
Abstract
Purpose
Vein punctures are performed daily to sample blood. Ultrasound (US) offers an alternative to the blind landmark technique for difficult vascular access. A challenge for this procedure is the presence of US gel in the puncture area. We present a technique for US-guided puncture from extremity veins not palpable or visible to the human eye, while keeping the puncture area dry and gel-free.
Methods
Ten healthy volunteers underwent two US-guided vein punctures from veins that were neither palpable nor visible. One was drawn from an antebrachial vein and another from a brachial vein. A sterile barrier drape was made from a commercially available dressing and a piece of transparent sterile plastic. The barrier drape consists of an adhesive part placed on the skin designed for sonography and a free transparent flap constituting the barrier between the unsterile sonographic site and the sterile gel-free puncture site.
Results
The success rate for vein puncture was 100% in both locations. A total of 22 skin punctures were performed (11 antebrachial and 11 brachial). Gain output was increased 7% (4-12%), and 8% (4-15%), respectively, to compensate for attenuation of the US signal due to the drape. Alignment of the centre of the transducer with the long-axis of the target vein during the procedure was reported as a challenge.
Conclusions
US-guided blood sampling from a brachial and antebrachial vein was possible with a 100% success rate, while ensuring a dry and gel-free venipuncture area on one side and the transducer on the other side of a sterile barrier.
Introduction
Peripheral vein punctures are performed daily at hospitals worldwide to sample blood. The traditional blind anatomical landmark technique is often inadequate to obtain venous access in obese, chronically ill or hypovolaemic patients, but difficulties have also been reported in healthy individuals (1–2–3).
Ultrasound (US) offers an alternative to the blind landmark technique in patients with difficult peripheral vascular access. Several studies on peripheral vascular cannulation have demonstrated that US improves success rate, requires fewer attempts, reduces overall time and increases patient satisfaction (2, 4–5–6–7).
During US procedures, gel is required to ensure acoustic coupling between the skin and the transducer. The overall key to successful ultrasound-guided vein puncture is to get full control of the needle tip as early as possible during the procedure, ideally already 0.5-1 mm after skin puncture. Otherwise unintended vessel or tissue damage may have already occurred before tracking of the needle tip towards the target vessel has started. From an anatomical and a geometrical consideration and the fact that the ultrasound image is very narrow compared to the width of the transducer, it is evident that the needle has to be very close to the transducer and actually almost touching and sliding the transducer at the moment of skin perforation. Otherwise the needle tip will be located deep into the tissue when the needle tip is identified on the screen.
Commonly, a sterile wrap around the ultrasound transducer and sterile gel between the skin and the wrap is used; however, this technique involves gel in the puncture area and contamination of the needle with gel is unavoidable under these circumstances. Two recently published papers conclude that gel is a source of contamination that needs to be addressed (8, 9). Different solutions have been attempted, but the important issue of avoiding gel or other liquids in the puncture area has never been solved. In our research laboratory, pilot studies in ultrasound phantoms using different types of adhesive drapes, provided good visualisation of the needle tip and artificial vessels. Based on these findings, we have developed a drape made from a commercially available dressing and a piece of plastic that serves as a non-sticky sterile barrier allowing ultrasound-guided blood sampling from a gel-free puncture area.
The aim of this study was to introduce and demonstrate a new ultrasound-guided technique for blood sampling that works without gel in the puncture area. All target veins were not palpable or visible to the human eye.
Materials and methods
Study subjects
After approval by the Central Denmark Region Committee of Biomedical Research Ethics (case no. 1-10-72-589-12) and a written informed consent had been obtained, a sample of ten healthy volunteers was included. The volunteers were recruited through advertisement on a billboard at Health, Aarhus University and the local Red Cross First Aid group. Exclusion criteria were: age below 18 or above 70 years of age, use of anticoagulants, chronic illnesses requiring frequent blood sampling, and cardiac or vascular diseases. The first ten volunteers who responded to the advertisement, met inclusion criteria, and were able to participate on one of the two trial dates, were included. Each participant received a compensatory fee of EUR27.00. The study took place at Aarhus University Hospital, Denmark.
Ultrasound equipment
A Flex Focus 400 Anaesthesia ultrasonography system with an 18-6 MHz linear transducer (BK-medical, Herlev, Denmark) was used for all procedures.
To assess anatomy and identify two target vessels a pre-scan of the sampled arm was performed. The choice of right or left arm was arbitrary.
Initially two veins, one in the antebrachial area no more than ten centimetres distal to the antecubital fold, and one vein in the brachial area no more than ten centimetres proximal to the antecubital fold, were visualised by US in a short axis (SAX) view. Veins not visible or palpable were chosen, in order to simulate situations with invisible veins.
The veins were identified by compressibility with light transducer pressure, and differentiated from arteries by absence of visible pulsation.
Ultrasound puncture technique
A modified out-of-plane approach, Dynamic Needle Tip Positioning (DNTP), earlier described in details (10) was used during the procedures. Briefly, the vessel is displayed in a SAX view as a circular anechoic structure, while the needle tip appears as a hyperechoic dot when it intersects the US beam. By successively moving the transducer and the needle away in intermittent small steps, the needle tip can be tracked more and more proximal towards the vessel.
Sterile barrier drape
The sterile barrier drape used for the vein punctures was made from a commercial dressing (3M™, St. Paul, MN) and a piece of transparent sterile plastic. The barrier drape has an adhesive part attached to the skin that constitutes an unsterile field where ultrasonography is performed. The other part of the drape presents a free flap serving as a barrier between the unsterile adhesive part on one side, and a sterile gel-free skin puncture area on the other side (Fig. 1). The piece of transparent sterile plastic was attached in order to cover the sticky part of the free flap.
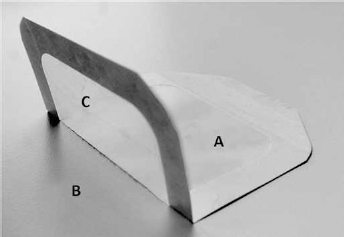
The barrier drape is made from commercially available Tegaderm (3M™, St. Paul, MN) and a transparent piece of sterile plastic. (
Blood sampling
During the initial sonography identifying appropriate target veins, the sonographic image was optimised by adjusting depth, gain and focus settings. During the venipuncture procedure, only gain was adjusted to compensate for the US attenuation caused by the adhesive part of the barrier drape. The first blood sample was drawn from the selected antebrachial vein and the second from the brachial vein. For the antebrachial vein puncture, a 22-gauge multi-sample needle connected with a single-use holder (Venoject®, Terumo Europe N.V, Belgium), was used to test the efficacy of the procedure for routine blood sampling. Successful venipuncture was defined as complete filling of a blood collection container (Venoject®, Terumo Europe N.V, Belgium). A tourniquet was tightened around the upper arm. The barrier drape was placed just proximal to the puncture area, allowing needle insertion 1-2 mm distal to the free flap of the drape. The skin was disinfected with standard aseptic technique using two swaps containing 82% alcohol/0.5% chlorhexidine. The needle was inserted by an US-guided DNTP technique until successful blood withdrawal. The needle was removed immediately afterwards and a cotton wad was used to compress the needle puncture site. The venipuncture was repeated in the selected brachial vein. Here successful vein puncture was defined as rapid filling of the tube connected to the blood bag. The entire procedure is summarised in Figure 2. Phlebotomy was performed by a consultant anaesthesiologist (ES) with two years of experience with the DNTP technique. All venipuncture procedures were video recorded for detailed offline analysis.
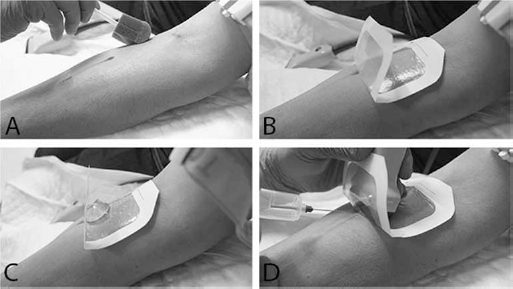
US-guided blood sampling with the barrier drape used in this study. (
Data analysis
A single examiner performed data analysis.
The following endpoints were recorded:
Number of successful vein punctures;
Vascular access time from skin puncture to needle tip placed deep inside the target vessel;
Number of skin punctures required for successful blood sampling;
Difference in gain setting, with and without barrier drape;
Complications, including transvascular penetration, gel in the puncture site and challenges with the technique;
Cross-sectional vascular diameter and skin-vessel-distance using the calibre tool of the US system.
Statistics
Continuous variables are presented as median (range). Categorical variables are presented as number of subjects (percentage).
Results
The median age was 25.5 years (21-34 years). Seventy percent were male. The success rate for venipuncture was 100%. A total of 22 skin punctures were performed (11 antebrachial and 11 brachial). The sterile barrier drape kept gel out of the puncture site and the gel was restricted to the adhesive unsterile part for the drape in all 22 venous cannulations. Vascular access time was 68 sec (48-115 sec) for antebrachial puncture and 37.5 sec (20-114 sec) for brachial puncture. Gain output was increased by 7% (4-12%) and 8% (4-15%), respectively. No transvascular penetrations were visually identified. Alignment of the centre of the transducer with the long-axis of the target vein during the procedure was reported as a challenge.
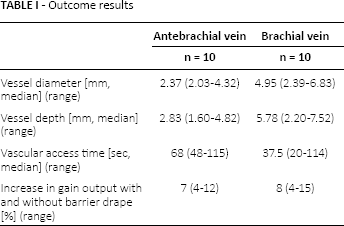
Anatomical data are presented in Table I.
Outcome results
Discussion
The present study shows that US-guided blood sampling can be performed without any gel applied at the disinfected puncture field by the use of a simple barrier drape. In addition, US-guided blood sampling is feasible from veins not palpable or visible to the human eye, with a success rate of 100%. This allowed for continuous visualising of the target vessel, allowing the needle tip to be followed accurately into the target vessel.
When taking blood samples, it is crucial to keep the puncture field dry and clean, to avoid any kind of blood sample contamination (11, 12). Different solutions have been recommended to overcome this problem during US-guided procedures, such as a sterile cover, gloves or adhesive dressings on the transducer. However, none of these methods have worked without gel, leaving the unsolved problem of possible gel contamination in the field. We here present a new and quick technique for blood sampling that works without gel or any other liquids in the puncture area.
Although the average gain output was increased in order to optimise the sonographic image, the overall image quality was ample, and yielded a 100% success rate without any technical hitches. However, the free flap of the barrier drape was not 100% transparent, which hampered the alignment of the centre of the transducer with the long-axis of the target vessel. This was reported as the main reason why one volunteer had two skin punctures in order to obtain an antebrachial blood sample. A solution could be to use an optimised transparent prototype with centre-line markings on the transducer and the US screen to facilitate alignment. Several US manufacturers already offer these features.
Pre-scanning of the puncture area made it possible to evaluate the anatomic relationship of nerves and vessels, and thus to preselect the most appropriate target vessel and puncture site. It is particularly important to make sure that the transducer can be moved freely, to ensure tracking of the needle tip into the vessel to allow unimpeded blood withdrawal.
Clinical implications
This new technique allows easy and quickly uncontaminated evacuation of blood with US-guidance in veins not palpable or visible to the human eye. Thus, the technique can potentially reduce multiple attempts in difficult clinical cases. Likewise, potential hitherto abandoned blood donors can be re-evaluated for their availability. Phlebotomists are no longer restricted to the median cubital vein for venous access, but can choose any appropriate vein on the extremity when the technique has been learnt.
Limitations
Only one physician performed all the US-guided blood collections in the study, and the results may not be directly extrapolated to other physicians. However, several studies have demonstrated that US-guided vascular access has a steep learning curve (13–14–15). Further studies comparing the US-guided technique with the traditional palpation technique and investigating patient satisfaction and pain scores could be interesting.
Conclusion
Easy and quick US-guided blood sampling was possible, with a 100% success rate in deep veins neither visible nor palpable, while ensuring a gel-free venipuncture area on one side and the transducer on the other side of a sterile barrier. No complications were identified. Further research is needed to fully evaluate the use of US-guided blood sampling for patients with difficult venous access, and to test whether this new technique can be implemented in the community of the phlebotomist.
Footnotes
Financial support: ST has received funding from the Danish Cancer Society and the Lundbeck Foundation covering salary. The authors do not have a financial relationship with the organisations that sponsored the research.
Conflict of interest: TFB, LK and ES have a patent pending on a commercial device to be used for the procedure (European Patent Office, Munich, Germany, patent number P18287PCEP). ES has given lectures for BK-Medical and received fees. ST and NG have no conflict of interests to declare.