
Abstract
For more than 15 years, patient safety has been an issue in different domains of medicine. There is evidence for this subject and also a great need for information. First, we should be familiar with the basic terminology such as the relationship between adverse events and errors, and understand the variations of error. In patient management, besides skills and knowledge (evidence-based medicine), the ability (competence) of healthcare professionals to act and react in unexpected situations is key to prevent and treat adverse events. Not only healthcare professionals should be involved in the process but also healthy people in a way that they understand and patients in a way that they are actively involved. This paper will show how a more general view of patient safety can and should be implemented in the daily work of caregivers dealing with dialysis access in different aspects. A key factor to advance in this subject is to be open-minded and sensualized for this topic. The reader should get an idea of how an institution can create a culture of safety.
The concept of patient safety
Charles Vincent, an expert and first-line enthusiast in the field of patient safety, stated that patient safety is avoidance, prevention and amelioration of adverse outcomes or injuries stemming from the process of healthcare (1). Indeed, patient safety is related to the quality of patient care and deals with the absence of errors and preventable adverse events. All patients undergoing any treatment are at a risk to suffer harm related to medical management. An adverse event describes an unintended and undesirable outcome of a treatment and can be unrelated to a medical error. An allergic reaction to an antibiotic is always possible, but if you know that your patient has this allergy and you prescribe the drug, you can provoke a medical error. We distinguish between errors of execution as failure of a planned action to be completed as intended and errors by omission where action is not being taken (Fig. 1). Adverse events caused by an error are always deemed preventable. Medical errors can be classified in different categories besides errors of execution and omission. There can be errors at the sharp end, meaning in activities close to the patient, and errors on the blunt end, where the problem relates more to organizational issues and/or a poor process design (2). Slips and lapses are failures of a schematic behaviour and are often related to stress and fatigue. Mistakes in contrast are errors caused by a lack of knowledge, experience and/or training and should be addressed by better education and supervision.

Adverse event of a bleeding after vascular access creation due to exaggerated anticoagulation and delayed clinical control during night shift.
In 1997, Reason summarized in his organizational accident model that errors can occur related to an organization itself and its culture. Contributory factors such as the work environment, team factors, individual staff factors, task factors and patient factors play an additional role. It is to be pointed out that defences and barriers exist or should be established to prevent incidents that can harm patients (3).
Health competency
In industry, instruments to improve working processes by analysing and improving the “competence” of co-workers have been available for many years. In Germany, the term “competence” stands not only for skills and knowledge (evidence) but also for the ability of a person to act and react, respectively, to organize oneself in daily practice as well as in an unexpected situation. Heyse and Schirks et al adapted an instrument of analysis, so-called KODE®, for medicine (4). Four parts can be differentiated: the personal competence (learning to be) containing key domains such as self-management/responsibility, willingness to learn and ethical behaviour; the activity and action competence (learning to do) with outcome-oriented acting or decision making; the socio-communicative competence (learning to live together) with key aspects such as interdisciplinary knowledge and objectivity; and the methods and professional competence (learning to know) with the abilities to communicate and cooperate, team integration and management of relations. Each person can check its profile answering questions out of the four domains in two settings: under normal conditions or in an emergency. After evaluation, each candidate can see their personal strengths and weakness. An additional effect can be reached if an external person evaluates the candidate. This instrument may help doctors to find out what speciality they fit in best.
Today people should become more responsible for their own health. We have the information tools that each person can acquire knowledge and use skills to protect one's own health, that is the ability to act or react. The WHO project of health literacy was started to involve people in this process (5). There is a trend to enforce activities in health literacy to support education and self-responsibility. The next step would be that these people become sick, turn into patients and have to elaborate skills and knowledge to deal with their illness. They require competence to act and react in their clinical setting. In such circumstances, due to medical treatment and/or intervention by health professionals, the risk for adverse events is elevated. To deal with such adverse events, doctors, nurses and other healthcare professionals with specific skills and knowledge need their competences to act proactively (Fig. 2). The better the patient understands the medical situation and the better healthcare professionals are prepared and trained for their job, the more they can show attention in their daily work and the lower is the risk to harm patients.
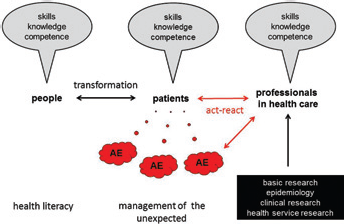
Global view on how patient safety interconnects between healthy persons, patients and healthcare professionals. AE = adverse event.
Perspectives of patients, doctors and healthcare professionals
Patients are directly involved in the process of care due to the fact that they can be confronted with adverse events. If patients check their fistulas regularly and are required to look for signs of access irregularities such as infection or bleeding, they will show up in time and heavy or even lethal complications can be prevented. Therefore, it is important for patients to get adequate information by healthcare professionals and not get blamed for asking questions. Patients should be informed and instructed as much as possible. Having trust in the dialysis care team, they can be better involved in the process of decision making and they are “in the same boat” if complications occur. For example, patients should have the courage to address violations of hand hygiene, to ask for alternatives in a treatment plan or to have their medication explained and potential side effects mentioned.
For doctors, the motto “nihil nocere” is still of value. They have to know that continuous education is important to be up to date in current science (evidence based medicine). Today more and more well organized skill trainings are offered not only to learn new techniques in access creation but also to understand the concepts in vascular access creation (6). Furthermore, the art of communication is essential to inform patients, to work well as a team and to discuss clinical problems in an interdisciplinary or even interprofessional group.
In the last years, several studies showed the benefit of vascular access coordinators in helping to run the process of patient safety, checking patients regularly for adverse events (7, 8). This is important, as due to working hour restrictions, doctors are not always available for their patients and sometimes patient-handover is lacking quality.
Safety in dialysis access patients
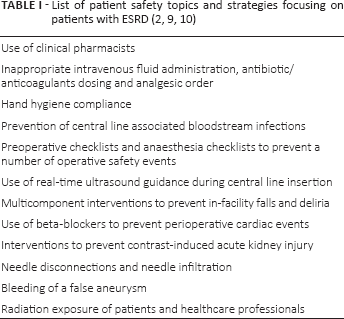
Patients with end-stage renal disease (ESRD) suffer from multiple comorbidities and are exposed to medical treatments for life with an extended risk to for a potentially preventable adverse event. Table I summarizes patient safety topics that are closely related to persons with ESRD undergoing haemodialysis (2, 9, 10).
Due to impaired renal function, the risk of drug toxicity and the need of multidrug therapy, patients can suffer from adverse medication events. The presence of pharmacists and computer-assisted prescription systems help to prevent drug overdosage or even underdosage. Systematic and regular medication reconciliation is very important and has the potential to decrease medication errors and adverse drug events (11). Paparella summarized how to safely prescribe drugs in chronic kidney disease patients and developed corresponding recommendations (12).
In patients with ESRD, especially in those with a status just before haemodialysis initiation, contrast agents can further impair renal function. In addition, radiation should be limited and necessary precautions are important. The risk of radiation exists for patients and healthcare professionals who are often inconsistently using protection devices.
Careful pre-operative planning using ultrasound and clinical evaluation is necessary for safe and successful vascular access creation, as ESRD patients frequently present with diseased arteries and veins. The use of central venous catheters or grafts should be minimized. Today, an individualized strategy in dialysis access creation is based not only on the age of the patient, the life expectancy, the comorbidities and risk factors, but also on the timing when dialysis should start (13).
A meaningful topic in vascular access creation is the pre-operative patient safety checklist introduced by the WHO, including informed consent and marking the correct operation site to prevent wrong side surgery, the checklists for anaesthesia with in-time application of antibiotic prophylaxis and the team time out before starting surgery. A postoperative debriefing checking the instruments is necessary as well as to communicate and document the postoperative plan of care (14).
Hospital-acquired infections are a relevant problem in haemodialysis patients with a high risk of morbidity and mortality. Nosocomial infections, especially in patients with catheters and grafts, can lead to adverse events with life-threatening complications such as sepsis or metastatic infections. Multiresistent germs pose a main hygiene problem on wards and also in the operating room (OR).
Unsafe cannulation is a main reason for adverse events, for example bleeding complications or the formation of false aneurysm with the risk of subsequent bleeding. For these patients, not only repair procedures are needed but also preventive strategies and continuous education to avoid such adverse events.
How to create a safety culture
On the organizational side, a no blame culture is a fundamental prerequisite to learn from errors. However, “no blame” also has its limits in cases of recurrent violation of important safety rules, for example noncompliance with hand disinfection. This “just culture” will balance no blame against personal accountability of clinicians. Team formation under leadership by dedicated persons is central to create an atmosphere of trust and collaboration between different professional and occupational groups. Continuous education with permanent knowledge transfer reporting results of meetings or organizing a journal club is essential. For young doctors, individual skills workshops using high fidelity models, for instance by Vascular International School (www.vascular-international.org) or workshops for vascular access creation on human cadavers organized by the European Society of Vascular Surgery (www.esvs.org), are excellent options to learn technical steps where mistakes are corrected immediately by tutors without harming patients. Teaching in access creation may produce future surgeons who are more vigilant and creative in the field of vascular access surgery (AVF). Workplace assessments such as the objective structured assessment of technical skills (OSATS) or the direct observed procedural skills (DOPS) are good tools to give direct feedback to the trainees (15–17). They learn to decide, to question their own techniques, and it strengthens standardized procedures.
The implementation of a critical incident reporting system for healthcare professionals and regular morbidity and mortality conferences can help to establish a more transparent and instructive environment and to improve weak points in systems of dialysis care units.
What to do in the future
In the last years, patient safety became an important topic in different domains of medicine. Now, it is time to bring this to attention of all healthcare professionals dealing with vascular access asking what can be done to improve patient safety. Quite often, it is not a problem of knowledge but a reluctance of caregivers to implement the available evidence and to make a step towards better long-term results.
We should remember a paragraph by Neil McIntyre and Sir Karl Popper published in 1983, when they first reflected about new ethics, saying: To learn only from one's own mistakes would be a slow and painful process and unnecessary costly to one's patient. Experiences need to be pooled so that doctors may also learn from the errors of others. This requires a willingness to admit one has erred and to discuss the factors that may be responsible. It calls for a critical attitude to one's own work and that of others (18).
The Vascular Access Society (www.vascularaccesssociety.com) is willing to take responsibility in an initiative to make healthcare professionals more alert to all aspects of patient safety in the domain of dialysis access. We need to pay particular attention to careful treatment of this group of patients who are per se at a higher risk for adverse events. Healthcare research offers the possibility to study issues of patient safety not only by evaluating treatment concepts or new devices but also by studying the whole process of care delivery. Hopefully, our patients will be safer in the future and will appreciate our efforts.
Footnotes
Financial support: None.
Conflict of interest: M.K. Widmer: Convenor and Tutor of Vascular International Foundation and School, Switzerland. J. Schmidli: Executive Board, Convenor and Tutor of Vascular International Foundation and School, Switzerland. D. Schwappach and T.R. Wyss report no conflict of interest.