients on dialysis (HD and PD). Reproduced from www.renine.nl with permission from Nefrovisie/Renine. Accessed January 2015.
Methods
A questionnaire was sent to all Dutch dialysis facilities, which provided HD treatment for adult ESRD patients (age >18 years). The questions concerned different aspects of predialysis care, peri- and postoperative management and access surveillance methods. In addition, the type of healthcare workers involved in VA care was registered.
Data were collected on predialysis care and postoperative access management (situation in the year 2013). The specific questions are depicted in Table II.
Vascular access questionnaire
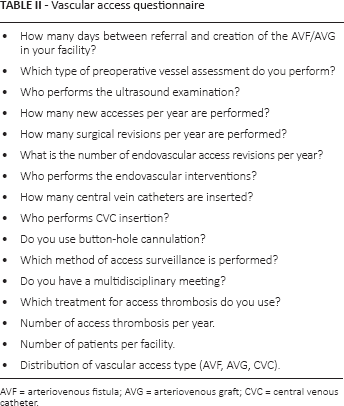
AVF = arteriovenous fistula; AVG = arteriovenous graft; CVC = central venous catheter.
Results
The response rate was 63% (46 from the 73 dialysis units), equally divided over university hospitals, general hospitals and satellite units. These dialysis units represent 74% (4072 patients) of the total Dutch HD population. The mean number of HD patients per center was 88 patients (range 12 to 199 patients; Fig. 5).
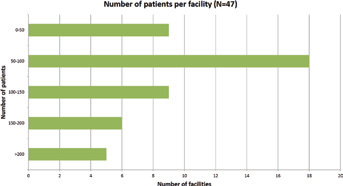
Number of patients per facility (cohorts from 0-50; 51-100; 101-150; 151-200; >200 patients).
Pre-Operative assessment and time to access surgery
Physical examination combined with ultrasonography (98%) to assess the quality of the vessels for VA was the diagnostic modality in most centers. In the majority of centers, ultrasonography examination was performed by qualified vascular technicians (98%) or radiologists (2%). The time period between referral to the surgeon and actual VA creation is 43% within 4 weeks, between 4 and 8 weeks in 30% and more than 8 weeks in 27% of the facilities (Fig. 6). According to the guidelines planning of the access operation >4 weeks after the patient is seen by the surgeon is too late.
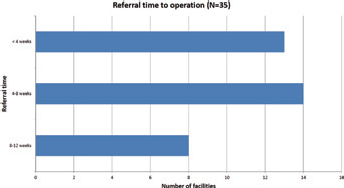
Referral time from surgical consultation to VA creation (time intervals from 0-4; 4-8 and 8-12 weeks).
New VAs and interventions
Data on surgical creation and revision of new and complicated VA were available from 39 centers. A total of 1,157 new VA and 1,653 surgical access revisions were registered in 2013. The mean number of new VA per center was 30 procedures (range 1-62) and the mean number of VA revisions 42 procedures (range 0-68).
Endovascular intervention for access complications was done in 2,529 cases (data from 41 hospitals; Fig. 7) and in the majority performed by radiologists (94%).
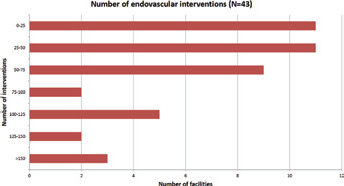
Number of endovascular interventions (cohorts from 0-25; 26-50; 51-75; 76-100; 101-125; 126-150 and >150 interventions per year).
Access management and surveillance
All renal units used flowmetry for access surveillance on a regular basis and additionally duplex scanning was performed in most facilities (91%). A weekly structural multidisciplinary meeting with nephrologists, surgeons and dialysis nurses was scheduled in 60%, while 9% of dialysis departments had meetings only on occasion because of VA problems. The rope-ladder technique was the preferred method of cannulation and buttonhole needling was used in the majority of patients in 6, occasionally in 34 and never in 7 units.
Access thrombosis and treatment
The number of access thromboses varied from 5 to 31 thrombotic episodes per center (range 0.02-0.2 episodes per patient/year). Thrombosis was treated by endovascular means (15%), surgery (21%) or both (64%). Temporary and permanent CVCs were inserted by nephrologists (34%), radiologists (36%) and surgeons (30%). In 2013, a total of 1,613 CVCs (41 centers) were implanted of which almost half of them for chronic HD treatment.
Type of VA
The type of access in prevalent patients was registered from 31 units. These units represented 59% of the total HD population in the Netherlands. Autologous AVFs were used in 71% (range 47%-78% per center), AVGs in 10% (range 2%-37% per center) and CVCs in 19% (range 7%-38% per center) of all patients.
Discussion
Data from Renine (http://www.renine.nl) show that the incidence and total number of RRT patients in the Netherlands grossly remained stable in the past 8 years. However, the number of HD patients increased by 5% per year because of the steady decline in PD patients from 22% (2008) to 14% (2014). Adequate planning of HD initiation and permanent VA placement is only possible when the nephrologist sees new patients in a timely fashion, for instance when the glomerular filtration rate (GFR) is less than 30 mL/min, and pursue referral to the vascular surgeon for VA placement when the GFR is 20 mL/min and consider initiation of RRT at 10 mL/min. Primary care physicians to assist with identification and appropriate referral of patients with advanced kidney disease can be very helpful for this purpose.
The presence of VA coordinators (VACs) improves the care of the HD patient. A quality improvement plan implemented with the coordination of specialized VACs resulted in a significant increase in the number of autologous AVFs in incident patients (from 69% to 77% [p<0.01] with 54% forearm and 23% upper arm AVFs). Prevalent AVFs increased from 61% to 64% (p<0.01). The use of temporary subclavian vein catheters declined (34% vs 11%; p<0.01), with a substantially higher percentage of jugular vein catheters (from 23% to 35%). The number of endovascular and surgical interventions for malfunctioning VA rose from 0.39 to 0.50 procedures per patient/year (p<0.001) and from 0.06 to 0.12 operations per patient/year (p<0.001), respectively (2).
Multidisciplinary VA meetings result in more effective logistics according to pre-operative diagnostics and scheduling of operation lists. In addition this approach of signalizing access problems results in a significant increase in preemptive endovascular balloon angioplasties and a significant decrease in surgical revisions, resulting in less patient morbidity. Higher primary and secondary access patencies were achieved after the introduction of an optimized care protocol (3). More than 60% of centers in the present survey have regular meetings to discuss access problem and it is obvious that there is a substantial increase in the number of endovascular interventions. A survey performed in 1999 indicated that 46% of the centers performed angioplasty on a regular basis vs 100% in 2013. Routine access surveillance was hardly done and malfunction was detected exclusively by recirculation and/or elevated venous pressures (4). Today all dialysis units use access flowmetry on a regular basis with additionally duplex scanning (only 10% in 1999). A quality improvement program based on periodical access flow measurement reduced the number of thrombotic events and reduced health care costs in patients with AVGs. Surgical thrombectomy procedures were significantly less (0.25 vs 0.63 procedures per patient/year), with an increase in elective endovascular interventions (0.88 vs 0.33 interventions per patient/year) compared to a historical time period without flow measurement (5).
In a Dutch study, physicians and dialysis staff in 11 renal units were strongly and repeatedly advised to adhere to current guidelines with extra attention for pre-operative duplex examination and salvaging of failing AVFs. Special access nurses registered all created VAs using an Internet-linked database. Twenty-two other centers served as a control group. The prevalent AVF use increased from 58.5% to 62.7% in the intervention group and from 65.5% to 67.3% in the control centers. The increase in AVF use per year was significantly quicker than in the control group (p<0.05) (6). The primary AVF failure rate among the participating centers varied from 8% to 50%. Factors related to an increased risk of AVF failure were female gender (odds ratio (OR): 1.73), RRT prior to AVF placement (OR: 1.19 per year on RRT), diabetes mellitus (OR: 3.08) and AVF placement at the wrist (compared with elbow) (OR: 1.86). The probability of AVF failure was strongly related to the center of access creation, suggesting an important role for the vascular surgeon's skills and decisions (7).
The type of VA has significantly changed in the past three decades, indicating a different patient demography with its inherent comorbidities and poor vessel quality for VA creation. In 1987 a 100% response survey among 2,195 Dutch HD patients indicated 76% AVF, 22% AVG and 2% Scribner shunt use in prevalent patients (8). Over the next decade the AVF incidence declined to 66% with a substantial increase of AVGs (30%) (4). The present survey shows a significant increase of CVCs (19%) at the cost of AVGs (10%), whereas the percentage of autologous AVFs (71%) remained fairly stable. The reason to abandon AVGs for VA is not clear, but may have been initiated by the publication of international guidelines like KDOQI (published in 2000 with update in 2006) and the Fistula First Initiative, advertising less AVG use because of poor patencies, the need for frequent revisions and hospital admissions, resulting in patient discomfort and high healthcare costs. However, CVC use as an alternative to AVGs bears the risk of infection and higher mortality rates (9). A strict protocol for catheter care is of utmost importance to achieve acceptable rates of infection (guideline recommendations: <3 infections/1000 catheter days) (10).
Management of the VA, in particular cannulation practice, is an important issue to prevent access complications and may add to an optimal patient comfort. Data from a recent study show a high incidence of cannulation failure among patient using autologous AVFs. AVF use (p<0.001) and limited length of the cannulation route (p<0.003) negatively affected the outcome of cannulation and resulted in the need for single-needle dialysis and CVC use. This was in particular seen in patients with upper arm AVFs. The conclusion of the study was that adjusted cannulation techniques, like buttonhole needling, might be indicated to improve VA outcome (11). This theory was tested in two centers which exclusively practiced either rope-ladder or buttonhole technique for AVF cannulation. Miscannulation, infiltration, aneurysm formation and the need for VA interventions were recorded. It showed that patients in the buttonhole group had more unsuccessful cannulations, compared with the rope-ladder method (p<0.0001), but the frequency of infiltrations (p<0.0001) and aneurysm formation (p<0.0001) was less. Angioplasties were more frequently seen in patients using the rope-ladder technique. A higher incidence of access infections occurred in the patients on buttonhole cannulation (12). This latter observation might be a major drawback to apply this cannulation technique for all patients and a recent meta-analysis has confirmed an overall higher infection rate in patients with buttonhole needling (13). Only a small number of Dutch renal units do use buttonhole cannulation in the majority of patients and most of the other units only in selected patients because of a limited vein length available for needling.
Conclusion
International and national guidelines have changed the scenery of HD VA management in the Netherlands. Timely referral and pre-operative noninvasive vessel assessment is common in most renal units. Multidisciplinary meetings to discuss access problems have led to an increase in (preemptive) endovascular interventions and a decrease in surgical procedures and VA thrombosis. The number of autologous AVFs has increased slightly during the past decades with a significant decrease in AVGs resulting in more permanent CVCs for chronic HD treatment.
Footnotes
Financial support: None.
Conflict of interest: None.