
Abstract
A persistent left superior vena cava (PLSVC) is a rare, under-recognized congenital anomaly. The PLSVC is incidentally discovered during central venous access procedures when access is obtained from the left internal jugular vein. The vast majority of PLSVCs drain into the right atrium; however, it is critical to recognize a PLSVC that drains into the left atrium as it can predispose to systemic dispersion of emboli through bypassing the lungs. Additionally, PLSVC catheterization has also been previously reported to be associated with cardiac dysrhythmias, venous stenosis, coronary sinus thrombosis, cardiac tamponade, and cardiac arrest. This case review presents three cases which illustrate the viability and safety of a PLSVC for long-term central venous access in the setting of chemotherapy and hemodialysis. Ascertaining the drainage pattern of a PLSVC with venogram, echocardiography, computed tomography is paramount prior to long-term catheterization.
Introduction
Central venous access is a mainstay of modern medical therapy, providing a means for efficient volume exchange (e.g., hemodialysis, plasmapheresis), large-volume resuscitation (e.g., transfusion, rapid fluid bolus), and safe administration of agents poorly tolerated in low-flow peripheral venous circulation (e.g., vasoactive medications, caustic substances, total parenteral nutrition). It is routinely performed in both inpatient and outpatient facilities, as well as in settings that vary from elective to urgent to emergency.
Despite its ubiquity, central venous catheterization is associated with increased patient morbidity, infection, and failure rates as compared to other forms of vascular access. Various large-scale initiatives designed to improve these outcomes have resulted in only modest improvement. For example, the UK's payment of surgeons based upon outcomes rather than quantity was associated with only a 16.7% increase in 1-year survival among hemodialysis patients over a 14-year period (63.9% in 1997 vs. 80.6% in 2011), despite concomitant advances in other areas of medicine (1).
As the medical community strives for improved outcomes, the proceduralist skilled in central venous access must possess a thorough knowledge of not only normal venous anatomy, but also of relevant acquired and congenital anatomic variation. One such variant, persistent left superior vena cava (PLSVC) exists in multiple forms with distinct implications upon the safety of central venous catheterization. Three cases of central venous access in patients with PLSVC are presented below, followed by a discussion of embryologic development and key clinical considerations.
Case 1
A 37-year-old female with history of non-Hodgkin's lymphoma required central venous access for chemotherapy. The patient's right internal jugular vein was occluded. Consequently, a chemotherapy port was placed via left internal jugular vein approach with the catheter terminating in a PLSVC, demonstrated by intra-procedural venography to drain into the right atrium (Figs. 1-3). The patient tolerated the procedure without complication and subsequently underwent 8 months of uneventful chemotherapy administration.

Intra-procedural venogram demonstrates left-sided superior vena cava.
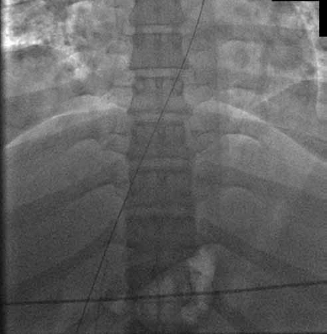
Guidewire into the inferior vena cava confirms that the persistent left superior vena cava terminates in the right atrium.
Catheter tip terminating in the distal persistent left superior vena cava.
Case 2
A 63-year-old female with history of renal insufficiency required central venous access for hemodialysis. The patient had a contraindication to right internal jugular vein catheterization. Consequently, a tunneled hemodialysis catheter was placed via left internal jugular vein approach, terminating in a PLSVC, demonstrated by intra-procedural venography to drain into the right atrium (Figs. 4-6). The patient tolerated the procedure without complication and subsequently underwent 9 months of uneventful hemodialysis.
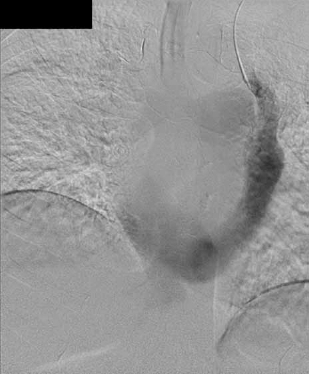
Venogram demonstrates persistent left superior vena cava draining into the right atrium.
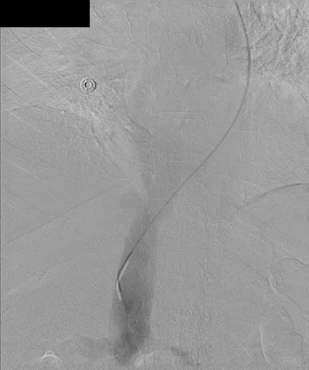
Guidewire is advanced from the persistent left superior vena cava into the right atrium then into the inferior vena cava.
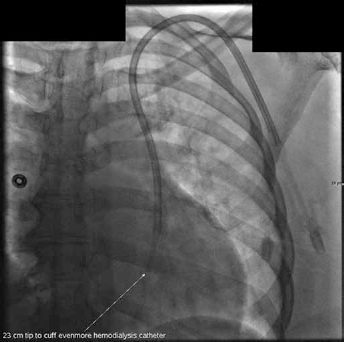
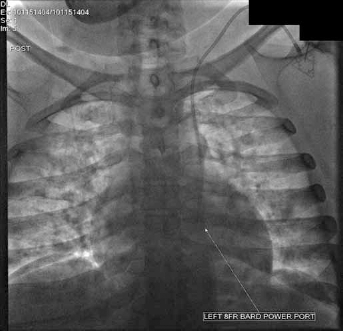
Hemodialysis catheter placed with tip terminating in the distal persistent left superior vena cava.
Case 3
A 58-year-old male with history of infected leads from a right-sided automatic implantable cardioverter-defibrillator automatic implantable cardioverter-defibrillator (AICD) required central venous access for outpatient intravenous antibiotic therapy. A tunneled central venous catheter was placed via left internal jugular vein approach terminating in a PLSVC, demonstrated by pre-procedural contrast-enhanced CT to drain into the right atrium (Figs. 7, 8). The patient tolerated the procedure without immediate complication and subsequently underwent 6 weeks of uneventful antibiotic administration.

Computed tomography angiography of the chest shows contrast draining to the persistent left superior vena cava and then into the right atrium.
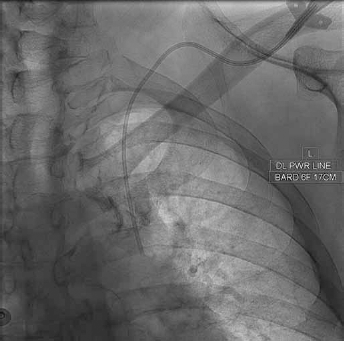
Peripherally inserted central catheter terminating into the persistent left superior vena cava.
Discussion
Persistent left superior vena cava (PLSVC) is an extremely uncommon congenital anomaly with a reported incidence of 0.3% in normal healthy individuals and as high as 4.5% in the patient population with congenital heart disease (2, 3). During the eighth week of embryologic development, a large venous anastomosis (the future left brachiocephalic vein) develops between the left and right precardinal veins. Above this anastomosis, the precardinal veins become the internal jugular veins. Below this anastomosis, the right precardinal and right common cardinal veins become the superior vena cava (SVC); the left precardinal vein normally regresses with only a short segment persisting as the left superior intercostal vein, while the left common cardinal vein forms the coronary sinus venosus. PLSVC arises from failure of the left precardinal vein to regress (4).
PLSVC typically descends lateral to the aortic arch and anterior to the pulmonary hilum, enters the pericardium in the posterior atrioventricular groove, and drains into the coronary sinus (5). Four anatomic variants of PLSVC have been described. The first variant results in bilateral SVCs and an underdeveloped left brachiocephalic vein. A second variant has a small vessel bridging the two SVCs, known as the left Cuvier duct. The third variant is the most common and is characterized by the brachiocephalic vein connecting the two SVCs. Atrophy of the right SVC with persistent left SVC is the fourth variant (6).
In addition to its rarity, PLSVC is likely also under recognized. First, PLSVC itself does not constitute a hemodynamically significant phenomenon and is generally only symptomatic if it drains into the left atrium (right-to-left shunting) (3, 7, 8) or if an enlarged coronary sinus causes conduction abnormalities (resulting in cardiac arrhythmia) (9). Second, the default tendency of most operators is to attempt central venous access from the shorter, straighter, right internal jugular or right subclavian approach; given that the preponderance of PLSVC occurs concomitantly with a viable right-sided SVC, it stands to reason that most cases remain undiscovered (10).
PLSVC most commonly drains into the right atrium through the coronary sinus (80%-90%), only infrequently draining into the left atrium (8%) (11). However, it is critically important to recognize PLSVC draining into the left atrium, as introduced gas or thrombus secondary to catheterization may embolize into the peripheral circulation (12). Other significant clinical consequences reported in association with PLSVC catheterization include cardiac dysrhythmia, venous stenosis, coronary sinus thrombosis, hypotension, cardiac tamponade, and cardiac arrest from coronary sinus irritation (13-16). Finally, misinterpretation of diagnostic imaging in patients with PLSVC catheterization may lead to the incorrect diagnosis of catheter malposition, which may result in unnecessary subsequent intervention, contrast administration, and/or radiation exposure, as well as delaying initiation of necessary therapy, such as hemodialysis or intravenous administration of medication.
As presented in these cases and as other authors have previously reported, short-term catheterization of the PLSVC variant with right atrial drainage is safe and effective (7, 17, 18). Powell et al concluded that central venous catheterization via unconventional approaches (collateral veins, occluded veins, translumbar inferior vena cava, transhepatic veins) did not result in poorer complication rates, dialysis flow rates, catheter-related bacteremia, or longevity of access when compared with conventional methods (1).
Venography is the gold standard to delineate patterns of central venous return and, when anomalous vascular anatomy is recognized intra-procedurally, should be utilized to confirm right atrial drainage prior to PLSVC catheterization; however, several complementary, noninvasive investigations may augment or supplant venography in contrast-intolerant patients or when an anomalous catheter course is recognized post-procedurally. Physical examination may reveal left external jugular vein distention and/or heart murmur (3, 19). A small, distinct area of mediastinal widening superior to the left margin of the aortic arch has been reported on conventional chest radiography (3). Computed tomography can demonstrate venous drainage, accurately depict PLSVC size, and characterize contralateral central venous structures, as well as confirm catheter course in cases of suspected incidental PLSVC catheterization. Blood gas analysis of catheter aspirate can differentiate arterial from venous catheterization. A dilated coronary sinus on echocardiogram should raise suspicion of a PLSVC and prompt investigation into the pattern of central venous return and presence of right-to-left shunting (3). Electrocardiography can assess for cardiac dysrhythmia following PLSVC catheterization (20, 21).
Conclusion
Short- or intermediate-term PLSVC catheterization is safe and effective in select patients in whom conventional SVC catheterization is infeasible, provided that venous return is to the right atrium. When PLSVC is recognized intra-procedurally, venography is suggested to delineate the pattern of central venous return prior to catheterization; when suspected post-procedurally, various noninvasive investigations can confirm catheter location within a PLSVC and/or assess its suitability for continued catheterization. Further research is required to establish feasibility of long-term PLSVC catheterization and caution should be exercised when administering potentially harmful agents (e.g., those associated with cardiotoxicity) via unconventional access.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.