
Abstract
Objectives
Hemodialysis (HD) patients with superior vena cava (SVC) occlusion have limited access options. Femoral access is commonly employed but is associated with high complication rates. Hemodialysis Reliable Outflow (HeRO) catheters can be used in tunneled catheter-dependent (TCD) patients who have exhausted other access options. The HeRO graft bypasses occlusion and traverses stenosis with outflow directly into the central venous circulation. At our institution we have used the inside-out central venous access technique (IOCVA) to traverse an occluded vena cava for HeRO graft placement. We review our experience with this technique.
Methods
A retrospective chart review was conducted of patients with HeRO graft placement at our institution. All were dependent on a tunneled femoral dialysis catheter due to central venous occlusion (CVO). The IOCVA technique was used in each case. This technique was used as last resort for patients who had no other dialysis access option. Demographics, patency rates, complications, and mortality were recorded.
Results
A total of 11 HeRO grafts were placed in 11 patients from January 2012 to June 2013, with 100% technical success rate. Three grafts were ligated due to steal syndrome. Two grafts were lost due to thrombosis. Five of 11 patients experienced a 30-day complication. Three patients died within the follow-up period; however, none were directly related to the graft placement. Follow up range was 65-573 days; 5 of 11 grafts were used for dialysis at the end of the follow-up period. The 12-month patency rate was 30%.
Conclusions
HeRO grafts are one option for dialysis patients with CVO. There is, however, a high incidence of steal syndrome and other complications. These grafts should be offered as a final potential alternative to catheter dependence.
Introduction
As the life expectancy of dialysis patients increases, so do the challenges of maintaining dialysis access. Although the prevalence of arteriovenous fistula has been increasing, the placement of tunneled dialysis catheters (TDCs) still persists at high rates. Despite the ‘Fistula First Initiative’ (encouragement for the abandonment of catheters), the kidney disease statistics reported that 18% of the US dialysis population are dependent on a TDC (1). As a result, central vein stenosis remains a significant problem, especially in patients who have been catheter dependent for hemodialysis (HD) for prolonged periods. This challenge has led to efforts to address the sequela of central vein occlusion (CVOD). Most recently, the Hemodialysis Reliant Outflow (HeRO) graft (CryoLife, Kennesaw, GA, USA) was introduced in 2008. The HeRO device is an expanded polytetrafluoroethylene (ePTFE) graft attached to a nitinol-reinforced silicone outflow component, which is placed in a similar way to a central venous catheter, and with a counter incision in the shoulder area the two components are connected subcutaneously with a titanium connector. The distal end of the silicone outflow component is in the right atrium providing continuous flow into the central venous system without a graft-to-vein anastomosis. At our institution, a novel technique, the inside-out central venous access (IOCVA) technique was devised to cross central vein occlusions and has been used in conjunction with placement of HeRO graft.
While it is becoming increasingly popular, outcome literature is now emerging. A recent report by Wallace et al (2) questioned whether the industry supported data is representative of outcomes in patients with CVOD, as most of the initial data encompassed a large patient population with central venous stenosis. In this study, we review our experience with the IOCVA technique for HeRO graft placement in tunneled catheter-dependent (TCD) patients.
Methods
Approval for this study was obtained from our Institutional Review Board at the University of Kentucky. No competing interests were declared.
Database
A retrospective review of all patients who underwent HeRO graft placement at our institution between January 2012 and June 2013 was conducted. Demographics, etiology of renal failure, complications, and patency rates were recorded. All, but one, of the procedures were performed by the same team of two attending surgeons. All HeRO grafts were placed specifically for superior vena cava (SVC) occlusion and not stenosis. Our goal in all these patients who had exhausted all other access options was to remove the femoral dialysis catheters.
Procedure
Preoperative history and physical examinations were performed on each patient including assessment of the radial and brachial pulses. Preoperative wrist-brachial indices (WBI) were obtained in two of the patients. The HeRO graft was preferentially placed in the right arm because the course to the supraclavicular fossa and the SVC after using the IOCVA technique is less tortuous as compared to the left side. The left arm was used when the pulse was diminished on the right. All procedures were performed under general anesthesia. Placement was a two-step process for five patients; one to cross the SVC occlusion and the second to place the HeRO graft. In these five patients the occlusion was crossed and a TDC was left in place, the HeRO was placed 21-63 days later. After crossing the occlusion, a tunneled catheter was placed over a wire. These patients required immediate removal of the femoral catheter and a new dialysis access but had not completed a preoperative assessment for placement of the HeRO system or required antibiotic therapy and optimization of comorbid conditions. At the second stage, a wire was inserted through the tunneled catheter, the catheter was removed and over this wire the HeRO system was inserted. In six of the patients, the recanalization of the SVC and the placement of the HeRO system were performed on the same day in our hybrid operating room.
All patients were dependent on a tunneled femoral catheter for dialysis, had multiple failed accesses, and had SVC occlusion that was crossed with the IOCVA technique as previously described (3). Briefly, to cross the occluded SVC, the right common femoral vein was accessed using ultrasound guidance and a Seldinger technique. A 0.035 J-tipped guide wire was placed in the inferior vena cava (IVC) with a 5-Fr angled tip catheter over the wire. Wire and catheter are navigated to the atrium and to the confluence with the occluded SVC. The guide wire was then removed and hand injections of contrast were administered through the catheter under cineangiography. A 0.032-inch J-tipped guide wire was then placed at the level of the occlusion and the catheter was removed along with the 6-Fr hemostasis sheath. An 8-Fr SL0 sheath (SL0, Daig Inc™, St. Jude Medical™, St. Paul, MN, USA) was then placed with the tip next to the occlusion. A BRK transseptal needle (St. Jude Medical, St. Paul, MN, USA) was then placed in the dilator and a 0.018-inch steel core cut wire was placed inside the needle. Both the transseptal needle and steel wire were then directed from the IVC to the SVC, using lateral projections with angiography to ensure the pathway did not go through the atrial appendage. The needle and wire were then directed to the posterior side of the clavicle. The wire was then exteriorized and pulled through the skin of the supraclavicular fossa. The SL-0 dilator and BRK needle were exteriorized as well. Wire and BRK needle were then removed from the groin and replaced with a 0.032-inch J-tipped guide wire via the dilator. Over this, wire balloon dilation using a 10 mm balloon was performed along the tract of the occluded SVC extending to the right atrium. Then the HeRO peel-away sheath was placed from the supraclavicular fossa. In cases where a catheter is already present, access was obtained by placing a wire through the catheter. Once the peel-away sheath was in place, the rigid silicone-nitinol portion of the graft was directed down into the atrium. The ePTFE graft was then tunneled in a subcutaneous position along the lateral edge of the biceps muscle and connected to the nitinol outflow component. The ePTFE graft was then anastomosed end-to-side to the left or right brachial artery, patients were systemically heparinized prior to the clamping of the brachial artery. A more proximal artery was not used because the incidence of steal in general increases with more proximal inflow. Furthermore the configuration of the graft curvature was optimal with a brachial artery anastomosis.
Patients were dialyzed through their femoral tunneled catheter until the HeRO was ready for use. Those with a femoral line that needed to be immediately removed also had a tunneled Cannon catheter (Arrow International, Asheboro, NC) placed alongside the nitinol outflow component. This was done by inserting two 0.018 wires through the dilator and using a catheter over each one of them to exchange to stiffer 0.032 or 0.035 wire. The femoral line was removed before leaving the operating room. No specific anticoagulation/antiplatelet regimen was used and the patients remained on their preoperative medications.
Data Analysis Primary patency and survival were analyzed using the method of Kaplan-Meier.
Results
There were 11 HeRO grafts placed in 11 patients with SVC occlusion using the IOCVA technique between January 2012 and June 2013; six were male and five were female. Average age was 54.4 y (SD 16.4 y). Six were Caucasian and five were African American. Seven had diabetes. Eight had coronary artery disease. Etiologies for renal failure besides diabetes included lithium toxicity, focal segmental glomerulosclerosis (FSGS), polycystic kidney disease (PCKD), lupus, and hypertension. Technical success rate was 100%. Median follow-up was 218 days, and range was 65-573 days.
Three grafts were ligated for steal syndrome at 2, 35, and 97 days after placement. Before ligation, angiograms were performed in two grafts to evaluate for treatable stenosis. Angioplasty of one subclavian and one radial artery stenosis failed to adequately treat the ischemia. None were deemed appropriate for further revision. Two were diabetic and had previously undergone lower extremity amputation. None of these patients had a stent in the SVC.
Two grafts were lost due to thrombosis. Neither had a history of hypercoagulable disorder and both were on daily aspirin at the time of graft placement. One had 146 days of primary patency, 21 days of secondary patency, and occluded a third time 12 days after the second thrombectomy despite being on warfarin. The second had 60 days of primary patency and less than 1 day of secondary patency.
Seven of 11 (64%) patients were taking aspirin at the time of graft placement, one was taking aspirin and Coumadin, and four (36%) were taking no antiplatelet or anticoagulation therapy at the time of initial placement.
Failures due to steal syndrome and thrombosis were included in calculating the Kaplan-Meier curve for primary patency rates depicted in Figure 1. There were no cases of assisted primary patency.
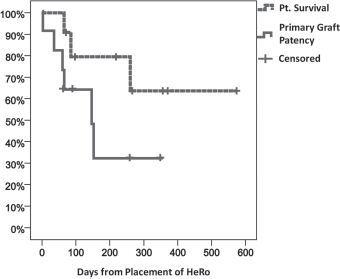
Kaplan-Meier curve of HeRO graft patency and patient survival.
Forty-five percent (5 of 11) patients had a complication within 30 days of HeRO placement. Complications in addition to steal syndrome included stroke (n = 1), pneumonia (n = 1), wound dehiscence (n = 1), pacemaker wire dislodgement (n = 1), bleeding requiring transfusion (n = 1), and acute psychosis (n = 1). The acute ischemic stroke was noted on MRI for a workup of left hand weakness. In retrospect, the left hand dysfunction was likely due to ischemia from steal syndrome. Pneumonia requiring hospitalization occurred in one patient with frequent lung infections and chronic pleural effusion. Wound dehiscence was noted in one patient during a follow-up appointment. There was no exposed graft, and tissue was re-approximated after washout in the operating room. The patient was given a 3-week course of intravenous antibiotics and is currently using the graft without complications.
There was one HeRO-associated episode of bacteremia in a patient with a co-existing TDC. Three patients died during the follow-up period, none directly related to HeRO graft placement. Two died after electing to stop dialysis, one after HeRO graft failure for thrombosis, and the other for failure secondary to steal syndrome. One died of complications from pneumonia after refusing intubation. At the end of the follow-up period, 5 of the 11 HeRO grafts were being used for dialysis. No patients were lost to follow up.
Discussion
The prevalence of patients needing renal replacement therapy has increased significantly during the last decades. Venous stenosis and occlusion frequently lead to access loss. In patients with an arteriovenous fistula or graft, CVOD can cause signs and symptoms of arm, neck or chest edema. Local trauma of a foreign body and turbulence of arterial flow in a venous system are proposed mechanisms which incite endothelial injury, thrombosis, and inflammation, resulting in stenosis and occlusion (4–7). CVOD is often silent until dialysis access in an ipsilateral limb incites high venous pressure, inadequate flow for dialysis, and thrombosis
Open surgical treatment of CVOD has traditionally been an innominate or axillary vein to right atrium bypass or an extra-anatomic bypass to the ipsilateral internal or external jugular vein or even a lower extremity vein (8–11). The extra-anatomic bypasses are not useful if the brachiocephahlic vein or SVC are occluded. The morbidity associated with a sternotomy or thoracotomy and six-month patency rates of these bypasses as low as 56% have resulted in infrequent use of these options (12).
In the era of endovascular therapy, angioplasty and stenting has become favored over open surgery for initial treatment of CVOD. Balloon angioplasty of central veins improves extremity edema and helps to maintain the access but the results tend to be short lived. Recurrence of the stenosis and occlusion is common (13–15). Primary patency for both bare metal and covered stents has been reported as 56% at 12 months (16, 17). Recurrent stenosis, need for repeated interventions, and inability to cross an occlusion are notable drawbacks to this approach.
Lower extremity access is another option when all upper extremity access options have been exhausted. Femoral loop grafts, in addition to some innovative techniques, such as the axillary to popliteal vein graft, have been well described. Risk of steal and high infection rates in the lower extremity deter many from these options (18).
The least desirable of all options is the TDC. Less effective dialysis, increased rates of thrombosis, higher rates of bacteremia, and greater mortality associated with use of a TDC are all well-known risks (19, 20). Thus our primary objective was to be able to remove the catheters from our patients. Our technique enabled us to place the HeRO catheter in all of our patients. The overall benefit was not as good as expected because of the high rate of ischemic and thrombotic complications.
The most common complication in our series was steal syndrome, necessitating graft ligation in 3 of 11 (27%) patients. Two of these patients were diabetic males with a history of peripheral vascular disease (PVD) and bilateral lower extremity amputation. Their grafts were ligated 35 and 153 days, respectively, after placement. Each had digit necrosis. The third patient was a non-diabetic 78-year-old female with a history of PVD. Her graft was ligated on postoperative day 1 after angioplasty of a subclavian stenosis failed to resolve her severe hand pain and ischemia. We did not feel that they were candidates for distal revision with interval ligation (DRIL) or revision using distal inflow (RUDI) due to variable factors, including multiple comorbidities, calcified arteries, diseased runoff, and severity of tissue loss.
During the time span that the grafts were placed, it became gradually apparent that steal syndrome was a significant risk. In each of the patients with ischemic complications, the graft was placed even if the preoperative pulse exam revealed diminished pulses, because there was no alternative other than dependence on a TDC. In our practice we now routinely include arm segmental pressure studies as part of the preoperative work-up. They were normal in the two performed in this series. Nevertheless, we do not consider an abnormal wrist-brachial index (WBI) a contraindication to placement of a HeRO system in a patient who has exhausted all other dialysis access options and is catheter dependent. At this point we do not have an objective segmental pressure threshold that can predict steal syndrome in these patients. We do however discuss this likely complication extensively with the patient as well as the potential for the need for revision of ligation of the graft if hand ischemia develops. Techniques have been described to address steal syndrome, the use of these techniques was considered but we felt that our patients were not suitable candidates for a revision procedure because of poor outflow, heavily diseased calcified vasculature and severity of ischemia.
The largest published series of HeRO graft outcomes reported 2 out of 164 (1.4%) patients with steal syndrome necessitated graft ligation (21). In that retrospective review, criteria for graft placement was either central vein stenosis or CVOD. Our population was more similar to that recently reported by Wallace et al (2) in which 4 of their 19 patients (24%) required HeRO ligation secondary to steal syndrome. Their population, as well as ours, had CVOD as a prerequisite for HeRO placement. At our institution, central vein stenosis is treated with angioplasty and stenting rather than HeRO graft placement, only patients who have failed this option are considered for HeRO graft placement.
Primary patency in our series was 30% at 1 year. This is lower than initial reports of 49% by Gage et al (21) and similar to Wallace et al's reported 20% patency (2). Two grafts in our series were lost due to repeated thrombosis. Secondary patency was short lived in both.
Patient selection may contribute to the difference between initial literature and recent reports. In the majority of the published literature, HeRO grafts were not placed for CVOD. As summarized by Nassar in 2010 (22), the initial trials for the HeRO graft did not require patients to have central vein stenosis prior to placement. An illustration of the difference in outcome that CVOD may have is the reported 56-month primary patency rate of the very first HeRO graft that was placed in 2004. That patient had no prior dialysis access and no history of CVOD (22).
Our technical success rate for placing the HeRO across SVC occlusion was 100%. This same technique has been used at our institution to place infusion catheters for patients with CVOD, thus avoiding placement of a femoral line.
The IOCVA technique also permitted placement of a second TDC at the time of HeRO placement in order to remove the pre-existing tunneled femoral catheter. This is an important component in preventing catheter-associated bacteremia and HeRO graft infection. In the initial published series of 38 HeRO grafts, Gage et al (21) reported 17 bacteremic events. All occurred during the bridging period with a TDC, and 59% of the TDCs were placed in the femoral vein. It is also feasible to place another tunneled catheter over a wire after removing the nitinol component in cases where the HeRO graft fails due to steal or thrombosis and avoid the femoral location.
Conclusion
The inside-out technique is an excellent option for successful recanalization of central venous occlusion in catheter-dependent end-stage renal disease patients. The HeRO device is an acceptable option for access in the dialysis patient with CVOD and it may be the only alternative to catheter dependence. Steal syndrome is a significant risk. Patients should be counseled accordingly and careful consideration should be given to those with PVD since they are more likely to develop this complication.
Footnotes
Financial support: None.
Conflicts of interest: None.