P-001 17-YEAR EXPERIENCE OF IMPLANTABLE VENOUS PORT USAGE AT CHILDREN AND ADOLESCENCE: EXPERIENCE OF 2 RUSSIAN INSTITUTES
M.Y. Rykov1, Y.V. Buydenok1, V.G. Polyakov1
1Institute of Pediatric Oncology and Hematology N.N. Blokhin Moscow, Russia;
1Institute of Clinical Oncology, Moscow, Russia
Introduction: Intravenous injection is an integral part of the treatment of cancer and many congenital diseases: mucopolysaccharidosis, cystic fibrosis, glycogenosis. Implantable venous ports are the best long-term access to the venous system.
Methods: 3256 patients (3 months. - 87 years) underwent implantation of venous ports: since 1998 2921 patients in the Institute of Clinical Oncology and since 2008 278 patients in the Institute of Pediatric Oncology and Hematology. To access the superior vena cava in 3127 (96%) an internal jugular was punctured, in 129 (4%) a subclavian vena was used. An ultrasound marking of veins came before the puncturing. Using intraoperative fluoroscopic for positioning of distal end of the catheter to the superior vena cava the ports were implanted in 2987 (91.7%) patients, in 269 (8.3) for this purpose an endocardial ECG was made.
Results: Thromboses of port systems was observed in 75 (2.3%) patients, catheter associated bloodstream infections - in 5 (0.15%), pneumothorax - in 5 (0.15%). Migration of a catheter wire to the internal jugular against bloodstream was observed in 138 (4.3%) to the subclavian vein in 92 (2.8%) to the internal jugular vena on the opposite side - in 11 (0.3%). From the first attempt we managed to puncture IJV in 3248 (99.7%), to catheterize in 2915 (89.5%).
Conclusions: The use of ultrasonic marking permits the avoidance of injury to the adjacent anatomical structures and the reduction of the duration of the surgery. The use of an X-ray scanner during the positioning of the port catheter prevents its migration into the cervical veins and enables to place a tip of the catheter into the v. cava superior directly above a right atrium entry site.
P-002 CATHETER-RELATED INFECTIONS AND THROMBOSIS IN CHILDREN WITH CANCER
M.Y. Rykov, V.G. Polyakov
Institute of Pediatric Oncology and Hematology N.N. Blokhin, Moscow, Russia
Background: A long-term use and operation of venous port systems, which are essential in the treatment of child cancer patients, is only possible with providing appropriate maintenance and care.
Materials and methods: From July 2010 to September 2015 we observed 217 child cancer patients aged from 6 months to 17 years. 97 underwent the implantation of subcutaneous venous port-systems, in 120 - traditional subclavian catheters we introduced. The following criteria were evaluated: local manifestations of infection, development of catheter-related bloodstream infections and cases of catheter thrombosis. Of the patients implanted with subcutaneous venous ports, periportal tissue infection was noted in 3 cases (3.09%). No catheter-related bloodstream infections were noted. Port catheter thrombosis was observed in 7 cases (7.2%). In patients with traditional subclavian catheters, puncture site infection was noted in 73 cases (60.8%). The development of catheter-related bloodstream infections was noted in 15 cases (12.5%). Catheter thrombosis was observed in 44 cases (36.6%). In cases of port thrombosis, we injected the system with a 25,000 IU dose of Urokinase with an exposure of 15 minutes. The treatment of 32 cases (72.7%) of the 44 occurrences of subclavian catheter thrombosis necessitated replacement, together with the associated need for general anesthesia. To seal the catheter between courses of treatment, we used heparin or a solution containing cyclotaurolidin (when using which no catheter-related bloodstream infections were noted).
Results: All venous ports have worked satisfactorily following implantation. All cases of thrombosis of venous port systems were successfully treated.
Conclusions: The use of a cyclotaurolidin solution to seal the venous system in the intervals between treatments prevents infection. The treatment of catheter-related infections is better effected by a combination of cyclotaurolidin and urokinase, which provides lysis of the microtrombs serving as a source of bacteria in both the catheter and port chamber.
P-003 PREPARING FOR THE NEXT PANDEMIC: LESSONS LEARNED FROM EBOLA VIRUS DISEASE FOR VASCULAR ACCESS
J.H. Garrett
PDI, Atlanta, USA
Ebola Virus Disease recently caused a global outbreak and worldwide concern for all healthcare providers and patients. Ebola, however, is just the most recent example of the potential threat for pandemic infectious diseases having a global impact on the delivery of healthcare services globally. Previously, bloodborne pathogens were the primary concern for occupational risk and exposure, however this recent outbreak has highlighted the potential dangers to Vascular Access Clinicians.
During the crisis, there were many lessons learned, but most notably the importance of ongoing training about Personal Protective Equipment and its appropriate use in order to mitigate risk for occupational exposure for healthcare providers. Given that patients impacted by emergent infectious diseases will require vascular access therapy and support, we must adequately train, prepare, and protect Vascular Access clinicians against occupational exposures from infectioud diseases. This session will focus on the revised World Health Organization and Centers for Disease Control and Prevention evidence based recommendations for use of personal protective equipment, pandemic preparedness, and the role of collaboration across disciplines to protect the patient, the vascular access clinician, and the clinical environment of care.
P-005 THE PATIENTS EXPERIENCE OF LONG TERM VASCULAR ACCESS
L.J. Kelly
University of the West of Scotland, Glasgow, UK
Introduction: Clinicians select Central Venous Access Devices (CVAD) based on issues such as: type of therapy; duration of treatment; device availability (Cowley, 2004; Cook, 2007; Ludemank, 2007). Information about advantages and disadvantages of devices from a patient view point is sparse but needs to be considered to ensure patient centred care (NHS, 2012). Obtaining the views of patients who have had a device in place should place clinicians in a better position to support future patients with a deeper; more sophisticated understanding the feelings and experiences of the patient. There are limited studies that have explored the perceptions or quality of life of patients who have received treatment through long term vascular access device. This study is part of a PhD and aims to gather information to gain a deep insight into the experiences and perceptions of patients living with a long term CVADs.
Methods: Qualitative study using one to one in-depth interviews. Purposeful sampling. Sample size 11. Patients had either a PiCC, tunnelled cuffed catheter or totally implanted port inserted.
Results: All patients accepted their devices; they preferred their devices to the others they were aware of. The patients got used to them almost immediately and soon saw them as ‘part of them’. They all found it difficult to find any negatives about their devices. The devices did not seem to affect their activities of daily living.
Discussion: One issue described was the lack of competence and competence of some practitioners out with specialist areas. Patients would like all practitioners to be able to confidently deal with the device when they attend for blood samples or dressings.
Conclusions: As more patients receive long term devices, we should ensure that training and education in the use, care and maintenance of CVADs is introduced into both nurse and medical staff training.
P-006 NOT ACCEPTABLE: POST-INSERTION COMPLICATIONS OF PAEDIATRIC CENTRAL VENOUS ACCESS DEVICES
A.J. Ullman, N. Marsh, G. Mihala, M. Cooke, C.M. Rickard
Menzies Health Institute Queensland, Brisbane, Australia
Central venous access devices (CVADs) are a necessary aspect of paediatric care, however their failure and complication results in interrupted treatment, morbidity and mortality for the child, and the insertion of a new CVAD. There is a range of CVADs available, which healthcare professionals elect to insert on the basis of the predicted duration of clinical necessity, risk of adverse outcomes, treatment requirements, frequency of usage, and vein availability.
A systematic review and meta-analysis of cohort studies which examined the incidence of CVAD failure and post-insertion complications across CVAD types in paediatrics was undertaken. CVAD failure was defined as CVAD loss of function prior to completion of necessary treatment, and post-insertion complications of CVAD-associated bloodstream infection, local infection/phlebitis, dislodgement, occlusion, thrombosis and breakage.
Searches of electronic databases were undertaken in January 2015. Seventy-four cohort studies were included with mixed quality reporting and method. Overall, 25% of CVADs failued prior to completion of therapy (95% CI 20.9-29.2%) at a rate of 1.97 per 1,000 catheter days (95% CI 1.71-2.23). The failure per CVAD type was highest proportionally in haemodialysis catheters (46.4%, 95% CI 29.6-63.6%); and per 1,000 catheter days in umbilical catheter (28.6 per 1,000 catheter days, 95% CI 17.4-39.8). Totally implanted devices had the lowest rate of failure per 1,000 catheter days (0.15, 95% CI 0.09-0.20).
Over 10% (95% CI 8.9-11.6%) of paediatric CVADs developed a CVAD-associated BSI with a rate of 1.6 per 1,000 catheter days (95% CI 1.4-1.9). The highest rates of CVAD-associated BSI were evident in each of the CVAD types, however there was inadequate data to provide estimates of comparative risks for non-tunnelled CVADs.
CVAD failure and complications in paediatrics is a significant burden on the healthcare system internationally.
P-007 EXTRAVASATIONS DUE TO THE INCOMPLETE FRACTURE OF GROSHONG SILICONE CATHETER OF POWER PORT-A-CATH AFTER CT EXAMINATION
J. Charvat, K. Lisova, O. Hloch, J. Masopust
Faculty Hospital, Prague, Czech Republic
Introduction: Extravasations is serious complication during chemotherapy treatment in cancer patients when using intravenous port. The most frequently this complication is due to the incorrect application to the port but occasionally it may be consequence of catheter rupture.
Case description: 34 years old patients with colon adenocarcinoma was indicated after its surgical removal to chemotherapy - Folfox and Avastin. 24th of July 2013 power port-a-cath with Groshong silicone catheter 6.6 F was implanted using the right internal jugular vein approach. Two years later after CT examination using power port the extravasations has appeared below the right clavicle bone relatively far away of port body. The angiography examination revealed sharp angle of catheter in the supraclavicular area and leak of contrast at the site of the catheter entrance into the right internal jugular vein. The extraction of port-a-cath was indicated. After surgical removal 2 holes - incomplete fracture - were detected on the catheter.
Conclusions: Extravasations due to incomplete catheter fracture may appear after CT examination using Groshong silicone power port-a-cath.
P-008 THROMBOTIC COMPLICATIONS OF MIDLINE CATHETER
J. Charvat, V. Zauska, K. Lisova, K. Zemanova
Faculty hospital, Prague, Czech Republic
Introduction: Midline catheter insertion into deep arm veins can be complicated with the formation of upper limb thrombosis. The aim of the study was to evaluate the rate of the symptomatic and asymptomatic upper limb thrombosis and the influence of some clinical parameters on its development.
Methods: Out of 360 midline catheters (4F) inserted since January till October 2015 the randomly selected subgroup of patients had ultrasonography examination of upper limb 6 to 10 days after procedure. The presence of thrombotic changes was evaluated and the significance of age, gender, the site insertion and preventive dose of low molecular heparin were analyzed. The size of the vein at site where midline was inserted had to be at least 4 mm.
Results: The subgroup formed 46 patients (12.7% out of 360) 30 women and 15 men. The age of patients was 38 to 96 years, median 65 years. Symptomatic thrombosis was confirmed in 2 patients (4.3%), asymptomatic thrombosis was detected in another 20 patients (43.5%), no thrombotic changes were seen in 24 patients (52.2%). No significant impact of age, gender, site of insertion or preventive dose of low molecular heparin on the presence of thrombosis was recorded. In whole group of 360 patients the number of clinically diagnosed upper limb thrombosis was 17 (4.7%). In no patients the symptoms or signs of pulmonary embolism or infected thrombosis were presented.
Discussion and conclusions: The rate of symptomatic upper limb thrombosis after midline insertion is below 5%, however the rate of asymptomatic thrombosis is high. The development of upper limb thrombosis after midline catheter insertion is not associated with age of patients, gender, site of insertion or preventive dose of low molecular heparin.
P-009 PICC OR PORT IN ONCOLOGY?
V. Manasek, S. Jinkova, L. Olosova, L. Chlachula
Novy Jicin Hospital, Novy Jicin, Czech Republic
Introduction: The choice of adequate venous access device (VAD) is a current topic in clinical practice, especially in case of longterm therapy. This is crucial to be engaged to this issue especially in oncology since specific anti-cancer therapy is performed mainly via parenteral route of administration. In case the VAD is indicated, we are often faced with deciding whether a particular patient should be refer for PICC insertion or port implantation.
Methods: The group of patients indicated for long-term VAD placement was analyzed in our centre in order to specify the ratio between PICCs' and venous ports' implantations. We focused on indication criteria that was used when choosing between PICC and port. Specific factors were evaluated in relation to the nature of the malignancy, patient's characteristics and duration of the planned treatment. The average dwell time and complications rate were assessed.
Results: We defined particular criteria to facilitate the decision when choosing between PICC or port with respect to the type and length of the planned treatment and patients' conditions. Special clinical situations in cancer treatment with preference for the introduction of PICC instead of port were defined. We suggest an approach to the choice of the most appropriate venous access device for the oncology patient.
Conclusions: PICC and port are among the most common types of VADs used for administration of parenteral drugs in oncology. Specific criteria might be assessed in order to facilitate the decision-making process in selection between PICC and port.
P-010 ADVANCES IN CANCER CHEMOTHERAPY PATIENTS PICC CENTRAL CATHETER-RELATED BLOODSTREAM INFECTION RISK FACTORS AND PREVENTION
Y. Wang1, X. Ma1
1Tianjin Medical University Cancer Hospital, Tianjin, China; 1Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences, Tianjin, China
Peripherally inserted central catheter (PICC) is a deep vein puncture technique which peripherally imported and located at the end of the superior vena cava. It has many advantages, such as highly puncture success rate, short operating time, fewer complications, long retention time, puncture technique is easy to master and so on. Chemotherapy patients need several cycles of chemotherapy. Because of the weak immunity, local or systemic catheter-related infection often happens during indwelling catheter. Central catheter-related bloodstream infections (CLABSI) even occurs severely. Thus, with the extensive application of PICC, there is a risk factor of infection in such an invasive procedures. The prevention of infection has become an important part of work for cancer nurses during catheter and maintenance. Except the strict aseptic, oncology nurses should also master skilled operating skills and high sense of responsibility to reduce the chance of exogenous infection of PICC. At the same time, oncology nurses should master the puncture indications strictly, monitor the indicators of patients who have the risk of infection regularly, implement protection measures proactively, explore effective ways to prevent CLABSI occurs actively, PICC quality management, and finally to improve quality of care. Therefore, we need to do our best in the catheter, catheter maintenance, quality control, standardized operation and other aspects. To improve the quality of care, every details are important, such as selecting the correct medical countermeasures, enhancing the training, enhancing nurses awareness of anti-infection and so on. So that our goal of zero risk, no infections, no tolerance happen. In that way, catheter-related infections could become a completely preventable infection.
P-011 30 DAYS ANTIMICROBIAL EFFICACY OF NON-LEACHING CENTRAL VENOUS CATHETERS
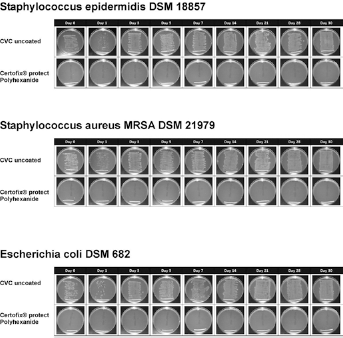
Introduction: Central venous catheters (CVCs) are widely used in intensive care but increase the incidence of adverse events, especially catheter-related blood stream infections (CRBSIs). Coagulase-negative staphylococci, such as S. epidermidis and Staphylococcus aureus, are the most frequent cause of CRBSIs. These bacteria grow because a biofilm has developed. The inhibition of bacterial growth by antimicrobial catheters helps to prevent surface colonization and improve safety. Certofix® Protect is the third generation of CVC, with non-leaching additives and antimicrobial activity from the catheter tip to the connectors.
Methods: The antimicrobial performance (30 days) of non-leaching antimicrobial CVCs on 7 typical CVC-associated infection bacteria was tested with the “Roll-Out” method (Staphylococcus epidermidis, Staphylococcus aureus MRSA and E. coli, Enterococcus faecalis, Pseudomonas aerugionosa, Klebsiella pneumoniae and Candida albicans). After inoculation, washing, incubation at 37°C, immersion in a minimum medium solution, and a second washing process, the catheter sample was placed on an agar plate and rolled 3 times over the agar plate to transfer surface bound bacteria to the agar medium. After overnight incubation (37°C), bacterial growth was recorded by photography.
30 day antimicrobial efficacy of non-leaching central venous catheters.
Results: The present in-vitro data demonstrate that non-leaching antimicrobial CVCs (e.g. Certofix® Protect, B.BRAUN) exhibit antimicrobial efficacy and prevent biofilm formation from gram-positive, gram-negative bacteria and fungi for up to 30 days. The study was performed in direct comparison with a non-antimicrobial control catheter, on which all 7 test strains were able to grow to an established surface biofilm.
Discussion and conclusions: This is the first in-vitro study to demonstrate antibacterial surface activity and prevention of biofilm formation with antimicrobial, non-leaching CVCs by using the “Roll-Out” method over a period of 30 days. These results demonstrate that non-leaching antimicrobial CVCs can prevent microbial colonization and infection.
P-012 MICROBIOLOGICAL CONTAMINATION OF A POSITIVE- AND A NEUTRAL- DISPLACEMENT NEEDLELESS INTRAVASCULAR ACCESS DEVICE IN CLINICAL USE
A.L. Casey, T.J. Karpanen, P. Nightingale, T.S.J. Elliott
University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK
Introduction: The risk of bloodstream infection (BSI) associated with needleless intravascular (IV) devices is the subject of debate. The aim of this study was to compare microbial contamination of a positive-and a neutral-displacement needleless IV access device.
Methods: A positive-displacement device was used for 6 months on all patients located on a haemato-oncology ward with a central venous catheters (CVC) in situ. Three months prior to and following this period, a neutral-displacement device was used. Following seven days of use, the microbial contamination of the devices was determined. The rate of central-line associated bloodstream infection (CLABSI) per 1000 patient days was also evaluated during the study period.
Results: 162 patients were studied and microorganisms recovered from the external silicone compression seal of 118 of 281 (42%) neutral-displacement devices compared to 79 of 276 (29%) positive-displacement devices (OR: 1.81; 95% CI: 1.27; 2.57, P = 0.001). The internal fluid pathway of 37 of 281 (13%) neutral-displacement devices were contaminated with microorganisms compared to 11 of 276 (4%) of positive-displacement devices (OR: 3.65; 95% CI: 1.82; 7.32, P = 0.0001). There was no significant difference in the rates of CLABSI between the periods during which the neutral- and positive-displacement devices were used (6.84 and 6.62 per 1000 patient days respectively, P = 0.87).
Discussion and conclusions: In contrast to previous reports, the rate of CLABSI did not increase with the introduction of the positive-displacement device. Indeed, the lower levels of external and internal microbial contamination observed with the positive displacement device may reduce the risk of microbial contamination of CVC and associated infection acquired via the intraluminal route. Further studies are required to investigate this observed difference in contamination and how this may impact on CLABSI rates.
P-013 BLOOD CLEARANCE OF PERIPHERAL IV CATHETERS WITH ADEQUATE FLUSHING TECHNIQUE
J. Bruenke
QualityLabs BT GmbH, Nuremberg, Germany
Introduction: Recent research investigated the potential risk of biofilm formation inside blood control IV catheters. However, studies show that an IV catheter can be maintained patent without an increase of catheter-related complications, if the catheter is flushed once a day.
This study intends to look into this controversy from a clinical perspective and prove that all blood can be flushed from IV catheters, thus reducing the risk of bacteria formation.
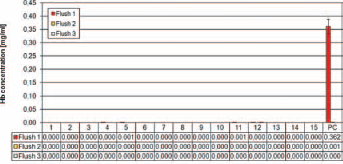
Methods: The catheter was inserted into an “artificial vein” composed of an in-stopper connected to a Heidelberger tube which was connected to a blood bag elevated to simulate patient's blood pressure. After the catheter hub was filled with blood, the needle was removed and discarded. Then, the catheter was flushed with a 3 ml syringe prefilled with a solution of 0.9% sodium chloride by pulsatile technique. After syringe disconnection, the catheter was closed with a cap. The flushing process was repeated 3 additional times, after 24 hours. Each flushing fraction was analyzed for traces of hemoglobin by using Drabkin's reagent and spectrophotometric reading. In total, 15 B.Braun Introcan Safety® 3 IV catheters were tested.
Results: Of the 15 tested Introcan Safety® 3 IV catheters, 13 were completely cleared during the first flush. Two of the 15 devices showed a clearance of 99.7% during the first flush and a complete clearance after the second flush. No hemoglobin was present in the subsequent flushing steps in any of the tested devices.
Discussion and conclusions: An hemoglobin clearance of >99.7% was achieved in the Introcan Safety® 3 already after the first flush of 3 ml 0.9% sodium chloride solution applied directly after blood aspiration. All tested catheters demonstrated a complete hemoglobin clearance latest after the second flush. Complete hemoglobin clearance of the Introcan Safety® 3 can be achieved by applying an adequate flushing technique of the devices.
Introcan Safety® 3 - Hemoglobin Detection; 3 consecutive flushings of 15 individual devices and positive control.
P-014 AN OVERVIEW OF PERIPHERALLY INSERTED CENTRAL VENOUS CATHETER-ASSOCIATED BLOODSTREAM INFECTIONS IN A PRIVATE HOSPITAL IN BRAZIL
Background: Although necessary in healthcare practice, central lines may be associated with bloodstream infections (BSI). Peripherally inserted central venous catheters (PICC) are increasingly being used to provide short to medium-term central venous access. We aimed to describe the incidence of PICC-BSI in intensive care units (ICU) and non-ICU setting in a 300-bed Brazilian Hospital, over 28 months.
Methods: PICC-BSI episodes occurred since August 2013 to November 2015 were detected by active surveillance by the Infection Control Team, according to National Healthcare Safety Network criteria. Statistical analysis was performed using a Z-test.
Results: There were 14 PICC-BSI in 12,142 patients-day with PICC (rate: 1.2 per 1,000 PICC/day). When stratifying by setting, ICU and non-ICU rates were, respectively, 2.1 and 0.5 (p = 0.01). Stratifying by type of patients, rates were 2.9 for neonates and 0.9 for adults (p = 0.02). There was no PICC-BSI in pediatric settings. The main microorganisms identified were Gram-negatives (50.0%), with a predominance of Klebsiella pneumoniae, followed by Grampositives (42.9%). There was one case of fungus (Candida lipolytica). There were no BSI associated deaths.
Discussion and conclusions: Some strategies have been taken to decrease PICC-BSI incidence: consider PICC-BSI rate as an institutional strategic indicator in Balanced Score Card, ultrasound-guided for all PICC insertion for adults (not available for neonatal), nursing capacitation in insertion/maintenance. Considering an increasing tendency line, since Oct/15, ward for units with ZERO BSI and patient empowerment for hand hygiene and catheter care have been introduced. Our results showed that PICC-BSI rates are higher in neonatal ICU. To achieve lower rates of complications, continuous and multidisciplinary strategies need to be done, focusing on motivation, education, monitoring and dissemination of information, with especial attention to leadership involvement. Besides, a dedicated team must be contemplated as an improvement opportunity. Indeed, PICCs should be aggressively discontinued when no longer absolutely needed.
P-015 A COMPARISON OF PERIPHERALLY INSERTED CENTRAL VENOUS CATHETER AND OTHER CENTRAL LINE-ASSOCIATED BLOODSTREAM INFECTIONS RATES IN A PRIVATE BRAZILIAN HOSPITAL
Background: Although necessary in health care practice, central lines (CL) may be associated with bloodstream infections (BSI). Peripherally inserted central venous catheter (PICC) seems to have lower BSI rates when compared to other CL. We aimed to compare the incidence of PICC and non-PICC BSI in a 300-bed Brazilian Hospital.
Methods: BSI cases were detected by active surveillance by the Infection Control Team, according to National Healthcare Safety Network criteria. The historical series from August 2003 to November 2015 was analyzed in intensive care units (ICU) and non-ICU settings. Statistical analysis was performed using a Z-test.
Results: Generally, there were 14 PICC-BSI in 11,531 PICC-day (rate: 1.2 per 1,000/PICC-day) and 73 non-PICC BSI in 54,152 other CL-day (rate: 1.3) in our institution (p = 0.71). In adult patients, PICC and non-PICC BSI rates were 0.9 and 1.3 respectively (p = 0.23). For pediatric patients, these rates were 2.9 for PICC and 1.0 for non-PICC (p = 0.06). When stratifying by type of setting, there was no statistical difference between PICC and non-PICC BSI in ICU (2.1 and 1.7 respectively - p = 0.56) or general floor (0.5 and 1.0 respectively - p = 0.44).
Discussion and Conclusions: There was no statistical difference between PICC and non-PICC BSI at our facility. Anyway, the PICC-BSI target must be ZERO and to achieve this goal, continuous and multidisciplinary strategies need to be done, focusing on motivation, education, monitoring and dissemination of information, with especial attention to leadership involvement. Indeed, PICCs should be aggressively discontinued when no longer absolutely needed.
P-016 THE EFFECT OF IMPLEMENTATION OF AN ADULT'S HOSPITAL-WIDE VASCULAR ACCESS TEAM ON CENTRAL LINE-ASSOCIATED BLOODSTREAM INFECTIONS
R.B. Cechinel, R.A. Zimerman, D.S. Nunes, D.S.G. Veçossi, K. Mesquita, L. Galo, J.M.O. Netto, N.N. Duster, R.M. Somensi, T.C.T. Sukiennik
Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, Brazil
Introduction: Infusion therapy is complex, invasive and risky for many patients. A vascular access team (VAT) could improve infusion practice within the organization by serving as consultant, educator, and advisor to the primary care team. In this study, we evaluated the effect of a VAT on the incidence of central line-associated bloodstream infection (CLABSI) in adults patients admitted to a hospital in Southern Brazil.
Methods: The setting of this study is the Pavilhão Pereira Filho Hospital at the Santa Casa de Misericórdia de Porto Alegre. In 2015 it counted 85 beds, 930 admissions, and 26515 patients-days. Distribution over the various wards was as follows: one medical/surgical intensive care unit, one adult step-down unit and three medical/surgical wards. The study used a before and after design. Post-intervention CLABSI rates were evaluated and compared with pre-intervention data. The VAT is composed of one infectious diseases physician and four registered nurses who are specially trained in infusion therapy. The team acted as a clinical resource for vascular access and infusion therapy, providing daily assessment of patients requiring central line. These assessments included: sterile dressing evaluation and changes, daily monitoring of the insertion site and identification of lines no longer needed. The team performed many others tasks throughout the hospital as well, including: insertions of peripherally inserted central catheters, desobstructions of central venous catheters, introduction of new technologies, provision of consultation services and education for patients and families.
Results: Overall CLABSI decreased by 68% after implementation of the VAT. Pre-intervention mean overall CLABSI rate was 4.25/1,000 catheter-days, as compared with 1.33/1,000 catheter-days after intervention.
Discussion and conclusions: The implementation of a vascular access team combined with introduction of chlorhexidine dressings, chlorhexidine/silver sulfadiazine antimicrobial catheters, and other behavioral changes was associated with a reduction in CLABSI in our hospital.
P-017 INDEPENDENT REVIEW TEAM VERSUS STANDARD INFECTION PREVENTIONALIST FOR CLABSI DIAGNOSIS: A SYSTEMATIC REVIEW OF DIAGNOSTIC ERROR
E.N. Larsen1, N. Gavin1, N. Marsh1, J. Webster1
1Griffith University, Nathan, Australia; 1Royal Brisbane and Women's Hospital, Herston, Australia
Introduction: Central venous access devices (CVADs) are frequently associated with hospital acquired infections known as central line-associated bloodstream infections (CLA-BSI). Classification and diagnosis of CLA-BSI is usually the responsibility of infection preventionalists (IPs) or other infectious diseases professionals, and is often based on National Health and Safety Network (U.S) definitions. Application of these definitions is sometimes inaccurate based on subjective clinical decision-making. Validation of data is essential to ensure accuracy of reporting. The objective of this systematic review was to compare hospital reported CLA-BSI rates with independent review team classification.
Methods: MEDLINE, CINAHL, Scopus and ProQuest were searched for eligible articles. Full-text studies comparing the diagnostic validity of historically reported bacteraemia episodes using NHSN CLA-BSI definitions with validation team data were included. Any studies which used either a program or algorithm to conduct the diagnosis validation were excluded.
Results: 87 studies were identified in the initial search, and 8 papers including 6754 patient records met the eligibility criteria. Of the total sample, validation teams found N = 5646 true negatives; N = 701 true positives; N = 124 false positives and N = 283 false negatives. Sensitivity (95% CI) ranged from 0.42 (0.15, 0.72) to 0.88 (0.77, 0.95) and specificity (95% CI) from 0.70 (0.58, 0.81) to 0.99 (0.99, 1.0). This indicates that clinicians are more likely to under-report than over-report. Sub-group analysis of individual patient groups was not possible due to the homogeneity of patients. The overall risk of study bias was low using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS 2) tool.
Discussion and conclusions: Validation of publicly reported data is essential in order to facilitate benchmarking between facilities, as well as evaluate the success of interventions to reduce the incidence of CLA-BSI. Continuous work is required to ensure classification reliability and further studies are needed to gain true understanding of CLA-BSI reporting bias.
P-018 CHLORHEXIDINE/SILVER SULFADIAZINE IMPREGNATED CATHETERS ASSOCIATED WITH DECREASE CENTRAL LINE-ASSOCIATED BLOODSTREAM INFECTION IN CRITICALLY ILL PATIENTS
R.A. Zimerman, R.B. Cechinel, D.S. Nunes, D.S.G. Veçossi, K. Mesquita, L. Galo, D.C. Birriel, J.M.O. Netto, R.M. Somensi, T.C.T. Sukiennik
Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, Brazil
Introduction: Central venous catheters (CVCs) are essential devices for the administration of fluids, medications, blood products and parenteral nutrition. However, bloodstream infections are common complications of their use. Several measures have been developed to reduce such infections, including antimicrobial or antiseptic impregnated catheters. In this study, we evaluated the impact of using CVCs impregnated with chlorhexidine and silver sulfadiazine on central line-associated bloodstream infection (CLABSI) in patients in a medical/surgical intensive care unit (ICU).
Methods: The study was conducted between January 2015 through December 2015 on the Pavilhão Pereira Filho Hospital at the Santa Casa de Misericórdia de Porto Alegre. The study consisted of two phases. The first phase was from January 2015 through August 2015, during which only uncoated, conventional CVCs were used (baseline). The second phase occurred between September 2015 and December 2015, during which most of the devices used were second generation chlorhexidine and silver sulfadiazine impregnated catheters (ARROWg+ard Blue PLUS). The ICU consisted of a 14 bed unit. All patients with CVCs admitted to the ICU were subjects for the surveillance of CLABSI. CLABSI were defined as per the Centers for Disease Control and Prevention criteria.
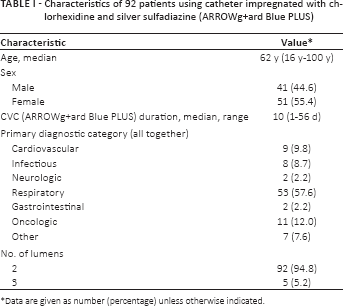
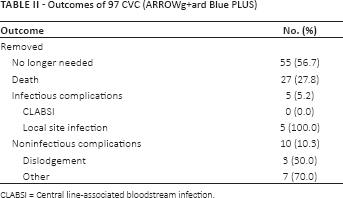
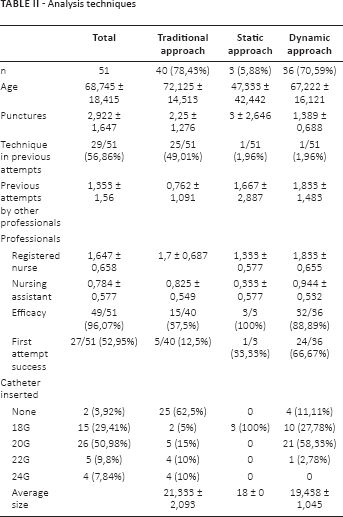
Results: The rates of CLABSI were compared for the two study periods to determine the impact of using the impregnated catheters in the ICU. During the study period 97 catheter impregnated with chlorhexidine and silver sulfadiazine were placed in 92 patients (Tabs. I and II). The rate of CLABSI in the ICU unit decreased 87% between periods, from 5.23 to 0.72 per 1,000 catheter-days. Noteworthy the single CLABSI case observed during intervention occurred in a patient with conventional, non-impregnated device.
Discussion and conclusions: Our study showed that among critically ill patients, the use of second generation antiseptic impregnated CVCs in the ICU was associated with a significant decrease in CLABSI.
Characteristics of 92 patients using catheter impregnated with chlorhexidine and silver sulfadiazine (ARROWg+ard Blue PLUS)
CVC (ARROWg+ard Blue PLUS) duration, median, range
10 (1-56 d)
Primary diagnostic category (all together)
Cardiovascular
9 (9.8)
Infectious
8 (8.7)
Neurologic
2 (2.2)
Respiratory
53 (57.6)
Gastrointestinal
2 (2.2)
Oncologic
11 (12.0)
Other
7 (7.6)
No. of lumens
2
92 (94.8)
3
5 (5.2)
Data are given as number (percentage) unless otherwise indicated.
Outcomes of 97 CVC (ARROWg+ard Blue PLUS)
Outcome
No. (%)
Removed
No longer needed
55 (56.7)
Death
27 (27.8)
Infectious complications
5 (5.2)
CLABSI
0 (0.0)
Local site infection
5 (100.0)
Noninfectious complications
10 (10.3)
Dislodgement
3 (30.0)
Other
7 (70.0)
CLABSI = Central line-associated bloodstream infection.
P-019 BLOOD TRANSFUSION VIA INTRAOSSEOUS ACCESS: A PRE-CLINICAL STUDY
D.F. Montez1, T.A. Puga1, C. Davlantes1, R. Higgins1, L.J. Miller1, T.E. Philbeck1
1Teleflex Medical, San Antonio, USA; 1The University of Texas Health Sciences Center at San Antonio, San Antonio, USA
Introduction: Intraosseous vascular access (IO) is an alternative for patients with inadequate intravenous access; with effective intraosseous blood transfusion reported by Tocantins as early as 1941. The possibility of hemolysis and ability to achieve clinically beneficial flow rates has been raised in discussions of IO blood transfusion. The objectives of this prospective pre-clinical study were to transfuse whole blood via IO access to evaluate for hemolysis and determine infusion rates.
Methods: 1-2 units of blood were collected from the pre-vena cava of 10 mature anesthetized swine. The blood was auto-transfused via the IO route using a blood transfusion set and pressure bag at 300 mmHg. Venous blood samples for the measurement of free hemoglobin were collected from the blood transfusion bags and swine pre- and post-transfusion.
Results: 18 units of whole blood were transfused in one unit quantities into 10 swine; 8 received bilateral transfusions. Seventeen transfusions were given through the proximal humerus and one through the proximal tibia. Mean blood volume delivered through each limb was 266 ± 74 ml (n = 18); mean transfusion time was 5.7 ± 3.5 minutes (n = 18); and the mean flow rate was 61.6 ± 37.3 ml/min (n = 18). Free hemoglobin results were obtained from 6 swine. The mean free hemoglobin values were: pre-transfusion 7.05 ± 5.2 mg/dL (n = 6); post-transfusion 7.16 ± 3.62 mg/dL (n = 6); blood collection bags 3.81 ± 5.12 mg/dL (n = 12); all within the swine reference interval (0-10 mg/dL). One swine demonstrated free hemoglobin levels above the upper limit of the reference interval in all samples suggesting hemolysis unrelated to IO transfusion.
Discussion and conclusions: Pressurized blood transfusion through IO vascular access resulted in acceptable flow rates and did not result in appreciable hemolysis, as indicated by free hemoglobin values. Limitations of this study include sample size and use of swine instead of humans.
P-020 CASE REPORT: EPIDERMOLYSIS BULLOSA USING A PICC LINE
T.C. Silva
Sociedade Beneficente de Senhoras Hospital Sírio Libanês, São Paulo, Brazil
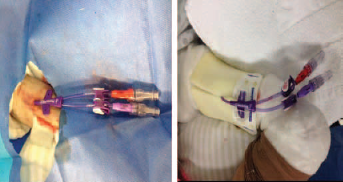
Epidermolysis bullosa is a rare, serious, non-contagious inherited disease. It features blistering through the body accompanied by a very high sensitivity of the body. It may appear spontaneously through trauma, or even change in temperature. The disease is classified according to the level shows. The diagnosis is made by biopsy. We searched in major databases and there no reports in literature of PICC use of associated with Epidermolysis Bullosa. This study is a case report of a 31-year old patient diagnosed with epidermolysis bullosa and skin cancer, requiring a safe route for administration of chemotherapy and sedation during radiotherapy. The patient was sedated and a 6 Fr double lumen power injectable tip catheter was inserted in the right arm; however, these patients cannot have adhesives used in direct contact to the skin, therefore, the catheter was sutured and a medicated dressing, a sterile sponge cover, catheter stabilizer and local bandaging were used (Fig. 1). After ten days of patient's catheter was stable, without bleeding in catheter and the dressing was intact. (Fig. 2). The power injectable peripherally inserted central catheter is a safe route for chemotherapy administration in patients with epidermolysis bullosa, it reduced discomfort and pain patients in chemotherapy. It is a safe alternative for patients in critical care.
P-021 PERIPHERALLY INSERTED CENTRAL CATHETER-RELATED UPPER EXTREMITY VENOUS THROMBOSIS IN ONCOLOGY PATIENTS: A PROSPECTIVE STUDY BASED ON DOPPLER ULTRASONOGRAPH
G.R. Wang
Sichuan Cancer Hospital, Chengdu, China
Introduction: Access devices include peripheral IVs, Hickman catheters, peripherally inserted central catheters (PICCs). The advent of PICCs has considerably improved the management of oncology patients because it facilitates transfusions, chemotherapy, parenteral nutrition, and blood sampling. Unfortunately, a known complication with the use of PICCs is upper extremity venous thrombosis (UEVT). While many studies have addressed risk factors for PICC-related UEVT, few studies have used prospective Doppler ultrasonography (US) in antithrombotic prophylaxis. Our key objectives were to estimate the incidence of PICC-related UEVT in oncology patients and to assess the role of Doppler US for initiation of antithrombotic prophylaxis.
Objective: PICCs are associated with an increased risk of venous thrombosis. This was a prospective study with each patient being followed for 6 weeks. It had two objectives: to estimate the incidence of UEVT associated with PICCs in oncology patients and to evaluate the role of the Doppler ultrasonography in antithrombotic prophylaxis.
Methods: From April 2014 to October 2014, we analyzed a series of 245 consecutive oncology patients undergoing chemotherapy via PICC for an overall number of 246 PICC placements assessing the role of Doppler US for initiation of antithrombotic prophylaxis. The series encompasses two cohorts of patients, those who received regular weekly Doppler US screening for UEVT prophylaxis and those who did not (no-Doppler US).
Results: Of 246 insertions, we observed 90 (36.59%) episodes of UEVT, 62 of them were asymptomatic in Doppler US group and 28 of them were symptomatic in no-Doppler US group separately. Doppler US patients had a significantly lower rate of symptomatic UEVT (0%) than no-Doppler US patients (23.53%; p = 0.00).
Conclusions: Our prospective study suggests that the rate of PICC-related UEVT in oncology patients is high and the occurrence of symptomatic UEVT could be lowered with regular weekly Doppler US screening following PICC insertions.
P-022 SAFETY AND EFFICIENCY OF PERIPHERAL INSERTED CENTRAL CATHETER (PICC) USE FOR INTRAVENOUS CONTINUAL INFUSION OF 5-FLUORURACIL IN OUTPATIENTS
M.A. Cubero, M. Montealegre, S. Varga, M. Zabala, J. González
Hospital Clinico San Carlos, Madrid, Spain
Introduction: 5-fluoruracil is a chemotherapy agent, which upon being administered through a peripheral venous line can lead to eczema reactions and sensitivity to light accompanied by a maculopapular rash and itching at the injection site with rare incidences of phlebitis and extravasation. In some cases hyperpigmentation of the veins utilized for the administration of the medicine can be observed, which is most frequent and intense after prolonged intravenous therapy through a peripheral venous catheter.
Methods: Retrospective observational study of the use of PICC line for the administration of 5-Fluoruracil in continuous intravenous administration in outpatient therapy in patients diagnosed with colorectal cancer.
All the catheters were inserted with ultrasound guided PICC line placement by the Hospital Clínico San Carlos Intravenous Therapy Team, the PICC being the high flow polyurethane and single lumen, 5French.
Results: In 2015 the team inserted a total of 76 PICC lines in outpatient therapy in oncological patients for the administration of chemotherapy, of which 25 catheters were for 5-Fluoruracil in continuous intravenous administration. Those PICC catheters were inserted for an average length of 63 days with a maximum of 258 days and a minimum of 28 days.
No complications resulted during their use, none of them were removed due to infection or thrombosis, the main motive of removal being the end of treatment or a change in treatment (80%), followed by the insertion of another type of central catheter (16%).
Discussion and conclusions: We can conclude that the PICC catheter is safe as a means of long-term venous access for the administration of 5-Fluoruracil in continuos IV therapy, reducing the number of treatments with chemotherapy administered through a peripheral venous line thereby avoiding possible cutaneous toxicity.
It reduces the number of patient hospital admissions, increasing the wellbeing and comfort of the patient.
P-023 PORT INSERTION: TUNNELED VS NON TUNNELED
T.W. Petry
GBMC, Baltimore, USA
Totally implanted devices: Making the right choice for insertion and for the patient population.
Introduction: Traditionally implanted devices have been inserted using an open surgical technique. Advances in technology, design and percutaneous insertion techniques have improved the choices available both for the operator and the patient. The insertion of an implantable device is just one aspect of the complete process required, to ensure the right implantable device is chosen to enable a smooth patient pathway, without unintended outcomes.
Methods: A comprehensive review of the process/protocol used to assure the correct implantable device is used will be presented, including patient assessment, review of intravenous therapy needs, systematic approach to determining the correct “size/profile” of implantable device. Consideration will also be given to determine the need for power injectable compatible devices. Procedural insertion techniques as to site/vessel selection will also be discussed, along with the need to tunnel or not tunnel.
Results: A series of case histories will be described, including a review of patient outcomes, describing the impact of correct “size/profile” choices, functionality, and complications.
Discussion: To ensure and improve patient outcomes, insertion of implantable devices has many variable aspects. The insertion of the device is one aspect of a comprehensive process, from patient selection, correct profile of the device and functionality. Pre and post insertion considerations play a vital part in providing a safe, complication free process.
P-024 TUNNELED CENTRAL VENOUS CATHETER REPLACEMENT THROUGH THE EXISTING TUNNEL WITHOUT USING A GUIDE-WIRE - METHOD REVIEW (VIDEO) WITH CASE REPORT
M. Atic1, D. Tulumovic1, A. Jasarevic1, E. Mesic1, N. Atic1, E. Hodzic1, V. Habul1, D. Trojak1, M. Dugonjic-Taletovic1
1University clinical center Tuzla, Tuzla, Bosnia-Herzegovina; 1University clinical center Tuzla, Clinic for Internal Medicine, Tuzla, Bosnia-Herzegovina
Introduction: Tunneled central venous catheter (CVC) is a common vascular access for hemodialysis, especially in cases of poor and exhausted possibilities for construction of arteriovenous fistula.
Methods: The skin over the subcutaneous tunnel, catheter entrance, catheter is cleaned with disinfectant. Local anesthesia of tunnel is performed by injecting 10 ml of xylocaine, with special attention to the ‘cuff’. Using mechanical force old catheter is carefully pulled out of the tunnel, and before the tunnel is closed a new catheter is inserted. After conserving and dressing of catheter it's necessary to take chest X-ray to determine the position of the catheter, after this is done the patient can immediately start with hemodialysis. There is no need for dose adjustment of anticoagulants. Antibiotics are administered, and it's necessary to monitor the parameters of inflammation and blood cultures.
Results: From 175 of patients, 25% of them are dialyzed through a CVC. The described method of catheter replacement was performed in 23 patients who had afunctional or mechanically damaged catheter, and were without clinical and laboratory evidence of inflammation. The procedure was successful in 17 patients, with the immediate possibility of performing hemodialysis. Flow rates and hemodialysis quality were optimal, and there was no need for hospitalization. Control markers of inflammation and blood cultures remained negative. In 5 cases the procedure could not be done (3 inability of the mechanical removal of CVC, 1 inability of passing a catheter through the tunnel, 1 deflection of the catheter into the jugular vein), when conventional method of replacement was performed.
Conclusions: Replacing of permanent CVC in certain cases can be performed through the existing tunnel without using a guide wire. The procedure is simple and safe, and its advantages are avoiding of surgical intervention, unnecessary adjustment of anticoagulants, avoiding shortening the duration of hemodialysis and hospitalization.
P-025 CREATING NATIVE ARTERIOVENOUS FISTULA FOR HAEMODIALYSIS: WITHOUT AGE LIMIT
K. Jemcov1, B. Baralic1, V. Aleksandra1, M. Radovic1
1Clinical Center of Serbia, Belgrade, Serbia; 1University of Belgrade, Belgrade, Serbia
Introduction: Creation of permanent vascular access in elderly patients who begin maintenance HD treatment might be very difficult. The aim of the study was to compare primary AVF creation success between elderly and younger patients.
Methods: A prospective, observational, single center study compared outcome of native AVF creation in 338 consecutive, incident patients during 5 years' period (2011-2015) allocated in two groups: elderly (mean age 74.2 ± 5.8, 66 to 90 years old, N = 135) and younger (51.1 ± 5.7, 20 to 65 years old, N = 203; p<0.0001). We compared primary AVF patency and age, gender, frequencies of comorbidities, diabetes mellitus, hypertension, permanent catheter placement and peritoneal dialysis (PD).
Results: Overall primary AVF creation rate was 89.3%, 9.7% out of patients had permanent catheter for HD, similarly frequent both in elderly (14%) and younger (8.3%) patients' groups (p = 0.107). Only 3 patients were transferred to PD. Men were borderline significant older than women (p = 0.054). Primary AVF success was more frequent in men than women (p = 0.0009). Men shown significant correlation between age and comorbidities (r1 = 0.283) and hypertension (r1 = 0.206), as well as women (r1 = 0.232; all p<0.05).
Comorbidity frequency was similar between elderly and younger patients (p = 0.278), and it correlated significantly with age (r1 = 0.254), diabetes (r1 = 0.232) in younger patients' group, and hypertension (r1 = 0.176) in elderly patients' group (all p<0.05).
Discussion and conclusions: Age, comorbidities presence and hypertension were associated with less favorable for native AVF creation outcome in elderly, and diabetes in younger patients. Overall AVF success rate close to 90% and 86% in elderly patients, justifies AVF attempt in those patients on maintenance HD.
P-026 PREDICTORS OF REINTERVENTION AFTER A PRIMARY INTERVENTION IN A VASCULAR ACCESS: MORE WORK IS NEEDED
A.T. Lanca Baptista, R.S. Escoli, E.M. Lopes, P.A. Santos, C.M. Nascimento, L. Cobileac, T. Sattut, F.R. Sofia, A.I. Reis, C.M. Marchão, J.C. Sequeira Andrade Fresenius Medical Care, Entroncamento, Portugal
Introduction: A long lasting arteriovenous (VA) free of complications that provide good quality dialysis has been a difficult goal to achieve. Vascular interventions have emerged to override this complex problem yet it still remains unsatisfactory.
Methods: Single-centre observational, retrospective cohort study of 70 End Stage Renal Disease vascular accesses (arteriovenous fistula - AVF or polytetrafluoroethylene grafts - PTFE) that undergone their first intervention (angioplasty or surgical revision) between 2011 and 2012 and were followed up for a 3 year period. We sought to analyze which predictors lead to a reintervention.
Results: Seventy dysfunctional vascular accesses (68,8% AVF and 31,4% PTFE) were assessed, where 58,6% were left VA and 41,4% were right VA. Out of these 35,7% were radiocephalic, 30% brachiocephalic, 22,9% brachio-basilic, 7,1% brachioaxilar, 1,4% femorofemoral. Among all, 58,6% belong to males and 41,1% to females with a mean age of 70 ± 13 years out of which 70% were older than 65 years old. Mean time to reintervention (time spent from first intervention to the second one) was 446 ± 400 days. During the follow-up 48,6% undergone a 2nd intervention, 28,6% a 3rd intervention, 17% a 4th intervention, 11,4% a 5th intervention and 7,1% a 6th intervention. There was 76,5% postprocedural success The suggested predictors of reintervention were the following growing aneurism (p = 0.056), intravascular high-pressures (p = 0.034), reduced vascular flow (p = 0.006), failure of previous intervention (p≤0.001), number of lesions encountered superior to 1 (p = 0.004) and angioplasty without stent (p = 0,002). However, in a Cox proportional hazard model, none of the suggested predictors were significant for the combined endpoint of reintervention.
Conclusions: Based on this study it was not possible to identify independent predictors of reintervention. A larger sample size together with longer follow-ups as well as other factors might be involved in these phenomena and clarify these predictors.
P-027 RISK FACTORS OF THROMBOSIS IN PERIPHERALLY INSERTED CENTRAL CATHETERS IN ONCOLOGIC PATIENTS. EXPERIENCE OF SINGLE CENTER
B. Moreno-de Gusmão1, V. Armenteros-Yeguas1, M.A. Tomás-López1, I. López de Aberasturi1, M. Mateos-del Pino1, M.I. Moraza-Dulanto1
1Albert Einstein Hospital, São Paulo, Brazil; 1Araba University Hospital, Vitoria-Gasteiz, Spain; 1Araba Research Unit, Vitoria-Gasteiz, Spain
Introduction: Thrombosis is one of the complications described in the literature related to Peripherally Inserted Central Catheters (PICC). The aim of this study was to describe the incidence of thrombosis in oncologic patients with PICC and identify predictive risk factors.
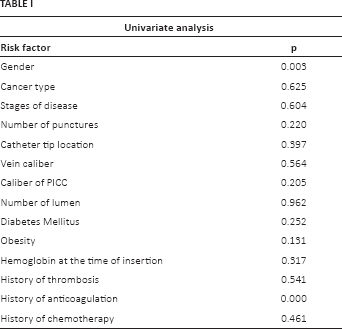
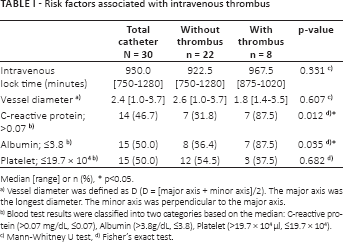
Methods: A prospective observational study was conducted in a sample of all PICCs inserted in patients with solid or hematologic cancer between January 2012 to February 2013. The variable thrombosis was reported after assessing the symptoms and confirmation by Doppler sonography. Risk factors of thrombosis were collected checking medical records: gender, cancer type, stage of disease, number of punctures, catheter tip location, vein caliber, caliber and number of lumen, diabetes mellitus, obesity, hemoglobin at the time of insertion and previous history of thrombosis, anticoagulation and chemotherapy. Univariate analysis was performed for each risk factor.
Univariate analysis
Risk factor
p
Gender
0.003
Cancer type
0.625
Stages of disease
0.604
Number of punctures
0.220
Catheter tip location
0.397
Vein caliber
0.564
Caliber of PICC
0.205
Number of lumen
0.962
Diabetes Mellitus
0.252
Obesity
0.131
Hemoglobin at the time of insertion
0.317
History of thrombosis
0.541
History of anticoagulation
0.000
History of chemotherapy
0.461
Results: 306 PICs were inserted in 293 patients. The incidence of thrombosis was 9.18% (95% CI: 5.78-12.58), 14.71% IC 95% = (8.39-21.03) for men. Gender (p = 0.003) and history of anticoagulants (p<0.001) were statistically significant. The rest of factors were not statistically significant in relation to thrombosis (Tab. I).
Discussion and conclusions: The incidence of thrombosis is in the range described in the literature. There are similar previous studies which described predictive factors (location of tumor, diameter of catheter, obesity …) but showing different and contradictory results although in this study were not statistically significant. Apparently this study supports the research lines that defend avoidance of anticoagulation prophylaxis previous PICC insertion. The main limitation of the study was the sample size and the low incidence of thrombosis which may influence the results. An extension of the study is required to analyze better the risk factors.
P-029 CHALLENGING VASCULAR ACCESS SITUATIONS
N. Nakazawa
Stanford Health Care, Stanford, USA
Introduction: Vascular access guidelines and principles of practice guide vascular access selection, insertion and management. However, there are challenging clinical situations that require critical thinking skills and a multidisciplinary approach to resolving these complex issues. This presentation presents a number of clinical situations and invite the audience to examine how they would approach each scenario.
Case study 1: Young female with a rare disorder causing continuous chylous pleural effusions, obese and pregnant, with such severe SOB that she can only tolerate sitting upright resting on a table top. Needs central access for biotherapy. What would you do?
Case study 2: Young male newly diagosed with Hodgkin's Lymphome and extremely large mediastinal mass, severe SOB. What might be your concerns and approach?
Case study 3: Female patient with end-stage liver disease who needs central access for biotherapy, morbidly obese, severely coagulopathic: INR >10, PTT >180. What do you do?
Case study 4: Complex congenital heart disease male patient with cerebral abscess. PICC ordered for 6 weeks of antibiotics. Patient has a single ventricle with history of multiple surgeries. What are your concerns?
P-030 PATHOGENESIS OF ARM LYMPHEDEMA AND IMPLICATIONS FOR VASCULAR ACCESS DEVICE SELECTION
N. Nakazawa
Stanford Health Care, Stanford, USA
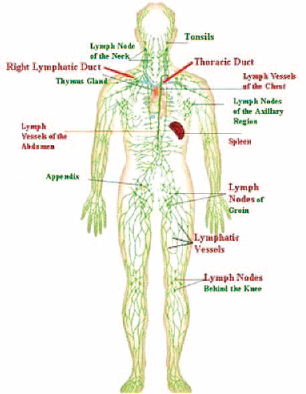
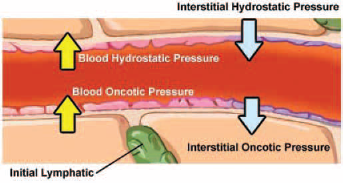
Breast cancer patients who have had axillary lymph node dissection or sentinel lymph node biopsy have a life time risk of developing arm lymphedema on the effected side. This presentation discusses the pathogenesis of lymphedema, risk factors, adverse sequelae of lymphedema, and implications for vascular access device selection.
Lymphatic system and thoracic ducts.
Interstitial hydrostatic pressure.
P-032 VASCULAR ACCESS DEVICE; ARE WE GETTING THE RIGHT LINES IN?
J. Bitmead, P. Coen
UCLH, London, UK
Introduction: Vascular Access Device (VAD) insertion is a common practice in health care settings. Most inserted VADs are Peripherally Inserted Venous Cannulas (PIVCs). Inserting PIVCs is not without risk. Patients can develop infection, phlebitis and extravasation. When reviewing bacteraemia cases, a number of patients had a large number of cannulation events.
Methods: We carried an audit to identify areas for improvement in VAD insertion. A project nurse was trained to undertake an audit of VADs over a 6 month period. Patients were visited on wards on a rotational basis and excluded Paediatric, Critical care, oncology and haematology areas.
During each visit e audited the number VADs each patient had during their admission, vein quality, the bodily site of VAD insertion, PIVC gauge and whether patients reported multiple insertions attempts.
Vein quality assessment was an adaptation of the Infection Preventions Society vessel health preservation tool as we had no access to ultrasound or vein viewer. We used a score of 1 for excellent 4 to 5 suitable veins to a score of 4 for no veins visible.
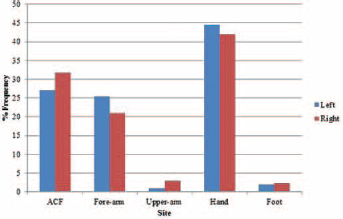
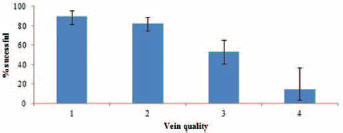
Results: We examined 951 VADs in 464 patients: 58 central VADS and 742 PIVCs; 151 were excluded due to missing documentation pertaining to type of gage and location of VAD. The most frequent insertion sites were hand (43.2%), and Antecubital Fossa (29.5%) (Fig. 1), with an equal distribution of insertions between left and right side. Vein quality is inversely correlated with decreased patient reported successful cannulation decreased (p<0.001; Fisher's exact test; Fig. 2).
Discussion and conclusions: A number of factors can affect the successful placement of PIVC, and visual vein quality is a significant one. We would need to consider the use of aids to assist with insertion of PIVC for short term infusions or the increase use of Midlines.
PIVCs stratified by insertion site and site.
% of successful insertion as a function of vein quality (PIVCs only).
P-033 REDUCING BLOODSTREAM INFECTIONS WITH CHLORHEXIDINE GEL IV DRESSING
J. Bitmead
UCLH, London, UK
Introduction: Although bloodstream infections are relatively rare in the hospitalised patient, the risk is increased by the insertion of a vascular access device (VAD) and specifically a central venous catheter (CVC). In a critically ill patient, CVCs have been used for the administration of intravenous medication and physiological monitoring; however Peripherally Inserted Central Catheters (PICC) and Midline are more frequently used for the administration of chemotherapy, parental nutrition and prolonged courses of antimicrobial therapy. Trialling and Introducing the Dressing: The introduction, trail and implementation of Tegaderm CHG™ began in 2009, initially reviewed by the Hospital's IV forum, some were concerned that the gel would be cold and uncomfortable for patients. Ten members of the group agreed that they would apply the dressing for a week and compare findings. The conclusion was that the dressing was comfortable. Formal evaluation then was carried out using the following criteria:
Ease of application;
Time taken to apply dressing;
Ability to observe the insertion site;
Ability to absorb exudate;
Ability of the gel pad to conform to and fixate the catheter;
Ease of removal;
Overall performance.
Results: The conclusion of the trial was that dressing performed in all criteria better than previous dressings used and one of the trial areas adopted the dressing immediately as the staff valued the stability especially. The majority of patients found the dressing comfortable, with only a small number of patients unable to tolerate the dressing. There were also some concerns raised about removal of the dressings, however this resolved with training.
A reduction in MRSA and MSSA bacteraemia cases in patients with IV lines has also been noted.
Discussion and conclusions: Since 2009 Tegaderm CHG™ has been successfully been used on all CVCs, PICC, arterial lines and midlines on patient over 16 years old.
P-034 PICC AND VENOUS THROMBOEMBOLISM: HOSPITAL'S CASE REPORT FROM SAO PAULO, BRAZIL
V.C. Pupin, A.R.M. Santos
Hospital Vivalle, Sao Jose dos Campos, Brazil
Introduction: PICC is a vascular device of peripherally insertion with a central localization with one or more lumens increasingly indicated for patients' intravenous therapy. PICC's insertion has grown due the safety and cost-effective it offers comparing with others central venous catheters.
Methods: It is a descriptive study, retrospective and exploratory where it was analyzed a period of 18 months, from April 2014 to October 2015.
Results: In this 18 months, it was realized 822 PICC's insertion on inpatient and intensive care units. The incidence of venous thromboembolism were on 15 cases diagnosed by ultrasonography Doppler positive for VTE, distributed in 7 patients with oncological disease and 7 with associated morbidity such as: stroke, cardiac arrhythmias, diabetes mellitus and sepsis. Only one patient was not associated with morbidityeventhough his diagnosis was urinary tract infection. The occurrence rate of VTE was 1.82% while the incidence described in literature was 13.91% for critically ill patients and 6.67% for oncological patients. The average time for the occurrence was 13.26 days and the occurence observed on the literature was 8.7 days. Only 3 patients have not had VTE prophylaxis, 1 have had contraindication and 11 patients with venous thromboembolism prophylaxis have developed the complication.
Discussion and conclusions: Although that our incidence rate was less than the rate literature describes, the PICC's indication always have to be discussed with attending physician and the decision has to be taken based on the patient's risk factors.
P-035 COMPARATIVE STUDY OF FOUR PUNCTURE METHODS FOR INSERTION OF PERIPHERALLY INSERTED CENTRAL CATHETER (PICC)
C.A. Oliveira, M.G.P. Cardoso
University Hospital of Londrina, Paraná, Brazil
Introduction: Using the PICC has been present in care nursing practice. This was initially inserted through the traditional technique known as direct, but with the advent of technological change other techniques are being used: puncture assisted and guided by ultrasound.
Methods: This is a retrospective study of descriptive and exploratory design. Held at the University Hospital of Londrina/Paraná. Data were collected in January 2016, the protocols of the catheters inserted between the years 2007 and 2015. We evaluated all data from catheters inserted by the nurse on duty of CCIV scale. The variables evaluated were: Indication, age, gender, chosen vessel, number of punctures, type of puncture, calibrate the catheter, catheter materials and reason for removal. The data collected were translated into the Epi Info version 3.5.4 program - 2012, where they performed statistical tests. In all tests the level of significance was α = 0.05.
Results: 285 catheters were inserted, and 188 by the traditional technique, 73 with puncture assisted by ultrasound and 24 with puncture guided by ultrasound. In 73% of cases the catheters were appointed to antibiotic therapy. The average age of patients was 55 years (SD: 22.08). In 64.1% of the inserts was used polyurethane catheter and 35.9% silicon. The average stay of the catheters was 13.78 days, and in 50.2% the reason for the withdrawal was high.
Discussion and conclusions: The study showed a statistically significant difference (p = 0.003), the relationship between the type of punch to the catheter dwell time, and what in the group of patients which was performed the puncture with the help of ultrasound, found If a greater number of days remaining. It is concluded from this study that technological advances contribute to the assertiveness of the procedure as well as the durability of the catheter.
P-036 NOVEL APPROACH TO DISINFECTION OF NEEDLELESS ACCESS SITES PRIOR TO USE
J.H. Garrett
PDI, Atlanta, USA
Bloodstream infections continue to be a tremendous source of mortality and morbidity in both inpatient and outpatient healthcare settings. It is important to properly disinfect all access sites prior to use with an appropriate antiseptic agent, even between sequential line accesses for procedures such as laboratory draws, medication administration, and flushing of medications. The scientific literature has been limited on two important factors regarding the best practices for disinfection of these devices: 1) the best choice for an antiseptic agent, and 2) the most appropriate scrub time to remove bioburden and pathogens from the access site. Prior best practice has historically been to utilize a 70% isopropyl alcohol prep pad at a minimum scrub time of 15 seconds up to in some institutions 30 seconds. This practice is not practical for clinicians to adhere to, therefore resulting in significant lapses in compliance and potential infection. Recent evidence has demonstrated that a novel 3.15% chlorhexidine gluconate and 70% isopropyl alcohol FDA cleared medical device used at a scrub time of five seconds is both reasonable for clinicians to adhere to and demonstrates a greater than 4 log 10 reduction in gram positive/negative bacteria as well as pathogenic fungal organisms known to be causative pathogens resulted in clinical bloodstream infections. This evidence has scientifically proven that this solution is more effective at reducing colonization of needleless connectors compared to isopropyl alcohol. This has an impact on clinician labor time as well. The use of novel technologies for disinfection of needleless access sites prior to use combined with ongoing education of healthcare providers responsible for vascular access will help mitigate risk for these largely preventable infections, reduce costs of care and associated mortality/morbidity, and improve the patient experience.
P-037 EMERGING INFECTIOUS DISEASES: CLINICAL IMPACTS TO VASCULAR ACCESS
J.H. Garrett
PDI, Atlanta, USA
Ebola Virus Disease recently caused a global outbreak and worldwide concern for all healthcare providers and patients. Ebola, however, is just the most recent example of the potential threat for pandemic infectious diseases having a global impact on the delivery of healthcare services globally. Previously, bloodborne pathogens were the primary concern for occupational risk and exposure, however this recent outbreak has highlighted the potential dangers to Vascular Access Clinicians.
During the crisis, there were many lessons learned, but most notably the importance of ongoing training about Personal Protective Equipment and its appropriate use in order to mitigate risk for occupational exposure for healthcare providers. Given that patients impacted by emergent infectious diseases will require vascular access therapy and support, we must adequately train, prepare, and protect Vascular Access clinicians against occupational exposures from infectioud diseases. This session will focus on the revised World Health Organization and Centers for Disease Control and Prevention evidence based recommendations for use of personal protective equipment, pandemic preparedness, and the role of collaboration across disciplines to protect the patient, the vascular access clinician, and the clinical environment of care.
P-038 DECONTAMINATION OF THE NEEDLELESS CONNECTOR: A DESCRIPTIVE REVIEW OF CURRENT LITERATURE
M. Flynn1, C. Rickard1, S. Keogh1, L. Zhang1
1Griffith University & RBWH, Brisbane, Australia; 1Griffith University, Brisbane, Australia
Aim: To evaluate and synthesise all relevant published peer reviewed quantitative studies on the decontamination of needleless connectors to assist researchers and healthcare decision makers inform practice.
Methods: Cinahl, Cochrane database of systematic reviews, JStor, Medline, Ovid, Pubmed, Science Direct, and Scopus were searched. The references of included studies were hand searched. The review included all current published research on needleless connector decontamination, with a primary outcome of central line associated bloodstream infection (CABSI) or, in the case of in vitro studies, bacterial contamination.
Inclusion criteria: The review considered primary research that:
Investigates adult, paediatric populations
RCTs, observational and in vitro studies
Analysed decontamination of the needleless connector
Had a primary outcome of CABSI, or bacterial contamination for in vitro studies
Original quantitative research
Exclusion criteria:
Studies that included a multi-modal approach to reducing CABSI.
Results: Eighteen papers were included in this review, four prospective clinical trials, seven pre-test/post-test studies and seven in vitro studies. Results of studies were difficult to compare due to the inconsistent reporting methods. Of the four prospective studies, two reported the number of participants (n = 77; n = 691), one reported in central line days (n = 361 central line days), with the final study reporting the number of stopcocks (n = 572).
Conclusions: This review highlights the importance of consistent reporting methods as well as the need for good quality randomised control trials in this area. Effective decontamination of the needleless connector is a simple yet undervalued component of minimising the introduction of microorganism into the needleless connector in an attempt to reduce CABSI.
P-039 COST-EFFECTIVENESS OF SAFETY ENGINEERED PERIPHERAL CATHETERS WITH AN INTEGRATED STABILIZATION PLATFORM UNDER THE PERSPECTIVE OF HOSPITALS IN BRAZIL
L.L. Mensor1, D. Giorgio1, C.P.R. Souza1
1Laboratórios B.Braun S.A., Rio De Janeiro, Brazil; 1Sense Company, São Paulo, Brazil
Introduction: Securement adverse reactions and peripheral intravenous restarts occur frequently in hospitalized patients. The current evaluation aims at determining the cost-effectiveness of a safety engineered peripheral catheter with an integrated stabilization platform and a multi-access septum during its use in patients admitted to hospitals and submitted to infusion therapy, under the perspective of Supplementary Healthcare in Brazil.
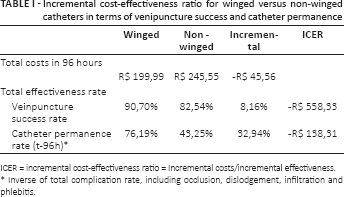
Methods: A decision tree was elaborated for estimating the incremental cost-effectiveness ratio (ICER) in short time horizon (96 hours) between safety engineered peripheral catheters with stabilization platform (winged catheters) and without platform (non-winged catheters), used during patients hospitalizations in Brazil.
Results: Clinical data applied to the model were the success rate in venipuncture (90,7% for winged catheters versus 82,2% for non-winged catheters, p = 0,036) and the odds for securement adverse reactions after venipuncture (16% with winged catheters versus 47,6% with non-winged catheters, p = 0,001). Outcomes were obtained from a systematic review of literature performed with scientific articles published internationally until 31.08.2015. The average of total direct medical costs for treatment of adverse events was 76,70 Brazilian Reais per peripheral intravenous restart and 98,07 Brazilian Reais per treatment of securement adverse reactions. Costs were estimated by expert opinion and pricing data was collected from secondary databases. The ICER results reflect cost-savings of 138,31 Brazilian Reais per avoided complications and 558,33 Brazilian Reais per peripheral intravenous restarts avoided.
Discussion and conclusions: Our study points out that safety engineered peripheral catheters with stabilization platforms (wings) integrated to the device constitutes feasible alternatives for Brazilian private hospitals. Its use can generate cost reductions and gains in effectiveness due to the lower tendencies for development of adverse reactions related to inadvertent mobilization of peripheral access over time.
Incremental cost-effectiveness ratio for winged versus non-winged catheters in terms of venipuncture success and catheter permanence
ICER = incremental cost-effectiveness ratio = Incremental costs/incremental effectiveness.
Inverse of total complication rate, including occlusion, dislodgement, infiltration and phlebitis.
Decision tree - Analitic decision model for cost-effectiveness estimation.
P-042 AUDIT OF 1000 CASES OF GROSHONG TIP PORT-A-CATH USING NOVEL TECHNIQUE UNDER LOCAL ANESTHESIA
S. Sampige Prasannakumar, P. Govindarajan
Manipal Hospital, Bangalore, India
Introduction: The most commonly used technique for chemoport insertion by most surgeons is Seldinger puncture technique. This utilizes blind puncturing of vein for catheter access and a separate incision for subcutaneous pocket for chamber. This technique carries risks of inadvertent arterial puncture, hematoma, pneumothorax, hemothorax, brachial plexus injuries and increased radiation exposure. These risks can be avoided by our novel technique of cephalic vein cut down. This audit explores this novel technique using Groshong tip catheter.
Methods: This audit includes 1000 patients over 9 years from a tertiary cancer care center in southern India. All patients underwent Groshong tip chemoport insertion using our novel cephalic vein cut down technique under local anesthesia. We use single incision for catheter and chamber placement. The common indications for chemoport insertion in our series were breast carcinoma, colorectal carcinoma, hematological malignancies and gynecological malignancies.
Results: We could access cephalic vein through this technique in 95% of cases. There were no immediate complications viz vascular injury, hematoma, and pneumothorax. In 5% of patients seldinger technique used as cephalic vein was too small for the catheter (n = 32) and absence of predominant cephalic vein with predominance of branching tiny venous tributaries within deltopectoral groove (n = 18). Sixteen cases developed port infection, among them 8 required chemoport removal remaining salvaged with antibiotic lock. The common organisms were Staphalococcus aureus (n = 8), Pseudomonas sp. (n = 4), and Ralstonia mannitolilytica (n = 4). Fifteen cases had recurrent seroma at the port site. Longterm patency maintained in 96% of the cases.
Conclusions: The main advantage is this technique can be done under local anesthesia with single incision. Direct visualization and catheter placement in cephalic vein makes procedure safe. Single fluoroscopic radiation exposure used to confirm the position of the catheter and no need of post procedure CXR to detect pulmonary complications. Groshong tip helps in longterm patency.
P-043 VENOUS PERIPHERAL LINES IN THE PEDIATRIC PATIENT: LONG VS SHORT
N. Ruiz, M. Delgado, M. D. Martín Ríos
Fundación Jiménez Díaz Hospital, Madrid, Spain
Introduction: We presented a pilot study evaluating the length of time of long devices (long venous peripheral lines) DPL (40/80 mm, 22 G) implanted with Seldinger technique vs the peripheral short devices (short venous peripheral lines) DPC (19/25 mm, 22-24 G) in pediatric patients in WoCoVA 2014 (Berlin). Today we can present the results obtained after the analysis of the total of the sample size, which has allowed us to obtain relevant results for improving the quality of our children care.
Methods: We have analyzed the results of a sample of 101 devices in patients that joined our unit with ages between 1 month and 18 years old, with a predictable need intravenous therapy equal or superior to 48 hours and no longer than 2 weeks. We have considered variables:
Independent: the different models of device, long and short.
Dependent: time, phlebitis, infiltrations and reasons of withdrawal of device.
Covariates: age, sex, pathology, canalized vein.
Results: The average length of the DPL was 4.76 (2.69) days against 2.62 (1.71) days for the DPC (P<0.0001). We appreciated infiltration by 16.83% of devices, a 2.0% on DPL and 32.0% DPC (P<0.0001). As for phlebitis we did not get significant differences: 13.7% in DPL compared to 22.0% in DPC (P = 0.277). 29.4% of DPL were removed for clinical causes, against 82.0% of the DPC (P<0.0001).
Discussion and conclusions: We have obtained results similar to adult studies previously published, or even better taking into account the limitations posed by the child, but our goal is not to show our experience, it is to find the better device that guarantees more length on time with minor complications.
The DPL have presented better results than the DPC in the pediatric patient.
P-044 CLOSING OF THE INCISION LINE WITH HISTOACRYL AFTER PLACEMENT OF IMPLANTABLE VENOUS ACCESS PORT
T.S. Seo, M.G. Song, S.O. Kim, J.S. Chae, H.W. Hyun, J.H. Kim
Korea University, College of Medicine, Guro Hospital, Seoul, South Korea
Introduction: Closing of the incision line with Histoacryl after placement of the implantable venous access port (IVAP) has advantages to take shower 24 hours after procedure and to reduce duration of wound dressing which may cause adhesive dermatitis and limitation of the daily life. The purpose of this study was to evaluate the feasibility and safety of the wound closing with Histoacryl.
Materials and methods: Between August 2014 and October 2015, IVAPs were placed in 456 patients at an interventional radiology suite and wound was closed with Histoacryl in 406 patients. They were 137 men and 269 women with a mean age of 55.9 years. Procedures were performed based on day care center and they visited out-patient department (OPD) of the radiology 1~3 days after procedure. At follow-up visiting, we evaluated the clot formation on wound due to polymerization of the Histoacryl by contact with blood from incision, oozing on gauze due to extruded blood from wound after polymerization, and complications. We retrospectively reviewed incidence wound infection within 1 month on medical record.
Results: All wound closing with Histoacryl were technically successful. Clot was formed in 16 patients (3.9%) and dried oozing was detected in 7 patients (1.7%). Complications were vesicle formation at margin of the Histoacryl film (n = 2) and wound dehiscence by untied knot of the suture after 2 days (n = 1). Vesicles were improved by conservative management and wound dehiscence was treated by one stitch of suture and closing with Histoacryl. All patients except 3 patients with complications did not need to revisit OPD. No wound infection was reported within 1 month.
Conclusions: Wound closing with Histoacryl after IVAP placement was feasible and safe method with high success rate and low complication rate and may improve life quality of the patients after placement of the IVAP.
P-045 ESTABLISHMENT OF PICC INSERTION FOR INFANTS AT ONE UNIVERSITY HOSPITAL IN JAPAN
R. Shirotsuki, H. Uchida, M. Kamei, A. Tanano, T. Tainaka, C. Shirota, A. Hinoki, K. Yokota, N. Murase, K. Ohshima, K. Chiba
Nagoya University Graduate School of Medicine, Nagoya, Japan
Introduction: Peripherally inserted central venous catheter (PICC) is widely used in many countries, with wide range of patients age. In Japan, PICC usage (<7% of central venous catheter; CVC) was more than 1/5 less than in USA (about 35% of CVC), because of low product awareness and less available catheters. Even in infants, PICC is better than CVC in many reasons; low risk in placement, infection resistance, reduce punctures of blood sampling and line placement, reduce patients discomfort and easy to remove. Thus, we try to insert PICC into infants' basilic vein of upper arm using ultrasound-echography guidance (US-guided) during perioperative setting.
Method and results: During 2014 October-2015 December, 9 infants (age range: 1.5-11.5 months, median 4.0 months) were inserted PICC for operation or neo-adjuvant chemotherapy with several devices (24G PI, 3.5 Fr polyurethane or 4Fr silicon catheter, depends on age and venous diameter). All insertions were US-guided with fluorography to confirm the tip of catheter by single pediatric surgeon under venous sedation or general anesthesia. There was no cases of incomplete insertion. Median of inserted days was 24 (9-180). Reason for removal were therapy complete 44% (4 cases), occlusion 44%(4 cases), suspect of infection 11%(1 case). There was no severe complication during insertion and inserted period.
Discussion: US-guided PICC insertions were safely performed even in infants. The big problem was a high occlusion rate, which might be lead by some reasons; thick and stiff catheter, drip line was easy to reflux, and medical staffs might be not-good at handling catheters. We should keep improving and broadening the handling technique and selecting devices (Ex; using continuous infusion pump, soft catheter and neutral pressure injection cap and etc.).
P-046 IDENTIFYING RISK FACTORS FOR PERIPHERAL INTRAVENOUS CATHETER FAILURE FROM A PROSPECTIVE COHORT STUDY OF 1000 PATIENTS
M. Marsh1, J. Webster1, E.N. Larsen1, M. Cooke1, M. Rickard1
1Griffith University, Brisbane, Australia; 1Royal Brisbane and Women's Hospital, Brisbane, Australia
Introduction: In acute care hospitals, up to 70% of patients will receive a peripheral intravenous catheter (PVC). As many as 40% of PVCs fail prior to the completion of therapy, causing distress for the patient and an economic burden for hospitals due to treatment delay and costs associated with re-siting. High rates of PVC failure, and subsequent catheter re-sites, necessitate a clearer understanding of the modifiable risk associated with catheter failure.
Methods: A single centre prospective cohort study was conducted in the medical/surgical wards of a large Queensland tertiary hospital between October 2014 and December 2015. Patients were eligible if they had been in hospital <24 hours. This study design allowed us to identify risk factors associated with PVC failure (defined as an unplanned catheter removal, not associated with completion of treatment).
Results: One thousand patients (1569 PVCs) were recruited to this study. PVCs dwelled for an average of 57 hours and the majority were inserted by medical staff (1275/1569). Device complications developed in 28.7% of PVCs. Of the first PVC per participant, occlusion (9.3%, p = 0.005), infiltration (11.2%, p = 0.02) and phlebitis (7.5%, p = 0.01) occurred more frequently in those with an infection at the time of device insertion. Higher occlusion rates were reported in participants with an extension tubing or 3-way connector (4.2%, P = <0.001) and dislodgement was more likely in patients with poor skin integrity (8.3%. p = 0.003).
Discussion: Our study confirms the high rate of catheter failure among patients admitted to acute care facilities. Identifying risk factors will aid in future education and PVC insertion skill development and may result in lower rates of PVC failure.
P-047 MICROBIAL BIOFILMS ASSOCIATED WITH INTRAVASCULAR CATHETER RELATED BLOODSTREAM INFECTIONS IN INTENSIVE CARE UNITS
L. Zhang1, C.M. Rickard1, J. Gowardman1, M. Morrison1, N. Runnegar1
1Griffith University, Brisbane, Australia; 1Royal Brisbane and Women's Hospital, Brisbane, Australia; 1The University of Queensland Diamantina Institute, Brisbane, Australia; 1Princess Alexandra Hospital, Brisbane, Australia
Background: Catheter Related-Bloodstream Infections (CRBSIs) are one of the most serious complications in hospitalized patients, leading to increased hospitalization, intensive care admissions, extensive antibiotic treatment and mortality. A greater understanding of these bacterial infections is needed to improve the prevention and the management of CRBSIs.
Methods: We describe here the systematic culture-independent evaluation of intravascular catheter (IVCs) bacteriology.
Results: Twelve IVCs (6 central venous catheters and 6 arterial catheters) were collected from 6 patients. Through traditional culture methods, three patients were diagnosed with catheter colonization including one patient who also had CRBSI, and three had no colonization. From a total of 839,539 high-quality sequence reads from high-throughput sequencing, 8 microbial phyla and 76 diverse microbial genera were detected. All IVCs examined in this study were colonized with complex microbial communities including ‘non-colonized IVCs’ as defined by traditional culture methods. Two main community types were observed: Enterobacteriaceae spp., dominant in patients without colonization or CRBSI; and Staphylococcus spp., dominant in patients with colonization and CRBSI.
Conclusions: More diverse pathogens and a higher microbial diversity were present on patients with IVC colonization and CRBSI. Community composition did not appear to be affected by patients' antibiotic treatment or IVC type. Characterization of these communities is the first step in elucidating roles of these pathogens in disease progression and to ultimately facilitate the improved prevention, refined diagnosis and management of CRBSI.
P-048 THE EFFECT OF USING INTRA-THECAL INTUBATION SHEATH TO MAKE A SKIN EXPANSION ON PREVENTING POST INSERTION BLOOD OOZING
Y. Wang1, X. Ma1
1Tianjin Medical University Cancer Hospital, Tianjin, China; 1 Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences, Tianjin, China
Objective: To explore the effect of using intra-thecal intubation sheath to make a skin expansion during the procedure of ultrasound guided PICC insertion on preventing post insertion bloodoozing from the insertion site for breast cancer patients.
Methods: One hundred breast cancer patients who needed PICC for their chemotherapy were recruited in the randomized controlled trial conducted in Tianjin Medical University Cancer Institute & Hospital, China. Fifty participants were assigned to the experimental group (using Intra-thecal intubation sheath to make a skin expansion), and the other half were assigned to the control group (using a scalpel to make a skin expansion). The data of total amount of blood oozing from the cut and the frequency of dressing-change were collected within 1 week from the date of the insertion in order to compare the effects of the two methods of skin expansion. T-tests and chi-square tests were used to analyze the data. p<0.05 was considered that the differences between the two groups were statistically significant.
Result: The total amount of blood oozing from the cut and the frequency of dressing-change were significantly lower in the experimental group than those in the control group (p<0.05).
Conclusions: This study showed a lower amount of blood oozing from the cut when intra-thecal intubation sheath was used for PICC insertion. This technique is value of clinic application for PICC insertion.
P-049 SUPERIOR SUCCESS RATE OF INTRACAVITARY ELECTROCARDIOGRAM GUIDANCE VERSUS ANATOMICAL LANDMARK FOR PERIPHERALLY INSERTED CENTRAL CATHETER PLACEMENT IN CANCER PATIENTS (EGG STUDY)
L. Yuan1, W. Xu1, P. Chen1, X. Wu1, Y. Yang1, A. Meng1, Z. Qiu1, M. Qin1, Y. Feng1, W. Kong1, J. Qi1, R. Li1
1Nanjing Drum Tower Hospital, Nanjing, China; 1The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China; 1Nanjing Hospital Affiliated to Nanjing Medical University, Nanjing, China; 1The First Affiliated Hospital of Suzhou University, Suzhou, China; 1Jiangsu Cancer Hospital, Nanjing, China; 1The Second Affiliated Hospital of Suzhou University, Suzhou, China; 1The People's Hospital Affiliated to Jiangsu University, Zhenjiang, China; 1Nanjing Jinling Hospital, Nanjing, China
Aims: To determine whether intracavitary electrocardiogram (IC ECG) guided peripherally inserted central catheter (PICC) provided more accurate positioning of catheter tip versus conventional anatomical landmark in cancer patients undergoing chemotherapy.
Methods: In the multicenter, open-abel, randomized controlled study (ClinicalTrials.gov number, NCT02409589), a total of 1,007 adult patients were assigned to receive either IC ECG guidance (n = 500) or anatomical landmark (n = 507) for PICC positioning. The confirmative x-ray data of catheter tip in the study were centrally read by independent radiologists. All reported analyses in overall population were performed on an intention-to-treat basis. Analyses of pre-specified subgroups and selected large subpopulation were conducted to explore consistency in accuracy.
Results: In the IC ECG guided group, the first-attempt success rate was 89.2% (95% Confidence Interval (CI), 86.5% to 91.9%), which was significantly higher than 77.4% (95% CI, 73.7% to 81.0%) in the anatomical landmark group (P<0.0001). This trend of superiority upon IC ECG guidance was consistently noted in almost all of the prespecified patient subgroups and selected two large subpopulations including using optimal target rate et al to measure. In contrast, the superiority nearly disappeared when PICCs were conducted via left instead of right arms (Interaction P value = 0.021). No any adverse events were reported during the PICCs procedure in either group.
Conclusions: Our findings indicated that this IC ECG guided method had favorable positioning accuracy versus traditional anatomical landmark for PICCs in adult cancer patients undergoing chemotherapy. Also there is no safety concern reported during the catheterization.
P-050 EXPERIENCES USING THE SHERLOCK TIP CONFIRMATION SYSTEM FOR PERIPHERALLY INSERTED CENTRAL CATHETERS
T.Q. Santolim
Institute of Orthopedics and Traumatology at Clinics Hospital of School of Medicine, São Paulo, Brazil
Introduction: The Peripherally Inserted Central Catheters (PICCs) are great allies in the treatment of patients with orthopedic infections, due to the lengthy treatments and aggressiveness towards the vascular system (antibiotics with extreme pH and osmolarity). Because of this, the use of PICCs has grown after one year of usage within our institution. Since no other institutions in Brazil use the Sherlock tip confirmation system (TCS) for PICCs, we study it in our institution with the objective of offering more safety to the patients with the indication of using PICCs. With this we looked for adequate position of the catheters, since our error of positioning index was of 25% using the traditional technique. Also, we dismissed the use of an x-ray to confirm the position of the catheter after the procedure.
Methods: We inserted 20 PICCs using the Sherlock TCS. Three nurses were selected for the procedures: two nurses inserted seven PICCs each and the third nurse inserted six. After inserting the PICCs, all the patients were x-rayed to confirm the correct positioning of the catheter. Adequate positioning was considered when the catheter was located in the medial third of the superior vena cava or in the atrial cava junction.
Results: Out of all the PICCs inserted, 98% had adequate positioning using the Sherlock TCS.
Discussion and conclusions: From the results obtained, we consider the Sherlock TCS as efficient equipment for the positioning of the PICCs. We found the inserting technique easy, allowing the immediate use of the catheter after the insertion, dispensing the use of a control x-ray for evaluating the position of the catheter inserted.
P-051 APPLICATION OF QUALITY INDICATORS FROM THE NURSING STAFF FOR EVALUATING THE SECURITY IN INFUSION THERAPY PROCEDURES
V.C. Dias
Institute of Orthopedics and Traumatology, São Paulo, Brazil
Introduction: The quality indicators used by the nursing staff, are important for measuring the quality of the care given to patients. This institution uses and measures indicators such as phlebitis, lost of peripherally inserted central catheters (PICCs) and of central venous catheters (CVCs). These indicators show unintentional harm that affects the patients' security. We established indicators that provide greater security in the infusion therapy procedures, with the objective of measuring the quality of the attention given by the nursing staff.
Methods: The collection of these indicators was done in the hospitalization wards, emergency room (ER) and intensive care unit (ICU). The data was collected monthly using indicator charts that show the level of quality of each unit analyzed. In the venous access indicator, the items studied were: the filling out of the control form and the nursing prescription of the care of the intravenous therapy. In solution container label indicator, we analyzed: name of the patient, hospital record number, date of birth, medication, dosage, time of administration, time of infusion and the name and signature of the professional responsible for applying the medication.
Results: The results showed improvement in the percentage of the venous access indicator in two units, between March and May 2015. In the hospitalization ward, the percentages were: 45%, 72% and 70% respectively. The ICU had 100% in every month measured. In the identification of the container of continued or intermittent intravenous saline infusion indicator, the percentages in the hospitalization ward were of 85%, 34% and 70%; and in the ICU were of 0%, 66% and 71%. The results showed no improvement in any of the indicators for the ER.
Discussion and conclusions: Based on the results, we can evaluate the quality of the attention and propose actions to improve it.
P-052 EFFECT OF DIFFERENT IMPLANTABLE VASCULAR ACCESSES TYPE ON CANCER PATIENTS PSYCHOLOGICAL DISTRESS
S. Bertoglio1, B. Faccini1, D. Russo1
1University of Genova, Genova, Italy; 1IRCCS San Martino-IST, Genova, Italy
Introduction: Assessment of psychological distress on cancer patients bearing TIVADs or PICCs for chemotherapy delivery was performed at the end of treatment before the device removal.
Methods: One hundred forty-nine patients were investigated by means of a questionnaire related to perceived patient's satisfaction, interference with daily lifestyle, interpersonal relationships and perceived body image. Responses were scored from 1 (excellent) to 4 (unaxeptable). Moreover patient where asked about their position with respect to a posibble re-use of a similar device. Study population: TIVADs were 114 (76.5%) and PICCs 35 (23.5%). Fourty patients were males (26.8%) and 109 (73.2%) were females equally represented among the two different devices.
Results: Up to 89% of patients declared satisfaction with the implanted device. For TIVADs we obtained scores 1-2 in all patients, opposite to PICCs where this result was observed only in 80% of patients. There was no difference on interference with daily lifestyle, up to 75% of patients declared no interference for TIVADs and PICCs, both; the remaining 25% of patients declared minimal interference (scores 2 -3) equally represented for the two devices. Concerning interpersonal relationships and perceived body image no interference was observed in 91.5% of PICC opposite to 75.5% of TIVAD. The latest ones declared elevated versus unacceptable interference in 5% of cases and none for PICC ones. Nevertheless quite the majority of TIVAD patients (88%) would accept a re-use of this device in case of necessity while only 71% of PICC group would re-use a PICC.
Discussion and conclusions: The two implantable vascular devices for chemotherapy delivery where well accepted with minor interferences on psychological distress. TIVADs had a slightly higher interference with interpersonal relationships and body image. PICCs induced a higher level of anxiety related to a perceived necessity of a major knowledge of the management of the external hub and its maintenance protocols.
P-053 MIDLINE CATHETER ULTRASOUND-GUIDED IMPLANTED IN HOSPITALIZED PATIENTS
M. Montealegre, M.A. Cubero, S. Varga, M. Rodriguez, P. Gallardo, A. Chato, J. Gonzalez
Hospital Clinico San Carlos, Madrid, Spain
Introduction: Hospitalized patient requiring intravenous therapy frequently have problems associated with central venous catheters (CVC) and/or peripheral venous catheters (PVC).
The Medial Venous Catheter (MVC) or Midline is a safe and efficient device for intravenous treatment increasingly used.
Methods: We perform a prospective observational study in order to evaluate the impact of MVC use, implanted with Seldinger ultrasound-guide technique.
During 2014-2015, admitted adult patients in Hospital Clínico San Carlos requiring peripheral intravenous treatment more than six days and/or patients with difficult venous access were included. Principal variables of the study were demographic and disease-related characteristics of the population, number of venipuncture and intravenous treatment type.
Results: The IV Team implanted 616 MVC. The main reason for insertion was poor vascular access (78%). The principal referral units into the hospital were: Internal Medicine (42.7%), Medical Oncology (12.7%).
The more frequent locations of insertion were upper right arm (67.7%), basilica vein (82.14%), cephalic (5.84%) and brachial (12.01%).
In the 72.70% of the subjects the canalization was successful at the first attempt.
The median duration of catheter implantation was 8 days. The principal reasons for the removal were end of treatment (49.83%), death (18.66%), accidental extraction (13.5%), obstruction (3.9%), replacement by another catheter type (6.16%), and phlebitis (1.13%).
Discussion and conclusions: The use of ultrasound in the vascular access setting has changed the landscape for the patients. This technique allows visualizing vascular structures avoiding complications.
MVC insertion is a opportunity that meets the needs of the patient, minimizing secondary problems associated with the use of CVC. These catheters are an alternative to short PVC and are useful in hospitalized patients with vascular depletion or intravenous treatment.
The combination of ultrasound and MVC, despite of its limitations, is a nursing tool for improve the quality of life and safety of our patients.
P-054 THE USE OF MANAGEMENT TOOLS IN THE ANALYSIS OF PROBLEMS RELATED TO INTRAVENOUS THERAPY
T.Q. Santolim, V.C. Dias, M.M. Giovani
Institute of Orthopedics and Traumatology at Clinics Hospital of School of Medicine, São Paulo, Brazil
Introduction: The process of administrating medications is complex and requires attention from the nursing staff in order to complete all the steps in the procedure. Not completing one of the steps can lead to serious or fatal mistakes towards the patient. Errors can occur as a consequence of not following protocols, carelessness and negligence or due to a flaw in the process that leads the professional into committing the mistake. Whenever an error occurs, measures must be taken in order to avoid it from happening again. Understanding the situation is fundamental. Several times when analyzing a situation we are influenced by past experiences or by the relationships within the staff involved in the situation, which is why it is important to use tools that aid in the understanding of the problem and its possible causes.
Methods: Two management tools were used to analyze two problems related to intravenous therapy. Both, the brainstorming and the Ishikawa diagram were applied for the analysis of the following events: obstruction of seven peripherally inserted central catheters (PICCs) within a timeframe of one month, and phlebitis after the infusion of intravenous levofloxacin.
Results: Possible causes were analyzed in both situations. The advantage of using the management tools was the possibility of bringing forward the causes that produced these events, as well as the fragilities in the process that were until then unidentified because they hadn't yet led to errors. From this data analysis, plans of action were made so that these events wouldn't happen again, as well as a revision of all of the maintenance process of the PICCs and intravenous infusion of antibiotics.
Discussion and conclusions: The use of management tools are great allies to identifying problems related with the assistance given by the nursing staff and should be used and widely spread.
P-055 PICC INSERTION WITH TUNNELING ON ARM WITHOUT THE NEED FOR EXTRA OPENING: REPORT OF THREE CASES
1PVP Medical Services, Sao Paulo, Brazil; 1SESV Especialized Vascular Solutions, Sao Paulo, Brazil
Introduction: Among PICC placement candidates, some patients have no adequate vein caliber in the green zone (area of the arm corresponding to lower risk of infection). This paper attempts to report the experience of 3 cases of PICC placement with direct tunneling without the need for auxiliary skin opening, with a 3 to 5 cm spacing of venous puncture site in relation to the skin exit site.
Methods: Patients who received PICC placement indication, and did not show basilica or brachial veins with appropriate caliber at the sonographic evaluation, were selected for catheter placement with small tunneling made directly with the puncture needle, guided by ultrasound on the long axis. Thus, despite the axillary vein puncture, there was a considerable distance from the skin insertion ostium related to wet axillary region.
Results: In all three cases there was no infection related to the puncture site or puncture accident. All catheters were used until the end of proposed therapies (10, 14, and 14 days).
Conclusions: The direct tunneling is feasible and safe in selected cases. Comprehensive studies are necessary to determine in which cases auxiliary incision will be required for tunneling PICC on arm.
P-056 PERIPHERALLY INSERTED CENTRAL CATHETER ASSOCIATED COMPLICATIONS: A REMARKABLY LOW INCIDENCE OF MAJOR COMPLICATIONS IN A NURSE-LED VASCULAR ACCESS PROGRAM
S.A. McDiarmid1, N.S. Scrivens1, E.S. Sabri1
1The Ottawa Hospital, Ottawa, Canada; 1Ottawa Hospital Research Institute, Ottawa, Canada
Background: Although peripherally inserted central catheters (PICCs) provide enormous benefit to patients requiring prolonged intravenous therapies, they are associated with a number of complications of varying severity. The use of standardized protocols, advanced catheter technology, experienced staff inserting high volumes can minimize complications.
Methods: We performed a retrospective analysis of 656 PICCs (436 single and 220 dual lumen catheters) made with the Endexo polymer. These catheters were randomly selected from a diverse cohort (inpatient and outpatient) of 8431 PICCs placed at The Ottawa Hospital from January 1st, 2013 to December 31st, 2014. The cumulative incidence of major complications (catheter-related bloodstream infections [CRBSI] catheter- related deep vein thrombosis [CR-DVT]) and less serious complications (occlusion, use of thrombolytics and catheter migration) were measured.
Results: The total number of catheter days for the 656 PICCs analyzed was 58,834 with a median dwell time of 45 days. The cumulative incidence of CRBSIs was 0.76% (95% confidence interval [CI], 0.3-1.8%). The overall rate for CRBSI was 0.08 per 1000 catheter days. The cumulative incidence of DVT was 2.29% (95% CI, 0.78-3.79%). Less serious complications included: complete catheter occlusions 7.47% (95% CI, 4.82-10.12%); withdrawal occlusions 12.35% (95% CI, 9.03-15.66%); use of thrombolytics 21.95% (95% CI, 17.78-26.12%); migrations 11.13% (95% CI, 7.96-14.30%).
Conclusions: Compared to a recent meta-analysis published in the Lancet (2013), we found a remarkably low incidence of major complications in these long indwelling catheters. The cumulative incidence of DVT was 2.29% and of CRBSI 0.76%. We attribute this low incidence to an experienced RN insertion team, standardized care and maintenance protocols, high insertion volumes, novel catheter material, and the continuous quality improvement initiatives we regularly implement and evaluate.
We conclude that the considerable benefits that PICCs provide to patients are attained with a very low risk of major complications.
Funding: AngioDynamics.
P-057 SAFETY AND EFFICACY OF ECG-GUIDANCE AND MAGNETIC TRACKING FOR TIP POSITIONING OF PICC-LINES: A RANDOMIZED CONTROLLED STUDY
H. Habrecht, V. Mack, S. Romankiewicz, A. Malouhi, F. Bürckenmeyer, U. Teichgräber, R. Aschenbach
Friedrich Schiller Universtiy Hospital, Jena, Germany
Introduction: Correct tip positioning in CVC is of major importance as malpositioning is associated with a high risk of complications. The aim of this study is to assess the safety and efficacy of an integrated magnetic tracking and ECG-guided tip location system vs. fluoroscopy in implantation of peripherally inserted central venous catheters (Power-PICC-Line).
Methods: A randomized controlled non-inferiority monocentric study in adults including 210 patients (105 per arm) comparing fluoroscopy and an integrated magnetic tracking and ECG-guided tip location system (SHERLOCK 3CG) in implantation Power-PICC-lines is planned to start in February 2016. A recruitment period of 12 months is intended. Tip location will be retrospectively determined radiographically by chest X-ray while correct tip location is defined by two vertebral bodies below the carina including an area of 3 cm above this marking line.
Results: According to previous studies it is expected that this method will be as accurate, safe and feasible as fluoroscopy for positioning the tip of peripherally inserted central venous catheters in adult patients. Furthermore it could be even cost and time saving.
Discussion and conclusions: Sherlock tip location system is a promising method as it combines magnetic tracking and ECG-guidance in tip positioning of PICC-Lines. Limitations might be the restricted applicability in patients with non-existing sinus rhythm and in patients with pace makers. Furthermore catheter malpositioning cannot be traced and documented with ECG and magnetic tracking alone and final X-ray after insertion will still be mandatory.
P-059 STANDARDIZED CENTRAL VENOUS ACCESS INSERTION EDUCATION: MEASURING PRACTICE, CHANGE AND LIMITATIONS
R. Spencer1, J. Bardin1
1Tim Spencer, Sussex Inlet, Australia; 1Teleflex, Raleigh-Durham, NC, USA
Advancing the vascular access specialty is a rapidly growing trend, one that requires additional education to develop this dynamic discipline. This simulated, hands-on program is intended to enhance knowledge, skill and procedural confidence across multi-disciplinary groups. Advancing healthcare professionals to include central venous catheter (CVC) insertion empowers clinicians to assess the vascular access needs of patients and insert the most appropriate device, based on intended therapy and full assessment of the vasculature, adding a valuable resource to their organization without added costs, risk, or delays in care.
To measure healthcare professionals procedural confidence and ability to advance their individual scope of practice after attending standardized ultrasound-guided central venous catheter insertion training.
To survey multi-disciplinary clinicians that attended a standardized ultrasound-guided CVC education program and measure CVC procedural confidence through pre- and post-course surveys. This project measured the number of courses and attendees, clinician type, number of catheters inserted prior to the course, procedural confidence, and the relationship between CVC program satisfaction and collegial education recommendation.
P-060 LOW APPROACH INTERNAL JUGULAR CENTRAL VENOUS CATHETERS: OPTIMIZING CATHETER PERFORMANCE AND PATIENT EXPERIENCE
R. Spencer1, J. Bardin1
1Tim Spencer, Sussex Inlet, Australia; 1Teleflex, Raleigh-Durham, NC, USA
An increase in internal jugular (IJ) catheter placement has been identified with the increased use of ultrasound technology for central venous catheter insertion. This site is often selected for ease of use and accessibility, but has limitations to care and maintenance due to exit site management and natural downward gravity when the catheter is positioned high on the neck. This high internal jugular position renders poor patient satisfaction and requires unscheduled dressing changes due to poor adherence of the dressing or securement device.
A survey of ten vascular access clinicians who currently insert IJ polyurethane type catheters was performed. This survey identified the percentage of time a low approach is utilized for insertion, overall catheter performance, dressing adherence, patient satisfaction and overall securement method.
To demonstrate safe and efficient low approach IJ insertion allowing adequate catheter securement and dressing maintenance when positioned over the clavicle on the respective insertion side.
P-061 ARTERIAL CATHETERIZATION: A SURVEY OF CURRENT CLINICAL PRACTICE
R. Spencer1, J. Bardin1
1Tim Spencer, Sussex Inlet, Australia; 1Teleflex, Raleigh-Durham, NC, USA
Arterial catheters are routinely placed by multiple disciplines within an organization. These catheters have both significant benefits and risks to critically ill patients. Recent evidence demonstrates need for a standardized approach to arterial catheter insertion and maintenance to reduce procedural and dwell-associated risks to this patient group.
To demonstrate the variance to procedural guidelines for arterial catheter insertion and maintenance, comparing current practices identified to best practice recommendations.
A survey of current active AVA members on arterial catheter insertion and maintenance practices was distributed electronically. 22 questions defining local clinical practices and potential variances based upon empirical published clinical guidelines were compared.
These guidelines were the currently quoted supportive literature based on recommendations from the Centers for Disease Control (CDC), Infusion Nurses Society (INS), Society for Healthcare Epidemiology of America/Infectious Diseases Society of America (SHEA/IDSA) and Joint Commission on Accreditation of Healthcare Organizations (JCAHO).
The survey also questioned the opportunity to add arterial catheters to current vascular access teams, in addition to identify what percentage of vascular access specialists are inserting or wanting to add arterial catheter insertion to their practice.
P-062 SWINE STUDY SHOWS NO INTRAMEDULLARY EFFECTS OF POWER-INJECTED CONTRAST MEDIA USING INTRAOSSEOUS ACCESS
T.A. Puga, D.F. Montez, C. Dgvlgntes, L.J. Miller, T.E. Philbeck
Teleflex Medical, San Antonio, USA
Introduction: For difficult vascular access patients, intraosseous (IO) access is an option. A preclinical study was conducted to examine the immediate effects of power-injected contrast media through the IO route on the medullary cavity and marrow in mature swine.
Methods: IO access was established bilaterally in the proximal humeri of anesthetized swine. One proximal humerus received power injection of 150 ml of contrast media at 5 ml/second. The contralateral limb served as the control. Both humeri were flushed with 10 ml of saline post-contrast injection. After euthanization, limbs were amputated superior to the IO insertion site with the needle left in-situ, and cross sections of the bone were cut. The pathologist, blinded to which limb received contrast, examined specimens to identify cellular/structural damage to the injection site. Sections were graded for physical differences including hematopoetic bone marrow wash-out, intact stroma/fat, hemorrhage, presence of trabeculae, and cortical thickness.
Results: For seven matched humeri-pairs, the mean maximum infusion-pressure was 80psi (range 61-95). Marrow wash-out varied by one degree or less for each pig when limbs were compared. Amount of trabecular fracture caused by the placement of the IO needle could not be histologically separated from possible loss of trabecula due to high pressure power-infusion of contrast. Six samples had some degree of hemorrhage in one level, graded: same in 4 swine, +1 in the limb without injection for swine B, and +2 for one level in injected limb for swine F. Two swine showed small extraosseal extravasations.
Discussion and conclusions: In limbs receiving and not-receiving power-injected contrast, there was no histological difference examined post-infusion. This supports the safety of IO power-infusion of CT contrast. When considered with previous studies demonstrating CT image adequacy after IO contrast administration, these findings may further support the utility of power-injected contrast delivered via the IO route.
P-063 PICC INSERTION VIA FEMORAL VEIN AT MID-THIGH FOR PATIENTS WITH SUPERIOR VENA CAVA SYNDROME
L.F. Zhao, X.Z. Cao
Sir Run Run Show Hospital, Hang Zhou, China
Introduction: Usually, PICC is inserted in the upper limb and the tip is located at the SVC. However, some patients with any condition that leads to obstruction of blood flow through the SVC accompany superior vena cava syndrome (SVCS). Obstruction can be caused by invasion or external compression of the SVC by an adjacent pathologic process involving the right lung, lymph nodes, and other mediastinal structures, or by thrombosis of blood within the SVC. At the same time these patients require central venous catheter due to the treatment needs. If the catheter is inserted via the femoral vein at inguinal area (traditional area), it is uncomfortable for activity, also the catheter will fracture easier. It is potentially contaminated because of the proximity of the perineal area, also difficult to clean the skin and stabilization. There are more complications such as thrombosis and infections, etc. We explore the feasibility of inserting PICC through femoral vein at mid-thigh for patients with superior vena cava syndrome.
Methods: We selected mid-thigh femoral vein for PICC insertion, we used ultrasound machine to guild, and combined with the modified Seldinger technique. A 4F, single-lumen catheter manufactured by BARD was used. The tip of the catheter is located at the IVC (L2-L3).
Results: 14 patients (9 males, 5 females) were inserted PICC in 2015, technical feasibility is 100%, one catheter has been kept for 316 days, the average catheter day was 121.61 ± 89.14, there is no complications such as thrombosis and infection, and the patient can do normal activity such as walking.
Conclusions: The femoral vein at mid-thigh is another opition to insert PICC. Patients can walk freely with this catheter, it can easily be fixed, and also reduces the risk of infections, it is a safe access for those special patients with SVCS.
Decubitus.
Erect position.
P-064 EXPERIENCE WITH SIDEWISE IMPLANTED CHEST PORT SYSTEMS: EFFICACY AND IMPLANTATION TECHNIQUE
Introduction: The sidewise implanted port catheter system represents an alternative for rapid, secure and easy port implantation. The aim of the study is to access the efficacy and complication rates of this novel sidewise implanted port systems.
Methods: In this retrospective study 50 patients who received a sidewise implanted port system (B.Braun, Celsite discrete) since January 2015 are evaluated. As outcome parameter the periprocedural, early and late complication rates are assessed. With reference to the catheter tip location the dislocation, catheter occlusion and dysfunction rates are analysed.
Results: No pneumothorax, massive hematoma or perforation of heart or vessels is detected. Overall 3 infections occurred, one as early complication (24 days after implantation) and two as a late infection (more than 4 weeks after implantation) with consecutive port explantation. One port system was loose with increased subcutaneous mobility and one was disconnected.
Conclusions: The sidewise implanted port catheter systems are a time saving and secure method with approximately equal risk to the conventional transversely implantation procedure with reference to infection rates, disconnection and dislocation.
P-065 INCATIV PLATFORM: A NEW MANAGEMENT TOOL TO EVALUATE THE CARE AND MAINTENANCE OF IV CATHETERS. A PILOT STUDY
S.C. Casanova-Vivas
Public Health Department - GVA, Valencia, Spain
Introduction: 78% of patients included in the INCATIV (Intravenous Therapy Quality Indicators) programme in the Valencian Community have received intravenous therapy (IV) during their stay in hospital. Infusion therapy is the most common procedure performed by hospital nurses. INCATIV study's main results demonstrated the efficacy of teaching interventions regarding the level of compliance with the IV therapy Protocol. However, they showed a wide variability of care standards between hospitals. The aim of this pilot study is to validate the INCATIV Platform using a new case report form (CRF) and a current innovative INCATIV score.
Methods: A cross-section pilot study will be undertaken in 4 hospitals in the Valencian Community. Data will be collected without any previous teaching by trained observers. Hospitals are classified according to their typology. The inclusion criteria are those patients admitted for more than 24 hours with IV therapy. New variables like type of infusion, catheter access protector and open/closed IV system have been added. After the first cross-section, we will conduct a teaching intervention with all IV nurses prior to a second cross-section.
Results: Data will be introduced in the new platform by each hospital and the different hospital results charts will show online in real time, allowing comparisons among hospital groups. Type of dressing, phlebitis rate and INCATIV score will be shown in evolutive charts. Analysis of variance will be used to assess the impact of training in the INCATIV score.
Discussion and conclusions: These results will help to validate the new management tool and to join all public hospitals of the Valencian Community to be audited. Relevant variables such as closed vs open systems as well as information about IV devices used, could be studied in depth opening new research to evaluate and measure the quality of patient safety in IV therapy nursing care.
P-066 ARE THERE SAVINGS TO BE MADE BY INTRODUCING AN ADVANCED SECUREMENT PERIPHERAL IV DRESSING INTO AN ACUTE NHS TRUST?
B.A. Day1, S. Foster1
1Derby Teaching Hospitals NHS Foundation Trust, Derby, UK; 13M, UK
Objective: To understand the total cost of upgrading from standard peripheral cannula film dressings to Advanced Securement dressing (ASD).
Introduction: Peripheral venous cannulas are a frequently used invasive medical device, failure prior to completion of therapy can occur in 69%. Caused by accidental removal from inadequate device securement or partial dislodgement leading to fluid leakage.
Methods: Purchasing data was used to compare two periods of product usage. Period 1 (Q4 2013/14) PVC securement was by standard film dressings, in period 2 (Q4 2014/15) ASDs were used. Increased patient admissions in period 2 required adjustment to the second period data to ensure meaningful comparison. Total costs were calculated upon: staff time (15 minutes of Band 2 support worker), dressings (£0.40p for standard film and £0.49 for ASD), extension set and cannula (£1.36) and other supplies (£0.46).
Results: Dressing use decreased by 3.5% in period 2, total costs reduced by £35,160 including 626 hours of staff time. Nursing and support worker time was saved due to reduction in cannula dislodgments. Patients received IV therapy in a timely fashion and less trauma from cannulas being re-sited.
Discussion: Cost pressures have led to cheaper alternatives, often masking the overall cost. Jackson et al indicated dislodgements of 36% with standard film dressings which significantly impacts total cost. It is important to consider this when selecting dressings for PVCs.
Conclusions: Using product usage data is a pragmatic method of calculating the true cost of IV securement. Introduction of the Advanced IV Securement Dressing led to overall savings to the Trust.
P-067 ‘SKINVASION’: AN IN VITRO MODEL FOR TRANSCUTANEOUS EXIT SITE INFECTIONS FOR THE ANALYSIS OF BACTERIAL INVASION THROUGH THE SKIN
E.N. Sowa-Söhle1, N. Moraw1, G. Marsch1, A. Weiss1, H. Wiegel1, N. Kachel1, T. Riemann1, A. Loos1, A. Haverich1
Introduction: Different catheter modifications and surface coatings have been developed to overcome bacterial infections of indwelling medical devices. So far there are no adequate in vitro test methods to investigate transcutaneous exit site infections. Therefore, to test the antibacterial behavior of these devices in vivo animal experiments are required. For animal welfare we developed “SkINvasion” as in vitro model for the testing of catheters.
Methods: We compared two catheter materials (antibacterial surface modification and control) for their antibacterial properties. The catheters were inserted into tubes filled with tryptone-soy-broth-agar. The external part of the catheter, mimicking a transcutaneous exit site, was infected with S. epidermidis and monitored for biofilm growth for up to 30 days. In parallel, animal experiments with infected subcutaneously implanted catheter materials were performed. Bacterial growth was monitored after 7 days.
Results: With this in vitro model we showed significant differences of biofilm growth between antibacterial and control catheter, which are comparable to the in vivo results.
Discussion and conclusions: Our results show that the in vitro “SkINvasion” model can be used to anticipate the antibacterial properties of catheters and can be used for screening of new materials and modifications of medical devices reducing animal experiments.
P-068 THE INFLUENCE OF A PERIPHERAL INTRAVENOUS CATHETER ON THE VEIN AND SUBCUTANEOUS TISSUE
R. Murayama1, H. Tanabe1, K. Yabunaka1, M. Oe1, C. Komiyama1, H. Sanada1
1The University of Tokyo, Tokyo, Japan; 1The University of Tokyo Hospital, Tokyo, Japan
Introduction: This observational study aimed to clarify the relationship between indwelling peripheral venous catheters (PIVCs) and their impact on the vein or subcutaneous tissue using ultrasonography (US) images. In addition, this study explored the risk factors associated with changes of the vein or subcutaneous tissue.
Methods: Data was obtained, after the placement of an indwelling catheter with heparin lock, before initial infusion, and immediately before the catheter removal. US examination was performed at bedside by one researcher in a medical ward of a university hospital in Tokyo, Japan. Characteristics of the PIVC placement and the patients, including blood test data which had been obtained most recently before the placement of indwelling catheters, were recorded. This study was approved by the Research Ethics Committee of the Graduate School of Medicine at the University of Tokyo (#10348).
Results: Thirty PIVCs from 28 patients (median age being 69 years old) were observed immediately after the placement of indwelling catheters and before the initial infusion. The duration of an intravenous lock time (median) was 930 minutes. Thrombus was observed in 8 (26.7%), and subcutaneous edema was observed in 2 (6.7%) of 30 US images before the initial infusion. Furthermore, all catheters (except dropouts) observed with thrombus before the initial infusion were also observed with thrombus immediately before catheter removal. Serum albumin lower than the median, and C-reactive protein higher than the median, were significantly associated with thrombus formation.
Discussion and conclusions: The intravenous lock may be associated with thrombus formation in the blood vessel. Furthermore, if there is thrombus before initial infusion, thrombus formation may occur easily. It was suggested that lower serum albumin and higher C-reactive protein may promote subsequent thrombus formation. Healthcare providers need to obtain information of patients' characteristics, including blood test data, and should consider the timing of catheterization.
Vessel diameter was defined as D (D = [major axis + minor axis]/2). The major axis was the longest diameter. The minor axis was perpendicular to the major axis.
Blood test results were classified into two categories based on the median: C-reactive protein (>0.07 mg/dL, ≤0.07), Albumin (>3.8g/dL, ≤3.8), Platelet (>19.7 × 101 μl, ≤19.7 × 101).
Mann-Whitney U test,
Fisher's exact test.
Ultrasonography findings of blood vessel, subcutaneous tissue, and peripheral intravenous catheter placement (a longitudinal image). Case: 81 years old, male, forearm. (A) After an indwelling catheter (Surflo V3®) was placed; (B) 17 hours (before infusion); (C) 42 hours (before catheter removal). Ultrasonography images showing the vessel wall (arrowheads), peripheral intravenous catheter tip (arrows), thrombus (circle), and subcutaneous edema (broken line circle).
P-069 IMPACT OF SHOWERPATCH AVAILABILITY FOR PATIENTS WITH INTRAVENOUS CATHETERS (ISIC): A RANDOMIZED CROSSOVER STUDY
M. Jérôme, G.A. Goossens, M. Stas
University Hospitals Leuven, Leuven, Belgium
Introduction: For patients with a long-term venous access is showering with this percutaneous catheter often prohibited due to the infection risk if the insertion site becomes wet. For patients with a catheter connected to an infusion line, this is even more difficult. Washing themselves is often impossible without assistance of a nurse or another person.
A newly developed protection tool, the Bedalpatch® (Bedal bvba, Belgium), is a device provided with a slit for the infusion administration set that completely covers the catheter dressing. Therefore it safeguards the insertion site of an intravenous catheter from water during bathing and showering activities. Patients can protect their vascular catheter themselves and they are no longer dependent on the availability of a caregiver.
The goal of the study is to compare the autonomy of patients with an intravenous catheter in situ, regarding their bathing activities when using the Bedalpatch® or just taking standard precaution measures.
Methods: This randomized study is conducted at the University Hospitals in Leuven, Belgium, registered at Clinical Trials.gov (NCT02324868). We anticipate to include 50 patients with a maximum observation follow up period of 8 weeks. The study time will be divided in two equal periods. Patients are randomized to start data collection with or without the Bedalpatch®. The primary endpoint is the patient's autonomy regarding bathing activities, weekly measured by a new-developed self-report scale. Secondary endpoints are the number and type of bathing activities, the status of the catheter dressing, the material used for catheter care, the time needed from the eventual caregiver and the incidence of catheter-related bloodstream infections and insertion site infections.
Results: Completion of data collection is anticipated by the end of February 2016 and results will be presented.
Discussion and conclusions: The results will be discussed.
P-070 ROLE PLAY IN THE DEVELOPMENT OF COMMUNICATION SKILLS IN OBTAINING INFORMED CONSENT FOR THE PERIPHERAL INSERTED CENTRAL CATHETER
C.S.C. Klippel, A.M. La Cava, R.A.C. Amorim, G.M. de Faria, S.M. Pinho
Novare, Rio de Janeiro, Brazil
Introduction: In Brazil, according to the Federal Nursing Council Resolution n1 258/2001, it is required to perform the nurse training course for management of PICC, to be considered able to perform the procedure safely. During the practical activities of a course held in a hospital, the nurses reffered to have difficulty in obtaining informed consent for the procedure, since this step involves technical, ethical and legal aspects. The objective of this study was to report the experience of the use of role play to develop communication skills in order to obtain informed consent for the insertion of the PICC.
Methodology: This is an experience report, carried out in a hospital in the city of Rio de Janeiro. The students were asked to act as actors playing the roles of nurse, patient and family, according to clinical cases, using the role play technique.
Results: Twenty eight nurses took part in the study. Among them, 75.6% reported that after the experience of the role play, they felt safer to handle similar situations in the workplace. 18% reported difficulties to argument, with the patient's relatives. Only 6.4% reported not feel comfortable for interpersonal approach with patients and their relatives.
Discussion: The authorization for insertion of PICC is the first step after the indication for the procedure. In order to get it, the nurse must present good communication skills, technical knowledge and attitude, to answer the questions of patients and relatives.
Conclusions: The role play technique contributed to the development of communication skills, giving the nurses arguments fto obtain the consent for the insertion of the PICC, enabling nurses to safe and humane approach.
P-071 EFFECTIVE INTERVENTIONS TO REDUCE BLOODSTREAM INFECTIONS IN A HEMODIALYSIS UNIT IN BRAZIL - THE CHALLENGE CONTINUES
R.D. Lobo, C.L. Luders, G.S. Dias, E.G. Gabriel
Hospital Sirio Libanes, Sao Paulo, Brazil
Introduction: Patients undergoing hemodialysis are a high-risk population for bloodstream infections (BSI), preventing these infections is a priority for hospital's staff and administration. Despite of low BSI's rates (0.8-1000 CVC-day) recorded in our institution, a private teaching hospital, we conducted an intervention study to further reduce those rates.
Methods: The quasi-experimental study was conducted in a hemodialysis unit where 15 hemodialysis' machines worked 3 shifts per day attending a total of 60 patients each day. A set of interventions was developed to improve the adherence to the recommended catheter venous central (CVC) care practices and new technologies were used in the dialysis unit daily routines.
In 2011 we implemented an evidenced-based intervention bundle that included:
alcohol based gel for hand hygiene available in all machines;
alcoholic chlorhexidine for catheter's disinfection (before alcohol);
citrate to lock the catheter;
chlorhexidine impregnated dressings;
training for new health care workers (HCW) admitted to the hemodialysis' unit and annual re-training for old ones;
catheter care skill evaluation for all nurse staff;
infection rate feedback to all HCW.
Results: In 2012, the BSI was 0.6-1000 CVC-day. After the interventions the rates decreased to zero in 2013, in 2014 and 2015 they were 0.2-1000 CVC-day. In 2014 blood cultures from 32 patients were collected, in these samples 3 had microorganisms isolated (S. aureus, Enterobacter cloacae and Enterococcus faecalis) and 1 infection was considered secondary abdominal. In 2015 blood cultures from 74 patients were collected, 3 had microorganisms (two s. epidermidis and one Enterobacter aerogenes), one infection was secondary to discitis.
Discussion and conclusions: These findings shows that our improved implementation of evidence-based practices and continuing education reduced BSI at hemodialysis centers.
P-072 FIBRIN SHEATH FORMATION AND THE RELATIONSHIP TO INFECTION; ISOTOPE IDENTIFIED SHEATHS - A PREDICTIVE FACTOR OF INFECTION?
D. Hill, F. Brady, F. Hussain, F. Hamblett
The Christie NHS Foundation Trust, Manchester, UK
Introduction: Isotope scans are used routinely for oncology patients for imaging of treatment and disease. It was identified during routine isotope scans that some patients with vascular access devices showed an increased uptake of isotope around the devices. It is assumed that the increased uptake is related to the fibrin sheath formation around the vascular device.
Methods: 196 consecutive patients were examined to identify the incidence of isotope on the devices. These patients were categorised in partial uptake or significant isotope uptake. 39 out of 196 patients were identified as having partial or significant isotope uptake on their devices, the rest had no uptake observed. Each of the 196 patients were followed up by retrospective analysis by reviewing medical notes, electronic records and laboratory results, 3 months prior and 3 months after the isotope scans. Incidence of vascular device related infections were identified.
Results: The data has been collected but not yet analysed. The difference in incidence of infection between the non-isotope group and positive uptake group will be investigated to identify if there is a positive correlation between isotope uptake and infective incidence.
P-073 SUBCUTANEOUS HYDRATION
F.S. Concklin, T.P. Kidd
Centra Lynchburg General Hospital, Lynchburg, USA
Introduction: Oral rehydrationis the preferred method for dehydrated children, but many still require parenteral rehydration which maybe time consuming and costly. There is limited data on the safety and acceptability- for use in children. A clear advantage of succutaneous delivery is that access is much easier to obtain than intravenous access and the training needed for successful insertion is minimal. Although a practice in the ‘70s that declined with the advent of plastic IV catheters, subcutaneous rehydration has resurfaced as an alternative to hydration therapy when oral therapy has failed for IV therapy is difficult to achieve in mild to moderately dehydrated children. Our objectives were to provide a brief overview of how subcutaneous infusion works, how Pediatric nurses implemented the procedure at Centra, and to review improvement i family/nurse satisfaction and impact cost savings.
Methods: Parmacy was consulted for the availability and cost of the medication. A Pediatric nurse developed a nursing policy/procedure and physician order set and presented the procedudre to the Pediatric Service Line and Pharmacy/Therapeutics Committee. After approval to proceed with the project, education was conducted with all the Pediatric unit and Outpatient Infusion Center nurses. Staff was supervised for their first insertion.
Results: All insertions were successful on the first attempt and therapy was able to be initiated quickly and completed. Staff and families were 100% satisfied with the procedure and results.
Discussion and conclusions: Subcutaneous infusion was included in the latest update of the Emergency Nurse Pediatric Course. Subcutaneous infusion may be a bridge for patients whose IV access is unobtainable and may not be at a level for central line or IO. Cost comparison is 1 attempt for subcutaneous vs average of 2.2 attempts IVaccess; less nursing time; and decreased wait for treatment.
P-074 SUBCUTANEOUS INJECTION/INFUSION VIA FLEXIBLE CATHETER
F.S. Concklin, D. Harbour, J. Power
Centra Lynchburg General Hospital, Lynchburg, USA
Introduction: Due to 2 recent needle stick injuries with stainless steel needles being used for subcutaneous infusions, nurses on a skilled/pallative care unit became proactive for patient/nursing safety.
Methods: A committee was formed to review literature on proucts, contact other insitiutions and manufacturers, and review/evaluate products. Product criteria for evaluation included patient/nurse safety, ease of use, minimal priming volume, low profile and minimal patient discomfort.
Results: After reviewing several catheters, the #24 Ga Nexiva IV catheter by Becton Dickinson was selected by the committee. A request to the Quality Value Analysis Committee was made for the catheter. With the assistance of a Vascular Access Team member, a policy/procedure was developed.
Discussion and conclusions: Staff were educated on the new catheter and found the insertion to be easy. No decrease in catheter dwell time or increase in skin redness/hardness around the insertion site has been noted. To ensure catheter patency, the patient must receieve medication every 4 hours or have a continuous infusion.
P-075 AN INTERNATIONAL SURVEY OF CANNULA AND CIRCUIT ACCESS PRACTICES REGARDING INFECTION PREVENTION AND SECUREMENT IN EXTRACORPOREAL MEMBRANE OXYGENATION
A. Corley1, T. Bull1, A.J. Spooner1, C.M. Rickard1, J.F. Fraser1
1Griffith University, Brisbane, Australia; 1The Prince Charles Hospital, Brisbane, Australia
Extracorporeal membrane oxygenation (ECMO) is a complex therapy used to support critically ill patients who have failed conventional medical treatment. The use of large-bore intravenous ECMO cannulae for central vessel access coupled with direct access into the ECMO circuit are significant contributing factors for increased morbidity and mortality. Bloodstream infections are the most common infection during ECMO ranging from 14.85 to 15.7 episodes per 1,000 ECMO days, and cannulae-related infections are reported to be double that of catheter-related infection (7.1 vs 3.4 episodes per 1,000 ECMO days). The Centers for Disease Control and Prevention (CDC) guidelines regarding securement and prevention of infection in central catheters are not specific to ECMO cannulae but are advocated by some ECMO clinicians given the absence of established best practice guidelines for ECMO. The Extracorporeal Life Support Organisation (ELSO) Task Force on Infectious Diseases provides limited recommendations regarding access and securement. ECMO clinical practice is largely based on institutional experience and varies worldwide. Practices regarding access and securement of ECMO cannulae are unknown. The primary aim of this study is to describe current infection prevention and cannulae securement practices regarding ECMO cannula and circuits. The secondary aim is to identify whether practice complies with practice guidelines and recommendations. This is a cross-sectional, descriptive survey of ECMO cannula and circuit management practices. A quantitative questionnaire was developed using evidence-based practice recommendations including the CDC and ELSO guidelines. Purposive sampling was used with the sampling frame being the ELSO Registry. The survey has been implemented and data collected through an online survey instrument. Data collection is ongoing. The findings from this study are important as they will identify gaps between evidence-based knowledge and clinical practice; inform the development of guidelines specific to ECMO cannula and circuit management; and provide baseline data to identify priorities for future research.
P-076 AN INVESTIGATION INTO THE ABILITY OF A DUAL-ANTIMICROBIAL SILICONE ADHESIVE SECUREMENT DRESSING TO PREVENT MICROBIAL RE-GROWTH
A.S. Grande, V. DiTizio
Covalon Technologies Ltd., Mississauga, Canada
Introduction: The use of intravascular catheters is associated with a high risk of infection (superficial and bloodstream infection). They have a significant impact on patient health and healthcare costs. Skin antisepsis and antimicrobial catheters and catheter dressings can be used to minimize the risk of infection. This study investigated the ability of a silicone cover dressing, containing both silver and chlorhexidine directly in the adhesive, to prevent microbial re-growth.
Methods: A single-centre, blinded, randomized study was completed with 37 volunteers, 34 of which completed the study. Two antimicrobial dressings were tested by dividing the patient's back into two zones. Each zone had 5 dressings applied: 1 control non-antimicrobial silicone dressing and 4 of the antimicrobial dressings to be tested. Quantitative skin cultures on days-4 and -7 were taken under the centre of the dressing and under the edges of the dressing using the Williamson-Kligman scrub cup technique.
Results: Both dressings tested had lower microbial concentrations than the controls. The antimicrobial dressing containing both silver and chlorhexidine directly in the adhesive provided a lower microbial concentration under the centre of the dressing and significantly lower under the edges of the dressing than the other antimicrobial dressing tested. This demonstrates the advantage of including antimicrobials throughout the entire contact area of the skin instead of only at the site of insertion.
Discussion and conclusions: The incorporation of both silver and chlorhexidine into the soft silicone adhesive layer of the antimicrobial dressing effectively suppresses re-growth under the entire surface of the dressing for up to 7 days, minimizing the risk of skin infection, particularly at catheter insertion sites.
P-077 AN IN VITRO EVALUATION OF THE ANTIMICROBIAL ACTIVITY OF A DUAL-ANTIMICROBIAL CLEAR SILICONE ADHESIVE SECUREMENT DRESSING
A.S. Grande, V. DiTizio
Covalon Technologies Ltd., Mississauga, Canada
Introduction: The healthcare industry is facing ever increasing demands for solutions relating to hospital acquired infections (HAI). Surgical site infections (SSIs, the second most prevalent HAI) and central line associated bloodstream infections (CLABSIs) represent the first and second most costly HAI respectively. This study focused on evaluating the antimicrobial efficacy of an antimicrobial silicone securement dressing for vascular access devices that contains both silver and chlorhexidine incorporated into the adhesive.
Methods: Log reduction testing challenged the dressing at various time points from 10 minutes to 7-days and the remaining viable organisms were counted following a modified ISO 22196 protocol involving eight common wound pathogens. Strikethrough testing was completed by placing film samples on D/E Neutralizing Agar and inoculated with 1-5 × 101 CFU of the test organisms. The plates were incubated (35 °C) for 7 days and examined daily for the presence or absence of microbial growth.
Results: The dressing demonstrated an average 99.9% (3-log) reduction of viable organisms when challenged (approximately 101 cfu) with Candida albicans, Candida tropicalis, Enterobacter cloacae, Klebsiella pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, Staphylococcus epidermidis, and Enterococcus faecalis after 10 minutes and an average reduction of 99.99% (4-log) after 30 minutes, which was maintained for 7-days. The strikethrough results showed no colony formation under the dressing after 7-days when challenged with each of the above microorganisms.
Discussion and conclusions: The 7-day in vitro antimicrobial activity and barrier performance of the dressing demonstrated its potential ability to minimize bacterial load on the skin at vascular access sites.
P-078 PERFORMANCE OF A DUAL ANTIMICROBIAL SILICONE ADHESIVE SECUREMENT DRESSING USING A HUMAN REPEAT PATCH STUDY
A.S. Grande, V. DiTizio
Covalon Technologies Ltd., Mississauga, Canada
Introduction: Catheter-related bloodstream infections (CRBSI) are one of the most frequent life-threatening complications of vascular access. The use of antimicrobial dressings have been implemented in many hospitals to help minimize the frequency of CRBSIs. The development of cutaneous irritation is not uncommon at vascular access sites and represents another challenge with prolonged dressing use. This is due to the potential release of chemicals and skin stripping that accompanies application/reapplication of adhesive products. This study evaluated the sensitization, irritation and adhesion/pain on removal of two antimicrobial IV dressings.
Methods: Human Repeat Insult Patch Tests were completed through multiple applications of the dressings using a modified Draize Test. The study was single-centre, blinded, and within-subject randomised. A total of nine test dressings were applied over a 3-week period to the back of 216 volunteers (63 male, 153 female). The dressings were applied, removed and reapplied every 48-72 hours for 4 weeks, followed by a 2 week rest period, and then an additional two dressing changes.
Results: Dressing 1 exhibited significantly less irritation (p<0.05) than the centre of Dressing 2. Both dressings did not exhibit contact sensitization. Pain evaluations, on a pain scale of 0 (no pain) to 10 (worst pain imaginable) were completed at visits 4, 7, 10 and 12. Dressing 1 had pain scores that were, on average, 10 times lower than those for Dressing 2.
Discussion and conclusions: The results of this study suggest that Dressing 1 will be extremely well-tolerated by patients. Dressing 1 balances the need for adhesion to the skin with being atraumatic and minimizing irritation and pain on removal.
P-079 PASSIVE DISINFECTION PORT PROTECTOR: EFFECT ON REDUCTION OF CATHETER-RELATED BLOODSTREAM INFECTION
R.P. Ventura1, C. O'Loughlin1, B. Vavrik1
1Aintree University NHS Foundation Trust, Liverpool, UK; 1Queen's University, Belfast, UK
Intravascular devices (IVDs) are widely used for vascular access but are associated with a substantial risk of IVD-related bloodstream infection (BSI). Latest research in BSI pathogenesis has led to novel technologies in IVDs with a prospect to reduce this risk dramatically. Infections of long-term IVDs (most are in place for 10 days), including cuffed and tunnelled central venous access devices (CVADs), implanted subcutaneous central venous ports, and peripherally inserted central catheters (PICCs), are primarily due to microorganisms that gain access to the catheter hub and lumen. The challenge for the future will be to identify safe and cost-effective infection-preventative IVD technologies and to implement their wider dissemination. One example of such technology might be use of passive disinfection port protectors that luer-lock onto needles IV ports. In quasi-experimental research, rate of catheter -related BSI (CRBSI) has been examined. Group of 764 in-patients with CVAD was introduced to the Curos™ port protector while using closed, needle-free IV access system. This represents 18,606 catheter days. CRBSI of this group were compared with past cases prior Curos™ introduction (with passive hub disinfection by 2% of chlorhexidine and 70% isopropyl by nursing staff). The result for pre-Curos™ patients ranged from 0.00 to 9.71 per 1000 catheter days (mean = 3.80). For Curos™ patients, the result was 0.00-1.74 per 1000 catheter days (mean 0.23). The introduction of passive disinfection port protectors appears to be linked to decreased rate in catheter related BSI's.
P-080 SECURING PERIPHERALLY INSERTED CENTRAL CATHETERS, RESULTS OF THE SECUASTAP STUDY: A RANDOMIZED CONTROLLED TRIAL COMPARING SECURACATH® AND STATLOCK®
C.M.P. Janssens, N. Grumiaux, M. Jérôme, G. Maleux, M. Stas, G.A. Goossens
University Hospitals Leuven, Leuven, Belgium
Introduction: The use of peripherally inserted central venous catheters (PICC) is growing over the last years in Belgium. Optimal care and maintenance for those catheters require a weekly dressing change including the change of the securement device. Making an efficient choice is a crucial component in saving nursing time during patient care. Different securement devices are available on the market, such as the StatLock®, already known for a long time period, and the more recently developed, SecurAcath®. The difference between both devices is that StatLock® has to be changed weekly and SecurAcath® remains in place during the entire time the catheter stays in place. The objective of this study is to compare the nursing time for dressing change between the two devices. Moreover, we explored insertion and removal issues and patient experiences.
Methods: From April 2015 till August 2015, in the University Hospitals Leuven, Belgium, 105 patients with any condition who need a PICC line were randomized to receive either a StatLock® or a SecurAcath® as securement device for their catheter. Data were collected at the time of insertion, at removal and at each dressing change for a maximum follow up period of 6 months. The primary endpoint was the time spent for dressing change. Secondary outcome measures include: catheter migration, accidental dislodgement and lab-confirmed catheter-related infection, as well as pain experienced by the patient. Furthermore the usability of the devices was evaluated by the health care workers.
Results: The last patient completed the study on December 15, 2015. Data analysis is ongoing and will be presented.
Discussion and conclusions: Results will be discussed.
P-082 PICC MIGRATION - A PROBLEM OF THE PAST!
D. McParlan, The Infusional Services Team
Belfast City Hospital, Belfast, Ireland
Introduction:“The tip of the catheter should lie within the lower third of the superior vena cava or near its junction with the right atrium” Infusion Nursing Society (2011). Migration from this ideal position has the potential to result in life threatening complications, such as thrombosis and infection, posing significant challenges for the service.
The 1200 PICCs inserted annually by the service for Oncology and Haematology patients were previously secured with an adhesive Statlock stabilisation device which required weekly renewal. Lack of security during reapplication heightened nurses' anxiety and left the PICC vulnerable to migration.
Infusional Services introduced Subcutaneous Anchored Securement (SAS, SecurAcath) in June 2014 as a means of reducing migration.
Methods: An evaluation was undertaken comparing practice prior to and following the introduction of SecurAcath.
Results: There have been no reported incidences of migration or subsequent PICC removal since the introduction of SAS. The reduction in chest x-rays to verify the location of migrated catheter tips and the need for re-insertions has decreased patients' exposure to radiation, reduced delays to therapy and the potential for increased bed occupancy. Fewer PICC re-insertions, the one off insertion of a SAS and the increased confidence of staff resulting in a more efficient dressing change, have resulted in significant financial benefits for the Trust. Additional benefits include reduced skin reactions, improved cleansing of the catheter site and greater user satisfaction. SAS also offers an alternative method of PICC securement for patients who are unable to tolerate any adhesive dressings. Problems encountered in relation to SAS placement and removal were overcome through education, training and support from the company.
Conclusions: SAS has prevented PICC migration. The device has improved patient outcomes, facilitated the service to meet its growing demand, and received positive feedback from staff and patients.
P-084 BABY-PORTS: WHY NOT?
U. Graziano1, L. Calise1, A. Corcione1, S. Fecarotta1, S. Ferraiuolo1, C. Pecoraro1, M. Schiavulli1, G. Severino1, M.I. Spagnuolo1
1Children's Hospital Santobono-Pausilipon, Naples, Italy; 1University Federico II, Naples, Italy
Introduction: In pediatric patients the insertion of central venous ports is not a widely performed procedure, despite the doubtless benefit of such devices in terms of body-schema integrity, low risk of infectious and mechanical complications and improvements in quality of life.
Methods: In our pediatric hospital, we decided to implement the use of baby-ports, i.e. ports small enough to be implantable in infants. All young patients with chronic diseases requiring long term intravenous access were taken into consideration: the indication was discussed with the physicians and the parents, evaluating the pros and cons of such devices in each case.
Results: In the year 2015, we inserted baby-ports on seven male children aged between 4 months and 8 years. Among these, five patients were suffering from chronic diseases requiring intravenous discontinuous substitutive therapy (congenital metabolic deficit, hemophilia, von Willebrand disease), while two patients required long term continuous venous access for total parenteral nutrition (short bowel syndrome) or chronic albumin infusion (Finnish nephrotic syndrome). In these latter patients, baby port was considered after severe problems in the home management of tunneled central venous access devices. The placement of the port was successful and uneventful in all cases. The complication rate was particularly low. Even in the patients with chronic venous access, the repeated punctures of the reservoir were well tolerated.
Discussion and conclusions: Our preliminary experience was encouraging: we are currently expanding the indication of baby-ports in all of our patients requiring a long term discontinuous access and considering it an option also in children requiring long term continuous access.
P-085 A DAY IN THE LIFE OF A PERIPHERAL IV CATHETER: THE PATIENT JOURNEY
S.J. Gallagher, C. Wootten
BD, Calgary, Canada
Introduction: Peripheral intravenous (PIV) catheters are the most commonly inserted invasive medical device utilized in health care. At least 80% of all patients admitted to Canadian hospitals have a PIV inserted. Twenty-six percent of all PIV catheters “fail” and 40% of patients have at least one PIV failure over a course of therapy. Examination of current PIV therapy practices within Canadian institutions led to the development of a framework clinicians can use to determine how their facility's PIV therapy policies and procedures and overall approach to PIV therapy influence outcomes.
Methods: This session will take participants through “a day in the life of a PIV catheter: the patient journey”. The “Patient Journey” is a framework clinicians can use to determine how their facility's PIV therapy policies and procedures and overall approach to PIV therapy influence outcomes. Based on the latest guidelines and standards, the presenters will discuss: risks associated with PIV therapy, implications to practice and patient outcomes.
Results: Integrating individual clinical knowledge and expertise with the best clinical evidence leads to better patient outcomes. These outcomes include: decreasing PIV catheter failure rates; significantly reducing risk of needle stick injury and blood exposure to patients and clinicians; and improving patient and clinician satisfaction through maximizing catheter dwell time and promoting clinical competency.
Discussion and conclusions: At the conclusion of this session, participants will be able to apply the “Patient Journey” framework to: recognize how varying peripheral intravenous (PIV) therapy practices influence PIV outcomes; identify strategies that lead to improving PIV therapy outcomes; and explain why communication between departments is vital to decrease PIV therapy risks.
P-086 THE FIRST EXPERIENCE IN RUSSIA WITH IMPLANTABLE VENOUS PORT SYSTEMS IN THE TREATMENT OF CHILDREN WITH ORPHAN DISEASES
M.Y. Rykov1, I. Filinov1, V.G. Polyakov1
1Institute of Pediatric Oncology and Hematology N.N. Blokhin, Moscow, Russia; 1FSBI “SCCH” of the Ministry of Health of the Russian Federation, Moscow, Russia
Introduction: Orphan diseases in children require life-long and regular intravenous enzyme replacement therapy. This abstract describes the first Russian experience of this group of patients implanted venous port systems in order to create long-term venous access.
Objective: To develop an optimal long-term venous access for enzyme replacement therapy in children with orphan diseases.
Materials and methods: In 2012-2015 we implanted venous port system in 32 patients aged 6 months up to 17 years with various orphan diseases: Mucopolysaccharidosis type I and II, and Pompe disease.
Results: Currently implantable venous port systems are used in 24 (75%) patients. It were observed in 4 cases of thrombosis at 3 (9.3%) patients. All cases of thrombosis were successfully treated. In 1 (3.1%) patient the port chamber turned down the membrane which occurred due to violation of implantation technique, successfully corrected by surgery (Fig. 1).
Conclusions: Implantable venous port systems can be successfully used in pediatric practice for long-term enzyme replacement therapy. However, research in this direction is not carried out.
Port system with an inverted toward the pectoralis major muscle membrane chamber. It is easily identified by the inverted image of the letter: TƆ instead of CT.
P-087 NURSE LED BEDSIDE PICC INSERTION SERVICE: TRANSITION FROM ACUTE REGIONAL TO UNIVERSITY TEACHING HOSPITAL INCORPORATING REAL TIME ECG TIP CONFIRMATION
L.M. Ruegg, M. Faucett
Sunshine Coast Hospital and Health Service, Nambour, Australia
Nambour General Hospital (NGH) Queensland is an acute regional hospital offering a range of specialty services for a population of 340,000. The current bed capacity is 350. The IV Service which consists of 1 full time Clinical Nurse inserts approx. 500 PICC lines per year “blindly” followed by CXR to confirm tip position. In November 2016 NGH moves and expands to the Sunshine Coast University teaching hospital opening with 450 beds expanding to 738 by 2021. We need to adapt to this change and provide a cost effective, accurate bed side service with best possible outcomes. PICC insertion with ECG tip confirmation is not common practice in Australia. There are 5 Nurse Led PICC teams based in radiology and 1 Bedside team - our PICC Insertion service. Magnetic guidance and ECG tip confirmation has been shown to be safe and effective in the placement of PICCs. The goal of the study was to evaluate this technology which is relatively new to Australia and compare the findings with our previous method of confirmation CXR. Which in turn has economic benefits and increases efficiency for our institution. 100 PICCs were placed using Sherlock 3CG. 96.19% were optimal placement e.g. SVC/CAJ compared to 92% inserting our previous technique. Pre 3CG 3% of PICCs were placed in the IJ vein, using the magnetic tracking system 0 were placed in the IJ vein. Technology is constantly changing and to meet best practice guidelines and comply with the Australian Council on Healthcare Standards, the Sherlock 3CG tip confirmation is the best practice that we have chosen to adopt to our service following the success of the 2015 study. The study demonstrated that its decreases labour costs and logistics enabling us to provide an economical bed side insertion service with the added patient benefits of no exposure to radiation.
PICC tip termination using 3CG ECG technology.
PICC tip termination pre ECG.
P-089 LONG TERM USE OF NON-TUNNELLED CENTRAL VENOUS CATHETERS IN CANCER PATIENTS: A RETROSPECTIVE COHORT STUDY
L. Ehrencrona, M. Hubrich, S. Lindgren
Sahlgrenska Academy, Gothenburg, Sweden
Introduction: Long-term use of central venous catheters (CVC) is common in cancer patients in order to facilitate the administration of nutrition and chemotherapy, which is associated with a number of complications. Non-tunnelled CVCs are usually not recommended for long-term use. The aim of this study was to describe the incidence and identify risk factors of CVC-complications during insertion, indwelling and extraction of non-tunnelled CVCs in patients treated in the Department of Oncology at Sahlgrenska University hospital in 2014.
Methods: Patients in the Department of Oncology at Sahlgrenska University hospital that received a non-tunnelled CVC during 2014 was enrolled in a retrospective journal study. Complications and possible risk factors were registered and analysed.
Result: A total of 531 CVCs on 479 patients during 41619.5 indwelling days were included in the study. The total incidence of insertion complications were 12.4%, consisting of arterial puncture (4.3%), malpositioning (2.5%), discomfort (2.3%), pneumothorax (1.1%), haemorrhage (0.8%), arrhythmia (0.8%) and nerve damage (0.2%). The total incidence of indwelling complications were 5.04/1000 indwelling days consisting of infections (0.46 to 2.47/1000 indwelling days), thromboembolic complications (0.43/1000 indwelling days) and mechanical complications (2.11/1000 indwelling days). A higher risk of infection was associated with indwelling-time over 30 days while a higher risk of mechanical complication was associated with TPN, CVC changed over a guidewire and CVC with more than one lumen. Increased cumulative risk of infection was associated with use of TPN.
Cumulative risk of CVC-infection with/without TPN.
Conclusions: The indwelling-time is an important risk factor for complications to non-tunnelled CVCs. Limiting the indwelling-time or using other types of CVCs could probably decrease the incidence of infections, and the cost associated with them. This must be weighed against the cost of placing tunnelled CVCs and subcutaneous ports and the increased risk of thrombosis associated with peripherally inserted CVCs.
P-090 PSYCHOLOGICAL ASPECTS OF INTRAVENOUS TREATMENT IN ONCOLOGY AND PERMANENT VENOUS ACCESS DEVICES TOLERANCE
V. Manasek, V. Manasek, J. Jokl, K. Slovackova
Novy Jicin Hospital, Novy Jicin, Czech Republic
Introduction: Since any intervention in the physical integrity of individuals are necessarily reflected in his mental level, we decided to conduct a survey dealing with tolerance of intravenous therapy in cancer patients. Especially, we focused on long-term venous access devices tolerance.
Methods: The aim of this study was to evaluate descriptively patients' awareness of the administration of parenteral drugs, risks in the application and the differences between the administration of drugs to the central and peripheral venous system. To collect data, own questionnaire containing 21 questions was compiled. It was distributed to patients in the oncology department and outpatient oncology ward at the hospital Novy Jicin, Czech Republic. Patients signed an informed consent to data collection. 100 valid questionnaires were evaluated in the analysis of the data.
Results: The results of the study generally indicate that patients do not tolerate venous sampling and intravenous therapy optimally. Patients who have some form of venous access device are mostly satisfied, it fulfills its mandate of maximum patient comfort.
Conclusions: The results indicate that most of the patients know alternatives to peripheral drugs application. However, awareness of this issue is inadequate. The vast majority of patients would recommend the introduction of long-term venous access device to other patients.
P-091 ADOPTION OF ECG GUIDED CVC TIP LOCATION ON INTENSIVE CARE IN THE UK
M.E.P. Jones
East Kent Hospitals University NHS Foundation Trust, Ashford, UK
Introduction: ECG based technology to aid the placement of a PICC tip into the central venous system is now widely accepted practice in the UK. It has been shown to safe, effective and accurate. However, it has not been widely adopted in intensive care units (ICUs) in the UK for CICC (Centrally Inserted Central Line) placement. This presentation examines the issues around embedding this technology as well as describing the barriers to implementation on one ICU in the UK.
Methods: Snapshot survey of Intensive Care Units in UK to ascertain: Current knowledge and current usage of ECG tip location technology.
Description of the programme of implementation with ICU staff in our own UK institution, recording the attitudes and issues of clinicians.
Difference in incidence of complications between subgroups
Infection
Tromboembolic complication
Mechanic complication
p-value
incidence (%)
p-value
incidence (%)
p-value
incidence (%)
0-30 days/>30 days
0.037
13.2/22.0
1.000
3.3/3.8
1.000
17.4/17.2
Females/males
0.463
19.1/22.1
0.435
3.2/4.9
0.438
16.4/19.3
Not TPN/TPN
0.123
27.9/18.9
0.149
4.2/0.0
0.000
14.7/36.1
V. jugularis interna/v. subclavia
0.556
26.3/19.7
0.517
3.6/5.3
0.755
17.1/21.1
New placement/changed over guidewire
0.828
20.1/17.6
0.628
4.0/0.0
0.008
15.9/35.3
One lumen/multiple lumina
0.641
19.3/22.6
1.000
3.8/3.2
0.002
15.5/38.7
TPN = total parenteral nutrition.
Results: Snapshot survey
Clinical staff on nearly every ICU in UK had no knowledge of ECG tip location technology. Usage in everyday practice almost never occurred.
Implementation on our own ICU
Current practice of using a post-insertion confirmatory chest radiograph is solidly embedded. Staff feel it is mandatory even though on 30% of chest radiographs, tip position could not be seen.
There was almost no prior knowledge at all, amongst staff members regarding ECG technology.
Currently used multi-lumen CICCs are too short to reach the lower third of the SVC in most cases.
Discussion: Discussion as to why this recommendation has not been adopted in the UK will be given. Feedback from UK Intensive Care staff will be presented.
Conclusions: The use of ECG technology during placement of CICCs on ICUs is widespread in many countries in the world but not the UK. Knowledge sharing across specialties is needed to encourage adoption of this simple and safe method in ICUs in the UK.
P-092 EFFECT OBSERVATION OF AUTOMATIC RESET METHOD IN PICC TIP IN THE JUGULAR AND CONTRALATERAL SUBCLAVIAN VEIN
W.F. Chen, L. Liu, L.X. He
Xiangya Hospital, Central South University, Changsha, China
Introduction: The purpose of this study is to observe the function of the peripherally inserted central catheter (PICC) that when the positioning of tip of PICC is in the jugular and contralateral subclavian vein.
Methods: We looked it as the normal position when the positioning of tip of PICC was in the jugular and contralateral subclavian vein. At the meanwhile, the patients who were inserted these catheters were independent living. The function of the catheter and the patients' symptoms and signs were watched. Then the patients took a chest X-ray to verify the positioning of the PICC tip 3 and 7 days later.
Results: From 2013 to 2015, 866 PICCs were positioned, the positioning of tip of 22 in jugular vein, 3 in contralateral subclavian vein. The function of the catheter was normal. The patients have no symptoms and signs. Seventy-six percent of the positioning of the PICC tip reached the correct position of the tip in SVC 3 days later; Twenty percent reached the correct position of the tip in SVC 7 days later.
Discussion and conclusions: When the patients with PICC could have an independent living. Although the tip of PICC was not in the correct position of the tip in SVC, it was in the jugular and contralateral subclavian vein, the function of the catheter could keep normal and the patients have no symptoms and signs.
P-093 SAFETY IN VASCULAR CARE OF HIGHLY COMPLEX PATIENTS
V. Armenteros-Yeguas1, M.A. Tomás-López1, M.I. Moraza-Dulanto1, E. Cristóbal-Domínguez1, E. Merino-Romero1, E. Miranda-Serrano1, L. Meléndez-Fernández1, L. Garate-Echenique1
1Araba University Hospital, Vitoria-Gasteiz, Spain; 1Araba Research Unit, Vitoria-Gasteiz, Spain; 1Santa Marina Hospital, Bilbao, Spain; 1Donostia Hospital, Donostia-San Sebastián, Spain
Introduction: The aim of this study was to describe and compare security in vascular care in patients with good venous access (GVA) and patients with poor venous access (PVA) and determine the risk of adverse events in both groups.
Methods: A cohort study was conducted in a sample of highly complex patients classified with Kaiser Permanente's definition. Two groups were established, GVA (visible and palpable veins and no history of more than two punctures for catheter insertion) and PVA.
Security in vascular care was measured by the number of VAD and caliber, number of punctures, hematomas at the moment of insertion, duration of VAD and number of adverse events. Incidence of adverse events was calculated and Chi-square and Student t-test/U-Mann-Whitney was used to compare security between groups. The OR was calculated to establish the risk of complications. A 95% confidence interval and α = 0.05 were considered.
Results: 135 patients were recruited, 34.8% women and 59.3% (95% CI 50.8-67.9%) with PVA. 224 VAD were inserted. Patients in PVA group required a mean of 1.71 VAD (SD = 1.07) and patients in GVA group 1.58 (SD = 0.96) (p = 0.496). The use of small catheters (22G) was statistically significant between PVA and GVA group, 29.6% and 11.5% respectively (p = 0.002). Number of punctures (two or more) need to insert a catheter was also significant between PVA (23%) and GVA (2.5%) (p<0.001). The presence of hematomas at the time of puncture was 24.8% (PVA) and 10.3% (GVA) (p = 0.007). The incidence of adverse events was 114.9/1000 catheter-day (95% CI 90.3-145.2) for PVA group and 95.52/1000 catheter-day (95% CI 65.3-134.8) (p = 0.343). The OR for the incidence of complications was 1.38 (95% CI 0.79-2.40).
Discussion and conclusions: Highly complex patients with PVA presented with more hematomas and required more VAD, more attempts to insert them and higher percentage of small caliber catheters.
P-094 ULTRASOUND AND FLUOROSCOPY GUIDED RIGHT INTERNAL JUGULAR CENTRAL VENOUS CATHETER INSERTION IN HEMODIALYSIS PATIENTS WITHOUT ROUTINE CHEST RADIOGRAPHS
S. Arya1, B. Arya1, M. Amirivahid1, M. Khavaninzadeh1
1Iran University of Medical Sciences, Tehran, Iran; 1Golestan University of Medical Sciences, Gorgan, Iran
Introduction: Post-procedural chest radiograph can show correct position and potential complications after central venous catheter (CVC) insertion; however, it increases patient's expenses and radiation exposure especially in chronic hemodialysis cases with multiple insertions. Our aim is to study complications of ultrasound and fluoroscopy guided right internal jugular CVC insertion without routine chest radiograph.
Methods: A prospective observational study was performed on consecutive patients with urgent hemodialysis indications in Hasheminejad Kidney center, Tehran, Iran, March 2012 - December 2015. Patients with pre-existing pleural effusion were excluded. An experienced vascular surgeon inserted temporary double lumen catheters in right internal jugular veins with Seldinger technique, under ultrasound and fluoroscopy guide. Patients admitted in hospital for hemodialysis and evaluated through serial clinical examinations for at least 72 hours.
Results: Total number of 287 catherters were inserted in 231 patients with mean ±SD age of 54 ± 16 years. As with intraoperative ultrasound and fluoroscopy, serial clinical examinations showed no evidence of pneumothorax, hemothorax, or catheter tip malposition. We estimated 5500 dollars cost saving by elimination of routine chest radiographs in this series.
Discussion and conclusions: In clinically non-suspicious patients, chest radiography may not be an essential procedure after image-guided right internal jugular CVC insertion. further research is needed to define the cost-effectiveness of such radiographs according to the specific healthcare and monetary systems.
P-095 ULTRASOUND-GUIDED INFRACLAVICULAR AXILLARY VEIN CANNULATION FOR CENTRAL VENOUS ACCESS IN CANCER PATIENTS
G.L. Guo
Sichuan Cancer Hospital, Chengdu, China
Introduction: In China, the venous access of Peripherally Inserted Central Catheter (PICC), internal jugular vein and subclavian vein are the priority choices to insert central venous catheters for cancer patients. However, there are great challenges including poor venous condition, not tolerating repeated acupuncture and the influence of tumor masses. The axillary vein is the direct continuation of the subclavian vein. Different from subclavian vein, infraclavicular axillary vein is visible in the guidance of ultrasound. But nowadays, the application and relevant reports of axillary vein in cancer treatment are limited in China.
Objective: To explore the accuracy, security and the key point of ultrasound-guided axillary vein catheterization technology.
Methods: The data were collected on 136 cancer patients accepted insertion of ultrasound-guided infraclavicular axillary venous access from December 2013 to November 2015. The one-time successful catheterization rate, the right location rate of the catheters and the complication rate are the primary data measured.
Results: 95.6% of all catheter tips located in exactly at the target by X-ray. The axillary vein was successfully punctured with the guide of ultrasound with first needle pass in 88.2% of cancer patients. The rate of one-time successful insertion of catheters accounted for 94.1%. And the total successful catheterization rate was 97.8%. The catheterization complication rate was 4.4%, including tip malposition (3 cases), accidental injury artery (2 cases) and 1 case of pneumothorax.
Conclusions: In the analysis of ultrasound-guided infraclavicular axillary venous access in this group, the majority of patients were cannulated successfully and safely. This research demonstrated that infraclavicular axillary venous access can be an alternative of central venous accesses. Due to the vital organs and complex tissue around the infraclavicular xillary vein, we should take the cases with good vascular puncture condition as the priority choice and give X-ray check in time.
P-096 Medical and surgical patients' experiences of peripheral IV insertion: a qualitative study
E.N. Larsen, S. Keogh, C. Rickard
Griffith University, Nathan, Australia
Introduction: Peripheral venous catheters (PVC) are the most common invasive device inserted for patients requiring medical treatment. Previous studies have found these devices cause a range of outcomes from mild discomfort to extreme pain or anxiety for patients. Little research has been conducted to date to explore the patient's experience of PVC insertion using qualitative methodology. The aim of this study was to gain an understanding of patients' experiences of PVC insertion. To do this we conducted a study using a phenomenological-hermeneutic approach involving semi-structured interviews.
Methods: Gadamer's Phenomenological method was used to explore the PVC insertion experience of a purposive sample of patients from medical and surgical wards at a tertiary hospital in Queensland, Australia. Consenting patients were interviewed using a semi-structured technique. The interviews were audiotaped, then transcribed and thematically analysed. The length of the interview was determined by patient responses, ranging from 5 to 30 minutes.
Results: Ten patients (aged 24-79 years) participated in the study. Seven were from surgical disciplines; three were general medical patients. 8/10 patients had at least one PVC inserted in emergency; and 7/10 patients had at least one device inserted in the cubital fossa. Of the total 26 PVCs, 19 were inserted by a doctor, and 6 by a nurse inserter. Ultrasound techniques were not used. Patients spoke of concern related to the perceived skill of the inserter and communication break-downs occurring between patient and inserter. Patients also suggested potential areas of improvement for insertion techniques, insertion site choice and maintenance options to increase comfort and reduce anxiety.
Discussion and conclusions: A clear understanding of patient experiences is essential for clinicians and health services to critically reflect upon and improve their insertion practices and patient experiences. Being responsive to consumer perspectives will impact positively upon overall patient satisfaction and insertion service provision.
P-097 INFUSION FLOW RATES AND INSERTION SUCCESS THROUGH THE STERNUM USING A MULTI-SITE INTRAOSSEOUS DEVICE
T.E. Philbeck, D.F. Diana, T.A. Puga, C. Davlantes, L.J. Miller
Teleflex Medical, San Antonio, USA
Introduction: Intraosseous (IO) vascular access is an effective option for vascular delivery of critically-necessary drugs and fluids. First described by Tocantins in 1940, the sternum was among the first bones used for IO access. In 2012, a new FDA-cleared manually-inserted sternal IO device was introduced (Arrow® EZ-IO® T.A.L.O.N.™, Teleflex, Morrisville, USA) primarily for military/tactical medicine use. Secondarily, the device can be inserted into the humerus and tibia for infusion. A prospective, single-site study of the T.A. L.O.N. device was conducted to examine performance characteristics.
Methods: IRB approval was obtained; healthy volunteers were recruited. The IO device consists of a 38.5 mm/15g needle-set, with a sternal locator to establish sternal access; without locator for extremity access. 24 sternal IO insertions were performed by 8 military-trained medics. Normal saline (NS) was infused via pressure-bag with flow-rates calculated after 3 minutes of infusion at various infusion pressures. The NS bag was weighed before and after each infusion to determine volume infused. Subjects were monitored for signs of infiltration during and after infusion.
Results: Subject mean age was 33.4 ± 8.8 years; 79% were male. Mean BMI was 26.3 (range: 17.1-31.7). Four subjects (17%) had a BMI >30, but without excess tissue overlying the insertion site and palpable landmarks.
Successful needle placement was initially confirmed by aspiration in 100% of cases. One case each of minor infiltration and needle dislodgment were observed under fluoroscopy, yielding a first attempt placement success rate with functionality of 92%. In no cases was there penetration of the posterior cortex of the manubrium. The mean infusion rates were: 1130 ± 692 ml/hour at gravity; 3374 ± 1370 ml/hour at 100 mmHg; 4619 ± 1785 ml/hour at 200 mmHg; and 5327 ± 1724 ml/hour at 300 mmHg. There were no serious complications.
Discussion and conclusions: Results suggest the T.A.L.O.N. device may be used to safely and successfully establish IO vascular access in the sternum with excellent infusion flow rates.
P-098 INTRAOSSEOUS CATHETER DWELL-TIME APPEARS SAFE FOR UP TO 48 HOURS: A PRELIMINARY REPORT
C. Davlantes1, L.J. Miller1, E. DeNoia1, D.F. Montez1, T.A. Puga1, T.E. Philbeck1
1Teleflex Medical, San Antonio, USA; 1ICON Early Phase Service, San Antonio, USA
Introduction: Despite few complications associated with intraosseous (IO) vascular access, the US FDA restricts catheter dwell-time to 24 hours. Under an Investigational Device Exemption and IRB-approval, a study is underway to determine the safety of IO access with the catheter in-place for 48 hours. We provide a preliminary report.
Methods: Adults with renal impairment and/or diabetes have an Arrow® EZ-IO® catheter (Teleflex, Morrisville, USA) placed in the proximal humerus or tibia. Some receive midazolam for anxiety and/or fentanyl to mitigate pain associated with the procedure. Infusion pain is managed initially with IO lidocaine, then as needed with oral acetaminophen. For higher levels of pain, intravenous/intramuscular ketorolac and/or oral hydrocodone/acetaminophen are administered. With slow continuous saline infusion, subjects remain in a research facility for 48 hours. Prior to removal, an IO aspirate culture specimen is obtained from the in-situ catheter. Following removal, an x-ray is taken of the insertion site. After 30-days, subjects return for examination and insertion site x-ray.
Results: As of December 2015, 39 subjects completed the study. There have been no serious adverse events/complications. The IO aspirate cultures have shown no signs of microorganism growth associated with osteomyelitis, or other abnormalities in plain radiographs. Pain associated with catheter dwell and infusion has been well-managed with additional medications, a finding previously unreported. Administration of fentanyl and midazolam before IO insertion has mitigated pain and anxiety associated with the initial saline-flush.
Discussion and conclusions: Preliminary results indicate IO access can be safely maintained for 48 hours without risk of serious adverse events. Extended dwell time and increased IO access utilization could result in avoidance of serious complications and costs associated with CVC placement solely for difficult vascular access. Additional analgesics for infusion pain management may be more effective than the current practice of administering lidocaine into the IO space.
P-099 THE USE OF ULTRASOUND TECHNIQUES BY NURSES FOR DIFFICULT PERIPHERAL VENOUS ACCESS IN EMERGENCY DEPARTMENT
J.J. Martinez-Moreno, M.A. Rodríguez-Calero, I. Fernández-Fernández, A. González-Trujillo, E. González-Fierro, R. Oyarbide-Lasarte
Hospital Manacor, Manacor, Spain
Introduction: Difficult peripheral venous access (DVA) is common in emergency department (ED), causing negative consequences for patient and staff, such as treatment delay, increase in the use of central venous catheter and patient and professional stress.
The aim of this study is to evaluate the characteristics of patients with DVA in ED and the utility of ultrasound (US) in contrast to traditional approach (TA) in DVA catheterization.
Methods: Cross-sectional study. Adult patiens in need of venous access in ED of Hospital Manacor-Mallorca (Spain) were selected (1st/feb/2015 to 31st/mar/2015), inclusion criteria was two or more failed attempts of insertion, previous history of DVA or failed attempts by other proffessionals due to inability to identify a suitable vein. Exclusion criteria were vital emergency, pregnancy and no informed consent.
Nurses recorded anonimously variables related to their intervention, patient's health conditions and DVA characteristics inmediatly after cannulation.
Statistic analysis with Epidat 4.0 included descriptive statistics and association tests.
Results: 13 nurses with more than 2 years of experience were enrolled, reporting 51 DVA cases. Main characteristic of DVA was the inability to identify a vein by palpation (77.55%). Most frequent chronic condition was obesity (45.1%) (Tab. I).
TA was used in 40 patiens, Static Approach in 3 and Dynamic Approach (DA) in 36 patients, 28 of them after failed TA attempts. Punctures average was 2,922 ± 1,647, DA group had received 1,833 ± 1,483 punctures prior to US technique. TA success rate was 37.5% vs 88.89% of DA (Tab. II). Catheter diameters were higher in DA group.
Discussion and conclusions: Multiple puncture is a common and avoidable consequence of DVA. US techniques carried out by nurses seem to be more effective than TA to solve DVA cases in ED.
Understanding DVA risk factors could help us to early identify difficult cases and prioritize US.
Patient characteristics
n
51
Age
68,745 ± 18,415
Sex
Woman
31 (60,78%)
Man
20 (39,22%)
Difficult venous access profile
No palpable veins
37 (72,55%)
No visible veins
34 (66,67%)
Previous history of difficulty
34 (66,67%)
No palpable + no visible veins
31 (60,78%)
2+ failed attempts
25 (49,02%)
Chronic health conditions
Obesity
23 (45,1%)
Quimiotherapy
15 (29,41%)
Diabetes
12 (23,53%)
Chronic renal failure
5 (9,8%)
Chronic liver failure
4 (7,84%)
Low weight
3 (5,88%)
Parenteral drug abuse
1 (1,96%)
Acute conditions
Hypotension
15 (29,41%)
Tachycardia
10 (19,61%)
Arrhythmia
6 (11,76%)
Pain
1 (1,96%)
Hypothermia
0
Analysis techniques
Total
Traditional approach
Static approach
Dynamic approach
n
51
40 (78,43%)
3 (5,88%)
36 (70,59%)
Age
68,745 ± 18,415
72,125 ± 14,513
47,333 ± 42,442
67,222 ± 16,121
Punctures
2,922 ± 1,647
2,25 ± 1,276
3 ± 2,646
1,389 ± 0,688
Technique in previous attempts
29/51 (56,86%)
25/51 (49,01%)
1/51 (1,96%)
1/51 (1,96%)
Previous attempts by other professionals
1,353 ± 1,56
0,762 ± 1,091
1,667 ± 2,887
1,833 ± 1,483
Professionals
Registered nurse
1,647 ± 0,658
1,7 ± 0,687
1,333 ± 0,577
1,833 ± 0,655
Nursing assistant
0,784 ± 0,577
0,825 ± 0,549
0,333 ± 0,577
0,944 ± 0,532
Efficacy
49/51 (96,07%)
15/40 (37,5%)
3/3 (100%)
32/36 (88,89%)
First attempt success
27/51 (52,95%)
5/40 (12,5%)
1/3 (33,33%)
24/36 (66,67%)
Catheter inserted
None
2 (3,92%)
25 (62,5%)
0
4 (11,11%)
18G
15 (29,41%)
2 (5%)
3 (100%)
10 (27,78%)
20G
26 (50,98%)
5 (15%)
0
21 (58,33%)
22G
5 (9,8%)
4 (10%)
0
1 (2,78%)
24G
4 (7,84%)
4 (10%)
0
0
Average size
21,333 ± 2,093
18 ± 0
19,438 ± 1,045
P-100 CATHETER PICC USE IN NEWBORN INTENSIVE CARE UNIT IN PUBLIC PEDIATRIC HOSPITAL OF NORTHEAST OF BRAZIL: 2014-2015
1Universidade Estadual do Ceará, Fortaleza, Brazil; 1Hospital Infantil Albert Sabin, Fortaleza, Brazil
Introduction: PICC has been widely used in the context of the NICU, considering its advantages and a low complication rate when related to other catheters.
Objectives: The main objective of this study was to evaluate the use of the PICC in the neonatal ICU of a public hospital pediatric reference of northeastern Brazil.
Methodology: Descriptive study, studying all punctures for two years, 1 January 2014 to 31 December 2015, totaling 1,000 catheters, with 647 in 2014 and 353 in 2015 in NICU that has 12 beds. Data were processed and analyzed using SPSS version 20.0. A descriptive analysis of all variables, using absolute and relative frequencies for categorical and mean, standard deviation, minimum and maximum for continuous.
Results: The average catheters punctured a day was 3 devices and the first device in 2014 and 2015 respectively. The length of stay averaged 16 days in 2014 and 12 days in 2015 and most of the catheters were removed by treating end 78.0% in 2014 and 78.19% in 2015. The main complication associated with PICC is displacement of the catheter 51.94%, then obstruction 18.18% and infection 15.5%. Puncture total, 83% were performed in infants with <1,500 g and 40.0% of these children had at the time more than 1 catheter PICC. the tip location of catheters, 67% in 2014 and 57% in 2015 were in central position vena cava. The high rate of displacement of the catheter waswas associated with the nonstandard stabilization technique established in the institution protocol (p = 0.012).
Conclusions: There is an urgent need for improvements in maintenance practices for the unity of nursing staff, given the high rate of observed compliance, which are much lower than seen in more advanced centers.
P-101 THE ROLE OF A SURVEILLANCE PROGRAM FOR SUCCESSFULLY INTRODUCING PICC CATHETERS: A 2-YEAR OBSERVATIONAL STUDY IN AN ACADEMIC HOSPITAL
E.F. Lo Priore, M.C. Fliedner, M. Heger, U. Novak, J.T. Heverhagen, J. Marschall
Bern University Hospital, Bern, Switzerland
Introduction: In our hospital a previous attempt to introduce peripherally inserted central catheters (PICC) was aborted due to an unstructured approach, seemingly accompanied by high rates of complications. The goal of this study was to introduce PICCs in an academic hospital accompanied by surveillance for infectious and non-infectious outcomes.
Methods: We prospectively collected data for this surveillance study from all patients who underwent PICC insertion from January 1, 2014 and had the catheter removed by December 31, 2015 at our 950-bed academic hospital (Bern University Hospital, Switzerland). Infectious complications were defined according to CDC/NHSN criteria. PICCs were restricted to oncology and infectious diseases patients and were followed irrespective of the management setting (outpatient, inpatient, intermittently hospitalized after insertion).
Results: One hundred thirty-five PICCs were inserted in 124 patients, the majority being oncology patients (n = 116, 85.9%). Indications for PICC insertions included: chemotherapy (n = 97, 71.9%), antibiotic therapy (n = 24, 17.8%), total parenteral nutrition (n = 8, 5.9%), blood product transfusion (n = 4, 3.0%) and palliative care (n = 2, 1.5%). During a total of 10'267 catheter-days (median dwell time 61 days), five CLABSI (including one mucosal barrier injury laboratory-confirmed bloodstream infection, MBI-LCBI) and two exit-site infections occurred, yielding an incidence rate of 0.49 and 0.19 infections per 1000 catheter-days, respectively. Incidence rates were 0.68/1000 catheter-days (n = 7) for radiologically documented deep venous thrombosis, 0.97 (n = 10) for tip dislocation, and 0.68 (n = 7) for catheter occlusion. Seventeen catheters (12.6%) were removed because of a complication.
Discussion and conclusions: We successfully introduced PICCs in an academic hospital by implementing a surveillance program for complications. Both infectious and non-infectious complications were rare. Infection prevention specialists should be actively involved during the introduction of new intravascular devices in order to provide quality indicators and assure patient safety.
P-102 CONTRIBUTION OF A NEW TEACHING TOOL FOR SAFE PLACEMENT AND REMOVAL OF ADHESIVE SUTURELESS SECUREMENT DEVICES (ASSDs) FOR PICC-LINES
C. Dupont1, B. Lehasif1, B. L Jaouani1
1Cochin Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France; 1Cancer Research Institute François Baclesse, Caen, France; 1Freelance homecare nurse, Paris, France
Introduction: In consideration of the results of a survey auditing the practices of 296 freelance homecare nurses, we observed that 122 nurses had already used Adhesive Sutureless Securement Devices (AASDs) and about 25% of them considered removal and placement of these devices problematic. Irregular practice, issues with ASSD design (too sticky, PICC displacement risk when placing/removing device) and the absence of a user guide on the packaging were common explanations. Inadequate caregiver training has been identified as a contributing factor for PICC related complications. To respond to this issue and to complement existing educational tools (video, leaflets), we created an arm band designed to make the difficulties of the skill more intelligible during workshops. Our goal is to evaluate the effectiverness of such an educational tool.
Methods: During the national nursing conference held in Paris, in May 2016, this arm band will be tested by a group of freelance homecare nurses, hospital nurses, nursing instructors and private homecare medical device providers. During the workshops, they will practice in pairs. One will wear the arm band into which a PICC is inserted, and the other will practice placing and removing the ASSD. Then the roles will be reversed. After practicing with the 3 most commonly used ASSDs in France, participants will fill out a questionnaire evaluating the effectiveness of the arm band as a teaching tool.
Results: The results of the survey will be presented at the 4th edition of WoCoVA.
Conclusions: Providing adequate tools, such as this arm band, for nurses to practice difficult skills can contribute to increasing patient safety and care quality.
P-103 IMPACT OF THE CREATION OF A SHORT-TERM CENTRAL VENOUS CATHETER (CVC) FOLLOW UP AND IMPROVEMENT MULTIDISCIPLINARY TEAM
E. Alonso
Hospital Nuestra Señora del Prado, Talavera de La Reina, Spain
Introduction: Catheter-related bacteremias (CRB) represent 12% of the nosocomial bacteremias and they are responsible for 10-20% of the nosocomial infections. 90% of the nosocomial bacteremias are caused by CVC. According to a study in Spain, CRB was related to an approximately 20 day prolongation of the stay and an additional cost increase for the system of 3000 euros per episode.
Objective: Determine the short-term CVC related bacteremias incidence in hospitalized patients in Hospital Nuestra Señora del Prado and evaluate the impact of the creation of a follow up and management multidisciplinary team of those catheters.
Methods: The multidisciplinary team is formed by a nurse, two internists and two microbiologists. November 2013: Actualization and diffusion of the CVC management protocol. February 2014: Registration of patients with short-term CVC. March 2014-September 2015: Registration, follow up and dairy revision of all short-term CVC and direct training of nursing staff.
Results: Data from 414 short-term CVC was collected, with a sum of 4328 catheter days. 13 CRB were confirmed during the period before the actualization and diffusion of the CVC management protocol (from July to October 2013), with an estimated incidence of 12,9 cases/1000 catheter days in this period. 11 CRB were confirmed in the period after the actualization and diffusion of the CVC management protocol (from November 2013 to February 2014), with an estimated incidence of 9,6 cases/1000 catheter days. 6 CRB were confirmed during the intervention period (from March 2014 to September 2015), with an observed incidence of 1,5 cases/1000 catheter days.
Discussion and conclusions: Before the beginning of the short-term CVC follow up and improvement multidisciplinary team activity the CRB incidence was high. After the beginning of its activity the CRB incidence has been considerably reduced.
P-104 EVALUATION OF THE INSERTION OF PERIPHERAL CATHETERS FOR VENOUS ACCESS GROUP OF A PUBLIC HOSPITAL PEDIATRIC REFERENCE IN NORTHEASTERN BRAZIL
1Hospital Infantil Albert Sabin, Fortaleza, Brazil; 1Universidade Estadual do Ceará, Fortaleza, Brazil
Introduction: The creation of catheters teams has been identified as one of the most important strategies for the adoption of the culture of good practice in the context of infusional therapy. Objective: To evaluate the insertion of peripheral catheters for venous access group - GAV of a public hospital pediatric reference of northeastern Brazil.
Methodology: Descriptive study performed from January to December 2005, which were evaluated 3,489 peripheral catheters inserted by members of the GAV. We used the program SPSS- 20. frequency measures were calculated statistical averages and standard deviation measures the quantitative variables as well, comparisons were made of the proportions of percentages through the x2 test and likelihood ratio.
Results: Regarding the punction attempts, 66.10% were obtained after the first attempt and 83.2% in the second attempt. Most catheters were implanted for administration of antibiotics, with pH less than 5, more than 10 days. Thus it was observed that 63% of these children had indicated PICC, the device according to the choice of algorithm. It is noteworthy that were patients of difficult access and with significantly impaired venous network. Children attended 16% of them were appointed central venous access, given the impossibility of punction.
Conclusions: It can be seen that despite the good skill of venous access group from the hospital, and of its existence, the planning of infusional therapy, including the choice of intravenous device becomes imperative for the implementation of safe practices, and certainly the scope of quality indicators.
P-105 THE IMPLEMENTATION TIME OF THE CATHETER AND ITS CHANGES IN NEONATAL CARE
M.V. Ferreira, C.P.M. Moraes, M.R.M. Nascimento
Clínica Perinatal Barra, Rio de Janeiro, Brazil
Introduction: The hospital-acquired infections, especially in critical patients, in addition to the economic impact, are related to high morbidity and mortality, and bloodstream infections (ICS) associated with central venous catheter (CVC) the leading cause of mortality in neonatal intensive care units. In place of that study the incidence of central venous catheter related infection was the top 50 percentile of CDC/CEVSP, despite various interventions.
Objective: Implementation of a catheter for reducing incidence rates of IPCSCVC to generate change in the care provided to inmates in this study utineonatal Rns.
Methodology: This is a descriptive study of a quantitative approach. The study was conducted in utineonatal of a private maternity of medium to large size references in high-risk gestation in the municipality of Rio de janeiro with 60 neonatal beds and an average occupancy of 75%. The data is collected daily by the CCIh staff calculating the number of monthly infections by 1000 catheters day. In this way, we decided to implement the catheter that encompassed the preparation of checklist; nurses and doctors handling constraint; training and team awareness about hygiene of the hands; preparation of the skin; maximum barrier precautions; transparent sterile dressing device; asepsis of the connections with alcohol 70%; We have grouped catheter manipulation; daily review use of the device; weekly meetings; discussion of unwanted events; and disclosure institution of days without infection.
Result: The average rate of infection related to CVC pre-intervention was 8.4/1000 catheter-days and the average was 2.7 post-intervention/1000 catheter-days.
Conclusions: The implementation of the team with preventive measures during the catheter insertion and maintenance is of fundamental importance for reducing the rate of infection. Note-If a multidisciplinary team's concern with patient safety in preventing hospital-acquired infections and, consequently, in the morbidity and mortality of Rns admitted to the institution.
P-106 CESSATION OF ROUTINE CXR IN ECG GUIDED PICC PLACEMENT - A LESSON IN CHANGING PRACTICE AND MINDS
F.J. Gillanders
St. George Hospital, Sydney, Australia
Introduction: Cancer Services nursing staff aimed to establish a PICC insertion service that delivers the best possible patient experience and outcomes through utilisation of contemporary insertion techniques. Literature supports that ultrasound guided vascular access and electrocardiograph (ECG) tracking confirmation systems (TCS) enable timely PICC insertion and provide the safest and most accurate insertion method. The project objectives were to establish a quality, sustainable, readily available PICC insertion service for cancer patients. Incorporating change in clinical practice through cessation of chest X-ray (CXR) confirmation of PICC tip placement, and advance nursing scope of practice to release PICC lines for use.
Methods: Gain managerial approval
Arrange use of TCS, training and ongoing support
Engage lead cardiologist and radiologist - provide literature for review, seek endorsement
Presentation to products committee - trial consent
Record trial outcomes
Present to local nursing and medical leaders, key stakeholders and clinical groups seeking endorsement for policy change: Demonstrate alignment of literature, trial outcomes, practice change benefits with the Australian Nursing and Midwifery Board Nursing Practice Decision Flowchart Submit endorsed policy amendment to local policy governance group.
Results: A sustainable high quality PICC insertion service has been established. Routine CXR has ceased. Appropriately qualified nurses have been endorsed to release PICC lines for use.
Discussion: Instigating change can be difficult as pioneering clinicians face attitudes such as “that's the way we have always done it” and “fear of recrimination”. Designing and following a systematic process to gain buy-in that leads to practice and policy change is useful in advancing nursing practice and improving patient centred quality care. By aligning proposed practice changes with professionally developed frameworks such as the Australian Nursing and Midwifery Board Nursing Practice Decision Flowchart, necessary assurance is demonstrated regarding risk management and enhanced safe and quality care.
P-107 NEGATIVE ASPECTS OF CENTRAL VENOUS CATHETERIZATIONS IN PEDIATRIC ONCOLOGY: SHOCKING ASIA. PART II
M.Y. Rykov
Institute of Pediatric Oncology and Hematology N.N. Blokhin, Moscow, Russia
Background: Catheterization of subclavian vein - a common but dangerous procedure which requires the use of general anesthesia in children. Unfortunately, in Russia, it is the most popular way of chemotherapy.
Materials and methods: From 2010 to 2015 we observed 1857 cancer patients aged 2 months to 17 years, who were installed 4428 subclavian catheters for the purpose of chemotherapy, that is, each patient had 2.3 catheterizations of subclavian vein.
Results: The operating time of catheters ranged from 2 hours to 13 months. The minimum time is explained by frequent self-removal of a catheter by children - 348 cases (7.85%). From the first attempt we managed to puncture the subclavian vein in 3117 cases (70.4%), of which the successful catheterization rom the first attempt succeeded in 2650 patients (85.0%), from the second - 127 (4.0%), 340 (10.9%) required repeated puncture of the subclavian vein. In 543 cases (12.2%) we managed to perform catheterization of the subclavian vein only from the third attempt. In 32 cases (0.72%) catheterization of subclavian vein failed. In 613 cases (13.8%), there was migration of the distal end of the catheter to the internal jugular vein in 74 (1.67%) - to subclavian vein on the opposite side. Pneumothorax complicated catheterization in 29 cases (0.65%), the injury of the lung - in 7 (0.15%). Unintentional puncture of the subclavian artery was observed in 234 cases (5.28%). Catheter-related bloodstream infections developed in 316 cases (7.14%), catheter thrombosis - in 1832 (41.3%) that in 1213 cases (66.2%) required replacement. The destruction of the subclavian catheter outer part was noted in 43 cases (0.97%).
Conclusions: Taking into the account that chemotherapy usually lasts for at least 5 days with an interval of 21 days, using a subclavian catheter is not appropriate and is accompanied by many complications.
Subclavian venous catheter and an implantable port in one patient.
The guide wire is in v. cava.
P-108 THE VALUE OF PROFESSIONAL BOARD CERTIFICATION IN VASCULAR ACCESS
J.H. Garrett
PDI, Atlanta, USA
Vascular Access is a specialty that impacts almost every patient that has a healthcare encounter in both inpatient and outpatient settings. The specialty is comprehensive and requires a comprehensive knowledge base to properly care for today's patient population. Vascular Access as a specialty continues to evolve to meet the complex healthcare needs of today's patients with extensive comorbidities and medical needs. Because of the comprehensive nature of vascular access practices, the need for professional board certification arose from extensive market analysis and to meet the professional development and advancement needs of clinicians responsible for vascular access care. In 2010, the Vascular Access Certification Corporation was formed to conduct an extensive practice analysis, develop a rigorous board certification examination, and launch a comprehensive certification representing the vast cognitive knowledge necessary to safely and confidently care for the complex healthcare patient needs that exist. The content is inclusive of vascular access devices, therapies, patient safety, infection prevention and control, research and quality management, patient advocacy, device management, and clinical theory. As of June 2015, over 2,500 clinicians have successfully received board certification in Vascular Access since the launch of the professional board certification. These individuals represent many professional disciplines including nurses, physicians, respiratory therapists, EMS professionals, medical science liaisons, nurse practitioners, physician assistants, and more. Patients have high expectations for their care, and most patients receive some form of vascular access therapy during their hospitalization or patient care experience. Certified professionals in many healthcare fields such as nursing have been proven to provide higher levels of care compared to those that were not certified. Professional certification in one's specialty also provides for career advancement and professional recognition by employers and patients. Professional Certification positively impacts patient care, improves outcomes, and increases professional recognition and advancement potential for Vascular Access Clinicians.
P-109 UNDERSTANDING LEVELS RESEARCH AND EVIDENCE WHEN MAKING PRACTICE DECISIONS
A.D. Grosklags
Bard Access Systems, Salt Lake City, USA
Research is performed and published in many formats ever day. As vascular access professionals we make practice decisions and decisions for our patients on the evidence which is presented from this research. The CDC, CVAA, RCN, INS, ONS, SIR, AVA and multiple other organizations publish standards which vascular access professionals routinely base their decisions. There is a hierarchy of evidence and types of studies which should be considered when evaluating research. Some standards are based on high levels of evidence and some on low levels of evidence. This lecture will discuss the levels of evidence, types of research, peer review, and valid scientific data to consider prior to making practice decisions.
P-110 CENTRAL-LINE ASSOCIATED BLOODSTREAM INFECTIONS IN NON-ICU INPATIENT: A 1-YEAR ANALYSIS OF A PRIVATE HOSPITAL IN SOUTH BRAZIL
J.S. Flor, L.B. Finatto, C.T.S. Kawski, I.M. Schneider, R. Marco, D. Wiltgen, J. Cogo
Hospital Moinhos de Vento, Porto Alegre, Brazil
Introduction: Catheter associated bloodstream Infection (CLABSI) is a major concern in hospitalized patients. In recent years, the use of peripherally inserted central catheters (PICCs) has increased as an alternative to central line catheters (CVC), largely due to their comparative ease of insertion and perceived safety. However the magnitude of reduction in infection rates compared to CVCs is still unknown.
Methodology: We performed CLABSI analyzes in incident cases during 2015 in medical/surgical non-ICU wards at a private hospital in south Brazil. The final definition of catheter insertion is on call of the attending physician, although there is a group of specialized nurses responsible for PICC insertion. The rates of CLABSI were calculated per catheter-day. According the 2013 publication of the National Healthcare Safety Network (NHSN), the expected average infection rates in wards with similar characteristics is 0.9/1000 catheter-day.
Results: During the analyzed period were recorded 15,832 catheters-day. Of these, 51 patients developed CLABSI: 40 related to central-line (12,444 catheter-day) and 11 related to PICC (PICC 3,388 catheter-day). Most incident microorganisms were Coagulase-negative staphylococci (29.4%), followed by gram-negative (Klebsiella sp and Serratia sp 19.6%-9.80%). CLABSI annual average was 3.22%/1000 catheter-day, above the established by NHSN.
Discussion and conclusions: Central line and PICC were similar regarding associated BSI in this one-year follow up. The finding that Coagulase-negative staphylococci is the most prevalent isolate suggests that aseptic technique breaks may occur during catheters manipulation. Reinforcement of correct catheter manipulation seems to be the goal to reduce infection rates, regardless of type of insertion.
P-111 THE CATHETER TEAM AND ‘D DAY OF CARE’: ACTION THAT PRIORITIZE THE SAFE USE OF CATHETERS IN HOSPITAL IN BRAZIL
J.S. Flor, L.B. Finatto, C.T.S. Kawski, D. Wiltgen, J. Cogo, C.V. Carneiro
Hospital Moinhos de Vento, Porto Alegre, Brazil
Introduction: Hospital Moinhos de Vento is a 380 bed hospital in south Brazil, with 17 operating rooms, 69 intensive care beds (31 adult, 11 pediatric and 27 neonatal) and emergency department. Since 2013, a group of specialized nurses (the “Catheter team”) is responsible for checking all patients admitted with catheters of any kind. The “Catheter Team” evaluate the site of insertion, dressings and advocate best practices in infusion therapy. The Team is also responsible for proceeding training in service for all healthcare workers about complications associated with catheters.
Methods: Recently the Team has developed an activity called the ‘D’ day, when all patients with catheters of any kind (peripheral and/or central venous catheter) were visited in order to observe, in a single day, all variables of relevance in care of catheters. The day ‘D’ was held on 06.22.2015.
Results: On this day there were 294 patients admitted to the institution and 89.12% were using one or more catheters. The prevalence of inadequacies was 24% in all patients with catheters: 77% related to dressing, 15% related to identification and 8% related to the site of insertion.
Discussion and conclusions: Our study showed that active surveillance is useful to identify the most common problems associated to catheters care. After this day, an extensive educational and practical training was made with all healthcare workers to check all about the routine of dressings. We have planned to systematically repeat the “D day” for good care of catheters in the next year.
P-112 PERIPHERALLY INSERTED CENTRAL CATHETER (PICC)TEAM IMPLEMENTATION IN A PRIVATE HOSPITAL IN SOUTH BRAZIL
J.S. Flor, L.B. Finatto, D. Wiltgen, J. Cogo, C.V. Carneiro, C.T.S. Kawski
Hospital Moinhos de Vento, Porto Alegre, Brazil
Introduction: The use of peripherally inserted central catheters (PICCs) has increased substantially within hospitals during the past several years. In 2013, Hospital Moinhos de Vento, a 380 bed tertiary hospital in south Brazil designated a group of nurses to constitute the ‘PICC team” (specially trained nurses who are responsible for PICC insertions at a hospital). The objective of this study was to measure the prevalence of PICC insertion between years 2013 and 2015, after structuring this team, and identifying the main reasons to choose PICC instead of central-line venous catheter.
Methods: Data was retrieved from the procedure spreadsheet fulfilled by the PICC team between years 2013 and 2015.
Results: A total of 111 PICC were inserted in 2013, 131 in 2014 and 172 in 2015, showing a progressive increase of insertion rate (18% between 2013 and 2014 and 31.29% between 2014 and 2015). The most prevalent indication for PICC insertion was antibiotics administration (84%), followed by chemotherapy infusion (9%) and total parenteral nutrition (TPN) infusion (4%).
Discussion and conclusions: Gradually the PICC team is promoting the culture of this kind of catheter in hospitalized patients, specially in cases in which a longer hospital stay/intravenous treatment is previewed. However, definitive information about safety and risk of infection associated to PICC is still to be determined.
P-113 THE IDENTIFICATION OF THE PATHWAYS OF THE VENOUS CATHETER AS SECURELY IN ASSISTING THE PATIENT IN A HOSPITAL IN BRAZIL
Introduction: Errors compared to medication administration events are subject to severe damage may cause adverse outcomes for both the patient and the professionals involved. The constant search for processes that minimize these events are very important for ensuring a safe in health care. Errors with respect to drug delivery routes may be reduced when in a process to correctly identify the administration form and route of administration of the drug.
Methodology: In a hospital in southern Brazil, where 84% of hospitalized patients have venous access, whether peripheral or central, we developed a system for the identification of drug administration routes where visually through labels can differentiate peripheral intravenous and central intravenous from other routes, such as nasogastric tube for example.
Results and conclusions: By implementing this method was created over a safety barrier, to thereby minimize the error resulting from the administration of drugs by the wrong route. In inspections carried out by infusional team of this hospital is possible to identify 100% of accesses are marked with these labels, therefore we can visually identify the pathways of both peripheral venous access as central.
P-114 IMPORTANCE OF KNOWLEDGE IN THE DEVELOPMENT OF COMPETENCES FOR THE USE OF THE PERIPHERALLY INSERTED CENTRAL CATHETER - PICC
L.M. Braga1, P.M.S.D. Parreira1, A.S. Salgueiro-Oliveira1, M.A.P. Henriques1, C. Arreguy-Sena1
1Universidade Federal de Viçosa-MG, Viçosa, Brazil; 1Escola Superior de Enfermagem de Coimbra, Coimbra, Portugal; 1Escola Superior de Enfermagem de Lisboa, Lisboa, Portugal; 1Universidade Federal de Juiz de Fora-MG, Juiz de Fora, Brazil
Introduction: In the face of increase of life expectancy and advances in diagnosis and therapy methods, providing confident venous accesses has become important. To meet these needs, the peripherally inserted central catheter (PICC) has been used throughout the world, however it does not have the same usage in adults in Portugal. In the face of international recommendations regarding indications for the insertion of venous catheters and the evidence of vascular trauma related to peripheral venous catheters, research was carried out to identify the Portuguese nurses' knowledge of the PICC in adults.
Methods: Descriptive study, that administered a questionnaire to 23 nurses of a Portuguese medicine service. Ethical requirements were met.
Results: The level of knowledge regarding PICC (obtained by summing the right answers) reached an average of 15.59 with standard deviation of 5.7, ranging between zero and 24 (maximum 30 points). The items that presented a percentage of wrong answer exceeding 30% were: regarding pre-insertion skin preparation (83.3%); in the choice of catheter diameter (55.6%); in catheter length to be inserted (33.3%); indications for insertion (52.9%); in time of permanence (77.8%); in the position of the catheter tip (55.6%); in the technique for unblocking (72.2%).
Discussion: The technical and scientific knowledge not demonstrated by nurses indicates a need for developing competences in this context that could aid the decision on the choice of venous catheter and thus reduce complication rate, in addition to being able to influence the time of permanence, the correct assessment between the diameter of the vein and the catheter, the insertion technique and positioning of the tip of the device, fixation technique and catheter maintenance.
Conclusions: The results showed a lack of knowledge on aspects related with placement, maintenance and monitoring of the PICC, indicating the need of training for the acquisition of specific competences.
P-115 VALIDATION OF NURSING INTERVENTIONS FOR THE PREVENTION OF PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) OBSTRUCTION IN NEWBORNS
L.M. Braga1, C. Arreguy-Sena1, P.M.S.D. Parreira1, A.B. Penna1, M.D.L. Correia1
1Universidade Federal de Viçosa-MG, Viçosa, Brazil; 1Universidade Federal de Juiz de Fora-MG, Juiz de Fora, Brazil; 1Escola Superior de Enfermagem de Coimbra, Coimbra, Portugal; 1Hospital das Clínicas da Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
Introduction: Obstruction is one of the commonest complications related to Peripherally Inserted Central Catheters (PICC), which is the responsibility of nurses to prevent. Research was performed to evaluate nursing interventions related to the prevention of PICC obstruction in newborns.
Methodology: Descriptive study using a validation model with a questionnaire and Likert type scale evaluation. The questionnaire was administered to 38 Brazilian nurses who worked for more than a year in the Neonatal/Pediatric Intensive Care Unit (ICU/Neo) and who participated in a course for the insertion/use of PICC. Ethical requirements were met.
Results: Most of the nurses had more than two years' experience in ICU/Neo (70.3%) and all performed PICC maintenance interventions. The nurses considered the following interventions fully or substantially indicated (≥80%): maintaining positive infusion pump pressure; saline solution flushing before/after administering medication; sterile water flushing before/after phenytoin; not administering hemocomponents in PICC ≤4 Fr; not collecting blood in PICC ≤4 Fr. There was no consensus: on the frequency of flushing, in the administration of the phenytoin by PICC and heparin flushing.
Discussion: Obstruction is up to 30% of PICC related complications and flushing is the most indicated preventive intervention. Some protocols recommend flushing in regular intervals, however there is no evidence available on the frequency, having not been possible to validate this intervention, because there was no consensus among the nurses. Phenytoin has been linked to precipitation-related obstruction and the presence of the saline solution could be one of the risk factors that justify the use of sterile water, according to the nurses' opinion. The nurses' clinical practice also confirms other evidence that contraindicated collection and administration of hemocomponentes by PICC ≤4 Fr.
Conclusions: The study allowed validating eight nursing interventions for obstruction prevention. Other studies must be conducted to enlarge validation in Brazil and other countries.
P-116 IMPLEMENTATION OF VASCULAR ACCESS MEDICAL TEAM AS A WAY TO REACH BEST ASSISTANCE IN A GENERAL HOSPITAL SÃO PAULO, BRAZIL
1PVP Medical Services, Sao Paulo, Brazil; 1SESV Especialized Vascular Solutions, Sao Paulo, Brazil
Introduction: Due to particularities of the additional health system in Brazil, hospitals serving this category have difficulty maintaining their own staff dedicated to the insertion and maintenance of accesses. While the nursing staff is employed by the hospital, physicians are outsourced service providers. The health insurance does not pay for nursing services as it pays for medical services. This has opened an opportunity to create a team of proficient physicians in indication, insertion and maintenance of all vascular accesses.
Methods: The team consists of six medical officers with expertise in vascular surgery, and following narrow protocols in indication and implementation of accesses, with 100% of ultrasound-guided punctures. We made records of all accesses inserted by this team in 2014 and 2015, as well as the registration of complications on the use of accesses.
Results: There was an increase of PICC deployment from 2 to 120 per month, with a concomitant decline in use of short term jugular and subclavian catheters (except dialysis catheters) from 15 to 4 per month (270 beds). The total amount of accesses deployed over 2 years was 1786, with only four arterial puncture accidents (0.2%), no pulmonary accident or fatality. Of total accesses deployed, 95% were being used by the end of the proposed therapy. Catheter related symptomatic venous thrombosis has occurred in 1.7%.
Conclusions: In the health insurance system in Brazil, it is feasible to form specialized medical staff in vascular accesses, and its implementation brings good results of safety and comfort to patients. In this registry, we show the evolution in the quality of patient care after the implementation of dedicated staff to vascular access.
P-117 TYPES OF VASCULAR ACCESS IN MENTAL HEALTH ENVIRONMENT, SPECIAL CONSIDERATIONS FOR PROFESSIONALS
J.C. De la Torre-Montero1, P. Plaza-Zamora1, N. Andújar-Espada1, P. Fernández-Velasco1, L. Rozalén-Quintano1, R.M. Fernández-Ayuso1
1Comillas Pontifical University, Madrid, Spain; 1San Juan de Dios Mental Health Centre, Ciempozuelos, Madrid, Spain
Introduction: One of the most prominent fields in mental health pathology during the last years has been the demystification in society and the integration of the patient with mental pathology within the overall-holistic provided care.
Although this is happening we should not remain oblivious to some considerations regarding the patient and professional's safety when dealing with venous access.
Methods: The main objective of the study was to identify the topics which is defined differently in the mental health patient cases about vascular access, with a cross-sectorial perspective, and to assess whether those differences might lead to an inconsistent implementation of new lines of cares.
It is created a series of questions directed to health providers specialized in mental health with experience in hospitalization, in the Europe's largest Mental Health Hospital, with up to 1200 places.
Results: The results have validated the initial hypothesis where we identity three clear points regarding the needs from patients with mental pathology: have bio-safety equipment used by professionals in charge of those patients; to know containment measures and to design protocols suitable for the management of intravenous equipment.
Discussion and conclusions: From the patient global care perspective, the medical attention in mental health is the key to manage the different conditions that happen within the mental health environment.
Taking into consideration the experts' assessments, we think it is necessary to adopt measures directed to:
the management of mechanic containment corresponding to the specific and limited areas of venous access; the knowledge of bio-safety equipment suitable for this specific environment; improve the specific protocols in this field regarding the care of the venous access.
P-118 EFFECTIVE STRATEGY TO KEEP THE PERIPHERALLY INSERTED CENTRAL CATHETERS PATENCY
T.C. Silva
Sociedade Beneficente de Senhoras Hospital Sírio Libanês, São Paulo, Brazil
Peripherally inserted central catheters have been widespread among venous access devices. Studies have shown that vascular nurses teams, have contributed to decrease complications and blood stream infection. Currently, there are different catheters available, such as valved and non-valved tip. Studies have showed a significant reduction in valved tip catheters occlusion rates when compared to non-valved. The objective of this study is to define strategies to ensure patency of non-valved tip peripherally inserted central catheters through interventions carried out by the vascular nurse team. Early identification of adverse events was important for the proper maintenance, troubleshooting and ensuring good results until the end of venous therapy. This study was developed in a private hospital. We designed a strategy using all catheters of hospitalized patient in 2 weekly. The catheter patency test was conducted, and the, dressing conditions, search of early deep vein thrombosis and infection signs and symptoms, were performed chest X-ray to confirm tip position and possible early removal was evaluated. During the study period, the average of catheters in use was of 160 catheters per day, with occlusion and no possibility of blood drawing of 5 cases per day. An individual evaluation was performed to identify patency problems with saline solution flush to restore catheter patency. After the study period, was possible to decrease 50% of malfunction cases, from 5 to 2.5. These outcomes have proved that, this strategy is effective to reduce occlusions event and impact on the therapy quality. During the study, we identified some cases of total occlusion, not possible to flush with saline, a fibrinolytic was needed and this catheter was excluded. We conclude that the vascular nurse team has been a very important and effective strategy to get good outcomes, reduce catheter malfunction, and increase nursing staff, medical and patient satisfaction.
P-119 ECONOMIC IMPACT OF PERIPHERALLY INSERTED CENTRAL CATHETER CHEMICAL CLEANING
T.C. Silva, M.J. Poltronieri
Sociedade Beneficente de Senhoras Hospital Sírio Libanês, São Paulo, Brazil
Peripherally inserted central catheter is expanding due to the positive outcomes, but there is a high risk of occlusion when compared to the valved tip catheter. The early identification of adverse event is important however when a catheter occlusion by clots occurs, a fibrinolytic is needed. The objective of this study is to define the cost and economic impact of chemical cleaning performed by vascular nurse team, as the cost is lower with chemical cleaning when compared to a new PICC placement. This study was performed from June 1st, 2015 to December 1st, 2015 in a private hospital located in São Paulo, Brazil. During this period, a total of 1203 non-valved high power infusion catethers was placed, and 89 required chemical cleaning. The fibrinolytic of choice was Urokinase 10 mg at a concentration of 2 mg/ml with. The catheter size was 5 and 6 Fr. The Urokinase in our hospital is handled exclusively by a vascular access team nurse and the use is based on a protocol validated by the technical board. This fibrinolytic has a cost of $ 74,25, disposables: $ 1,01 and nursing procedure fee of $ 29,70 amounting to a total of $ 104,96 per catheter. For a new PICC placement, the procedure value was $ 1.237,62 when placed by the bedside. A total of 89 catheters was included in this study, 98% achieved satisfactory outcomes of catheter patency on the first intervention with no complications or systemic bleeding, regardless of the platelet count or coagulation changes. We conclude that the chemical cleaning with Urokinase had a total cost of $ 9.341,44 and could represent a significant impact on cost reduction when compared to a new PICC placement that would represent a total cost of $ 110.148,18 for the 89 cases in this study.
P-120 TRAINING AND IMPLEMENTATION OF PICC TEAM OF THE HOSPITAL SÍRIO LIBANÊS-2011
T.C. Silva
Sociedade Beneficente de Senhoras Hospital Sírio Libanês, São Paulo, Brazil
A team of nurses trained and dedicated to the insertion and maintenance of PICC can reduce costs, optimize the time of the nursing staff, reduce bloodstream infection rates and reduce complications related to the usage of a PICC line. This study is an experience report. After the initial process, seven nurses were selected, and all have achieved an average score of more than eight in e-learning training and practical training with dolls and pigs. During the period from July 22, 2011 to December 31, 2011 were 103 PICC placements were requested, however, 23 were contraindicated, 78 were successfully inserted and 25 were procedure failures. At this early stage, the number of contraindications reached 25% due to the limitation of the conventional technique in performing venipuncture successfully. At the end of the sixth month we noticed a significant increase in requests, reaching 28 requests in December 2011 versus 4 in July of the same year. Planning has become critical to project success. We started developing the institutional protocol, choosing the best device with the technique that offers our customers greater safety and quality. An institutional training was also carried out as this, was a new infusion therapy device in the institution, with different dates and times for all employees and promoted to all clinical staff. The result of this process was the addition of a new device that can be used with different types of treatments, bringing more safety and comfort with low rates of complications related to PICC.
P-121 ANALYSIS OF CENTRAL VENOUS CATHETER CHECKLIST
D.S.H. Bikkulova
Dmitry Rogachev Federal Research Centre of Pediatric Hematology, Oncology and Im, Moscow, Russia
A safe insertion of all types of central venous catheters (CVC) has always been of vital importance. There are some factors such as the rotation of employees, the introduction of new types of catheters, a change in preferences of treating physicians when choosing a central venous access device that can affect this process. In order to ensure a patient's safety and to control the situation, it is important to use CVC checklists.
In our Center CVC insertion is performed by anesthesiologists. Since 2013 till 2015 checklists have been completed annually, from February till May.
806 checklists have been analyzed. The age range of patients with hematological and oncological diseases is 2 months - 18 years old. Year in, year out the number of CVC insertion procedures has been increasing, the proportion of catheters types used has been changing. For instance, in 2013 long-term CVCs were inserted into the subclavian or the internal jugular vein. Nowadays, long-term CVCs inserted only into the internal jugular vein, whereas short-term CVCs - only into the subclavian vein. In 2014 some cases of repeated puncturing of the subclavian vein. Analysis showed that the puncture site and the direction of the needle had been incorrect. We changed the technique of the procedure. In 2015 there were 78 cases of CVC substitution. The reasons were accidental removal of CVC by a patient (22 cases), thrombosis (13), infection (11). Accidental catheter removal was observed in adolescents - we wrote a brochure about CVC for adolescents. In addition a recertification of the staff as well as training for nurses, etc. were carried out. A regular analysis of checklists allows one to identify mistakes in work as well as helps to improve the organizational activity of the hospital administration.
P-122 PERIPHERALLY INSERTED CENTRAL CATHETERS IN PEDIATRIC ONCOLOGY PATIENT IN A TERTIARY CARE SETTING IN BRAZIL: NEW PERSPECTIVE FOR LINE INSERTIONS
Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, Brazil
Introduction: Peripherally inserted central venous catheters (PICC) have been successfully used to provide central access for chemotherapy in developed countries. The purpose of this study was to assess the feasibility of PICCs and determine PICC-related complications in pediatric oncology patients in a hospital in southern Brazil before and after implementation of a vascular access team (VAT).
Methods: All oncologic pediatric patients who underwent PICC line insertion at the Santo Antonio Children's Hospital de Porto Alegre from January 2015 to December 2015 were enrolled. Between January to August 2015 PICCs were inserted by non-dedicated per diem nurses whereas all PICCs insertions from September on were performed by the VAT.
Results: A total of 27 PICCs were placed in 25 children during the period. The 27 PICCs were in place for a total 2145 catheter-days (median time, 79 days; range, 1 to 241 days). The 27 PICCs had 9 overall complications, for a rate of 4.20/1000 catheter-days. Four central line-associated bloodstream infection (CLABSI) occurred (incidence rate, 1.86 cases per 1000 catheter-days). The most common reason for PICCs removal was CLABSI (14.8%) and irritant contact dermatites (7.4%). After the implementation of a VAT, the numbers of catheters inserted by the team increased by 45% and an insertion success rate of 94% at bedside was achieved.
Discussion and conclusions: PICCs are feasible in a developing country scenario for chemotherapy administration and prolonged venous access. Trained nurses from VAT who places PICCs almost daily with high-tech achieved over 90% insertion success. The study found that a VAT PICC placement for infusion therapies was effective and safe with relatively low complication rates and that a VAT played important roles in the increased use of PICCs in oncology pediatric patient in our hospital. CLABSI was the most significant complication. Efforts in prevention should be warranted.
P-123 MEDICAL ADHESIVE-RELATED SKIN INJURY IN ONCOLOGY PEDIATRIC PATIENT WITH PERIPHERALLY INSERTED CENTRAL CATHETERS: A CASE SERIES
Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, Brazil
Introduction: Medical adhesive-related skin injury (MARSI) is a prevalent but frequently underreported complication since it is not currently categorized as an adverse event. Repeated exposure to topical chlorhexidine gluconate and various types of medical adhesive used as catheters insertion site dressings can lead to irritant contact dermatites (ICD), a common type of MARSI. The complication is also favored by improper technique during application and/or removal of adhesive products. MARSI hampers patient safety, quality of life and increases healthcare costs.
Methods: Hereby we report 4 oncology pediatric patient with PICC who developed ICD during dressings changes.
Results: All four oncology pediatric patient with PICC presented with a scalded skin appearance (burn) with papules and/or vesicles on an erythematous patchy background with weeping and/or edema present. Lesions were often preceded by a burning sensation in the area when exposed to 0.5% chlorhexidine gluconate (CHG) in an alcohol solution to cleanse the skin around the PICC insertion site during dressing changes. We identified that the skin decontamination product had not been correctly apply, since it had not been allow to dry completely before the application of the standard dressing. Removal process of the dressing was also deemed inadequate. The treatment include the elimination of contact with irritants most likely involved (CHG and transparent semipermeable dressing) followed by substitution of the topical antiseptic and the transparent semipermeable dressing by another antiseptic and sterile gauze. Finally, we altered the dressing protocol, introducing the application of a Cavilon No Sting Barrier Film® (size 1 ml wipe) under dressing to cover the catheter sites for all PICC inserted.
Discussion and conclusions: MARSI is an often overlooked, frequent complication with impact in quality of life and costs. Alteration in change dressing protocol decreased the MARSI in our patients.
Dmitry Rogachev Federal Research Centre of Pediatric Hematology, Oncology and Immunology, Moscow, Russia
The correct maintain of venous access devices provides their safety and irreproachable capacity for work. Modern techniques with use of a catheter presented by the colleagues in some publications are confirmed by research.
However, it's important for staffs to understand that laws of physics occur in the basis of each position.
We present some comments for mannual action of the medical staff on maintainance of a catheter in the basis of which there are laws of mechanics and hydrodynamics.
Prevention of occlusion of a catheter: flushing the catheter using the technique ‘start-stop’ creates the turbulent flows of liquid into the lumen of the catheter providing the best effect. The non-stop piston preassure in the syringe creates laminar flows of liquid in the catheter and as a result- unsatisfactory effect with using even more liquid.
Prevention of thrombosis going inside the catheter. After infusion, flushing the catheter it's important to close timely the clamp of the catheter. There are two tecniques here - consistent and simultaneous. The first one has 3 items: 1-flushing, 2- releasing the syringe piston from a hand of nurse, 3-closing the clamp. Item 2 according to the laws of applied mechanics - ‘intervention force is equal to anti-intervention force’ creates the risk of return current of the blood into the lumen of the cathater. The simultaneous technique has 1 item - pressing the syringe piston with one hand and at the same time closing the catheter clamp with the other hand. We have also other laws of physics at the heart of work with a catheter.
Mastering modern techniques of exploitation venous catheters and understanding the laws of Nature which are in the basis of these techniques assist to improve physicians' qualification and decrease the ammount of complications when using CVC.
P-125 CENTRAL VENOUS ACCESS DEVICE SITE CARE AND DRESSING CHANGE COMPETENCY: AN EXPERIENCE IN SOUTHERN BRAZIL
Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, Brazil
Introduction: Central venous access devices (CVAD) are essential for care of inpatients requiring fluids, eletrolytes, medications, parenteral nutrition and blood products. Maintenance of insertion sites dressing integrity and occlusivity and performing adequate site desinfection during dressing changes are critical in preventing extra-luminal colonization and subsequent Catheter-Related Bloodstream Infections (CRBSI). Competency-based education using low-fidelity simulation was found to improve competency in nursing practice leading to safer care, less hospital-acquired infections, and cost savings for the patient and the healthcare organization. This study evaluated the impact of a competency-based education on central line maintenance and care among a group of nurses from an adult's hospital in Southern Brazil.
Methods: The setting of this study was the Pavilhão Pereira Filho Hospital at the Santa Casa de Misericórdia de Porto Alegre. The competency-based education occurred in October and November 2015 in our hospital. The Vascular Access Team (VAT) developed and applied a questionnaire to all nurses who accessing CVAD. The nurses were required to demonstrate theoretical knowledge in this questionnaire and were also required to demonstrate practical competency in performing CVAD site care and dressing changes using a simulator.
Results: Thirty nurses completed assessment and training in CVAD site care and dressing changes in the simulation laboratory. The adequation scores ranged from of 73.0% to 100% with an average of 89%.
Discussion and conclusions: The nurses displayed large variability in their ability to perform central line maintenance tasks. After competency-based education, there was significant improvement, and all nurses reached a predetermined level of competency.
P-126 SUCCESSFUL CONTROL OF INFECTION OF DIALYSIS CATHETERS IN INTENSIVE CARE UNIT
J. Perme, A.J. Jaklic
University medical center Ljubljana, Ljubljana, Slovenia
In the intensive care unit at the Clinic for infectious diseases and febrile conditions (ICU) patients with severe infections and failure of most organ systems are treated, including kidney failure. In the unit intermittent and continuous hemodialysis and plasmapheresis is performed.
The investigation was divided into two parts. In the first part, we have not implemented any measures. Dressing was carried out only on dialysis for three or more days, there was no daily inspection of the catheter insertion site. Dressing was implemented with disinfectant soap and alcohol. The insertion site has been covered with gaze and before coverage, antibiotic ointment was applied to the insertion site. The majority of dialysis catheters were inserted in the femoral region. In the second period, we have taken measures for care of dialysis catheters. Dressing of the insertions site was performed with 2% chlorhexidine in 70% ethanol. The insertion site was covered with hydrogel gaze soaked with chlorhexidine, which allowed daily control of the insertion site. Dressing was changed every 7 days. Antibiotic ointments were not used. The process of dialysis remained unchanged, using the same dialysis. Most catheters were inserted femoral.
Results in the pre-interventional period: 34 catheters were inserted, 477 catheter days. 8 infections were recorded, which is 16.8/1000 catheter days, of which 2 were local infections 4.2/1000 catheter days and 6 were system infections 12.6/1000 catheter days.
The results of the intervention period: 86 dialysis catheters were inserted, 828 catheter days. 3 infections were recorded, 3.6/1000 catheter days, one local and two systemic infections 2.4/1000 catheter days.
In our unit we have demonstrated that with implementation of modern international recommendations for the care of the central vascular catheters, it was possible to successfully control also infection of dialysis catheters, despite unfavorable anatomic site.
P-127 THE BEWARE OF VASCULAR ACCESS IN CHILDREN WITH CANCER: THE PLAYFUL AND THE EDUCATIONAL PROCESS
K. Mesquita, C.R. Magalhães, S.T. Canabarro
Universidade Federal de Ciências da Saúde Porto Alegre, Porto Alegre, Brazil
Introduction: In Brazil, the cancer mortality in children and adolescents aged 1 to 18, comprising the fourth leading cause of death from cancer. For the completion of chemotherapy, need is a venous access for infusion of anticancer drugs. The intravenous route is known that it is more secure, since it chooses a device suitable for intravenous administration. In such cases, the central venous catheter indwelling, is the most suitable for infusional therapy of cancer patients. It is known that hospitalization brings deprivation being with his brothers and/or colleagues, the distance from home and their favorite toys, the experience of pain, guilt and fear among other sentiments expressed by the children in the hospital. Understanding the context that children with cancer experiences due to hospitalization, and that requires a long-term central venous access for their treatment and knowing that the intrusive procedures for obtaining a route venous causes tension, fears and anxieties. It is necessary to investigate whether the recreational activity may contribute to the implementation of the educational process in children with vascular access.
Methodology: This is an Integrative Review (RI), through literature searches. Data collection was carried out between October and November 2015. We carried out the survey of scientific literature indexed in the databases of the virtual library Scientific Electronic Library Online (SciELO) and Data Nursing (BDENF).
Results: We analyzed 715 articles that after reading in full and submission to defined inclusion and exclusion criteria resulted in 28 articles that were used in the study.
Discussion and conclusions: The data analysis led to the identification of two categories: recreational practices with hospitalized children and play in children with cancer.
P-128 A PROSPECTIVE STUDY OF PLACEMENT AND CONFIRMATION OF PICC'S TIP POSITION USING A MAGNETIC TRACKING AND ELECTROGRAPHIC METHOD
Background/purpose: Atrio-cava junction is the best position for central venous catheters (CVC). Fluoroscopy is still the reference to place PICC in France. The endocavitary ECG method has proven to be useful in obtaining atrio-cava junction tip position. The aim of this study was to evaluate the interest of using magnetic tracking and ECG confirmation (Sherlock 3CG) combined with ultrasonography in PICC placement instead of perioperative fluoroscopy.
Methods: During 6 months, all adult patients from a French cancer center undergoing a PICC placement using ultrasound and the SHERLOCK 3CG device were included in this prospective study. The primary objective was to study the success rate of PICC placement using Sherlock 3CG. Failure was defined as need of fluoroscopy or more than 3 punctures to achieve PICC application or whole procedure failure. Secondary objectives were to describe conditions of CVC placement.
Results: From October 2013 to April 2014, 544 PICC applications were performed in 510 patients (34 patients had 2 procedures): 50.2% males, median age of 61 years (range: 18-89). 37.8% (n = 201) of procedures were performed in patients who had previous CVC placement. PICC were inserted on the right side in 71.9% of cases; through basilica or brachial vein in 65% and 35%, respectively.
Sherlock 3CG success rate was 94.8% (95% CI: 92.6-96.5). Failures were associated with fluoroscopy use (3.3%, n = 18, median dose: 28.30 cGy/cm1 (3.60-681.60)), need of more than 3 punctures (1.3%, n = 7) or whole procedure failure (2%, n = 11); due to incidental findings of thrombosis or stenosis in 6 cases.
Maximum pain during procedure (Verbal Analogic Scale) reached 1.05/10 in median (0-7). No tip was above the carena, 1.7% (n = 9) were close to the third vertebra under the carena.
Conclusions: The high success rate obtained with Sherlock 3CG for PICC placement support that it could be a good alternative to fluoroscopy.
P-129 IMPROVEMENT OF PATIENT SAFETY ACCESS - AGGREGATION OF CVC INSERTION AND LICENSE SYSTEM AT CVC CENTER - FOLLOW-UP REPORT
J.O. Oda
Tokyo Medical University, Tokyo, Japan
Introduction: In our university hospital with 1,015 beds, we established a CV Catheterization Center in August, 2005 and also introduced a license system for CVC placements in order to prevent serious complications with CV catheterization. We organized a multidisciplinary CVC committee for the purpose of management, establishing rule of catheterization and checking all catheterization procedures.
Methods: All CVC catheterization procedures had to be reported in proper form. We defined and revised guideline for catheterization for entire hospital, and catheterization center for all patients in entire hospital except ER, OR, and ICU. We managed CVC lecture, skill test, and instituted license/registration system. Our guideline required operators to use ultrasonography to confirm the vein, to catheterize using fluoroscope, to check blood gas analysis of catheter blood, to confirm backflow, and conduct 2 X-ray exams soon after and 4-6 hours after catheterization. We restricted the placers from puncturing the vein to 3 times, at maximum as a rule.
Results: Over 15,000 catheterizations have been registered in 10 years. The number of catheterizations is approximately 1,300 per year. Only 7% of patients were catheterized in general ward, with acceptable reasons for not moving to CVC center as severe condition, monitoring requirement, sudden change, and infection. The purpose of approximately 7,000 CVC catheterizations were TPN and/or chemotherapy, they seem potentially to switch to PICC. Less than 5% of patients suffered from minor complications. Incidence of complication with accident level 3b or more reduced to 0.7% of all patients. Over 3 times puncture increased risk of complication. Over 60 minutes procedure increased complication rate to over 20%. Half of pneumothorax or pleural space infusion was found by later x-ray.
Discussion and conclusions: Aggregation into CV Catheterization center, registration system, and rules above are important for patient safety access for CVC.
P-130 BI-DIRECTIONAL NEEDLESS DEVICES TO PREVENT INTRALUMINAL OCCLUSION IN PERIPHERALLY INSERTED CENTRAL CATHETERS
J.E. Hitchcock
Imperial College Healthcare NHS Trust, London, UK
Introduction: Peripherally inserted central catheters (PICCs) are used in a variety of specialities delivering diverse range of treatment. Infective and thrombotic complications are widely reported, however little is written about the complications of persistent withdrawal occlusion (PWO) or complete luminal occlusion in PICCs.
Methods: An audit was conducted of all patients who had a PICC insitu for a 6 week period, in all clinical settings using a combination of reviewing clinical documentation, local departmental databases, physical review of inpatients and discussing with clinical nurse specialities that saw the patients in haematology, oncology, outpatient parenteral antibiotic therapy and the vascular access team. It was difficult to determine a rate of either PWO or complete occlusion due to the diversity of the patient cohort and the tertiary nature of the organisation, it was estimated the occlusion rate was 5%, there was general agreement this was underestimating the problem.
Results: The introduction of bidirectional device on of the organisations sites that had speciality services of haematology, oncology and hepatobiliary for all PICCS was implemented. 180 PICCs inserted over a twelve month period with a total dwell time of 9702 catheter days, mean dwell 53.9 days, median dwell 35 days saw a PWO rate of 1/1000 catheter days and total occlusion rate of 0.4/1000 catheter days. The time for insertion to complication of PWO or occlusion ranged from 9-144 days.
Discussion: Despite poor baseline data the results suggested the introduction of the bidirectional needleless device had a positive impact on the PWO and occlusion rates in PICCs. The use of heparinised saline and thrombolytic agents decreased significantly, as did premature removal of PICCs.
Conclusions: The bidirectional needleless device has been implemented across the organisation with continued low rates of both PWO and occlusion year on year.
P-131 MEDICAL ADHESIVE RELATED SKIN INJURY (MARSI) - IMPLEMENTING A PREVENTION AND TREATMENT ALGORITHM
J.E. Hitchcock, L. Savine
Imperial College Healthcare NHS Trust, London, UK
Introduction: Establishing vascular access and preventing infection, both at insertion and during on-going care is generally the top priority; the maintenance of optimal skin integrity is often a distant and lesser secondary consideration. Skin can react to types of dressings/adhesive, the securement of lines and the development of sensitivities to cleaning solutions. Clearly, these scenarios are not limited to securement of vascular access devices, however the often precious nature of a long term vascular access device makes this a very important and yet largely unrecognised area.
Methods: A review of the limited literature that existed prior to March 2015 is typically associated with skin tears connected with dressings and removal, and contact irritant dermatitis. The expert knowledge of the tissue viability and vascular access team viewed the current products associated with a typical vascular access dressing to ensure it was fit for purpose and where at all possible had good scientific literature for validation.
We worked proactively to recognise those patients at risk with the early identification of potential MARSI. To facilitate this we have developed an algorithm which offers a step by step approach clearly outlining what to do to prevent MARSI and its treatment should it develop.
Discussion: Through this work, reactions can result from other factors than simply the dressing alone, an increase in these kinds of skin reaction in patients who are on chemotherapy regimens in haematology and oncology cohort; this is something that that is currently exploring further. Validation of our reduction in terms of per catheter days is any area being developed.
Conclusions: Through the implementation of a algorithm, education for both staff and patients and collaborative working between vascular access and tissue viability teams we are seeing a reduction in these phenomena in an increasing number of at risk patients.
P-132 USE AND OUTCOME ANALYSIS OF ULTRASOUND AIDED PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) INSERTIONS IN TERTIARY ONCOLOGICAL SET-UP
R. Naik
HCG Hospital, Bangalore, India
Introduction: It is well established that a PICC is recommended for long term chemotherapy, antibiotic therapy and total parenteral nutrition. In a developing economy like India, it requires consistent efforts in shifting the approach from conservative to modern. This study is an attempt to share our experience of ultrasound guided PICC insertions.
Methods: Fifty subjects requiring chemotherapy, confirmed with malignancy, aged between 14-65 years underwent upper arm PICC insertion with the aid of Ultrasound under sterile conditions. Subsequently they were followed up for a period of ninety days post insertion.
Results: Out of the fifty subjects, twenty six were female. Left basillic vein was preferred insertion site. Cephalic vein insertion in 5 subjects, 14 brachial & 31 basillic vein insertions respectively. The attempts to access the vein were mostly single except for four. The veins were prominently accessed at 1 cm depth. The catheter length in the body ranged between 32-45 cms. The average time of the procedure from venous puncture to dressing the insertion site is about 15.49 mins. Post insertion follow up of 90 days observed that six subjects expired and 2 underwent removal due to successful completion of treatment and 2 removed due to catheter blockage.
Discussion: We have recently incorporated ultrasound guided PICC insertion in our practice and have observed zero infection rates or hematomas. The amount of time to complete the procedure is less due to ultrasound guidance. The number of attempts to get the vascular access is almost once. We have observed that two subject on 5 Fluorouracil had a repeated blockage and underwent catheter replacements.
Conclusions: Our experience with ultrasound guided PICC insertions is successful as it minimizes complications and ensure better safety in cancer patients.
These abstracts have been produced electronically by Wichtig Publishing and are available on the Journal's web site at www.vascular-access.info
Every effort has been made to faithfully reproduce the abstracts as submitted. However, no responsibility is assumed by the organisers as well as by the Publisher for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions or ideas contained in the material herein. Because of the rapid advances in the medical sciences, we recommend that independent verification of diagnoses and drug dosages should be made.