
Abstract
Vascular access preparation in the elderly with advanced kidney disease needs a nuanced approach. Recent studies indicate that age, along with comorbidity, modify the outcomes associated with the type of access placed or used for hemodialysis (HD). Options ranging from permanent vascular access (arteriovenous fistula [AVF] or graft [AVG]) to tunneled central venous catheter (TCVC) or conservative medical care must be weighed on an individual basis and reassessed longitudinally. The potential benefits derived from AVF compared with AVG and TCVC are not always seen in this population. Herein, we review the literature concerning patient and vascular access outcomes in the elderly with advanced kidney disease or on HD. A multidimensional approach that takes into consideration the burden of comorbid diseases, functional status and patient-reported views on quality of life ought to be incorporated in the process of vascular access planning in the elderly.
Elderly with Kidney Disease – Epidemiologic Trends
Advances in medicine, public health and economic developments have added an extra decade of life to the average human lifespan since the early twentieth century (1). Concurrently, the fertility rate dropped by nearly 50% (2). As a result, these two independent and parallel phenomena, elderly adults (age 75 years and older) comprise about 12% of the total population, a fraction projected to increase to nearly a quarter of the world population by 2050. Of the elderly population, the oldest of these (85 years and older) is the fasted growing segment, expected to increase by 351% before 2030 (1). Medical victories in the treatment and prevention of various illnesses have modified the landscape of common diseases and main causes of death: communicable infectious diseases and acute and life-threatening illnesses are more often amenable to effective treatments, giving rise to higher prevalence of chronic diseases such as diabetes mellitus, coronary artery disease, cancer, and stroke (2). Resultant of the demographic and epidemiologic changes, elderly individuals represent the fastest growing group of patients diagnosed with kidney disease. Large community-based retrospective studies revealed that the incidence of dialysis and non-dialysis requiring acute kidney injury (AKI) steadily rose over the last decade, with the steepest rise being present among the elderly (3, 4). Based on large dialysis registries, the annual incident and prevalent rates of end-stage renal disease (ESRD) requiring hemodialysis (HD) has steadily risen in the older age groups, with the highest rise observed among the >85-year-old age group; while the incidence and prevalence of ESRD in younger patients remained uniform. In the USA, the rate of dialysis initiation in the elderly increased by 57% between 1996 and 2003; in France, the number of elderly dialysis patients aged 75-84 rose 10% annually, and dialysis rate doubled in those older than 85 years (5-7).
Preparation for Vascular Access in the Elderly
In light of the aforementioned trends, nephrologists more often encounter older individuals with advanced kidney disease for whom treatment choices, dialysis education and dialysis vascular access need to be addressed.
Among elderly starting HD in the USA, 80% are initiated with a tunneled central venous catheter (TCVC), similar to the overall use of catheters at HD initiation across all ESRD patients; 11% are initiated with a functioning arteriovenous fistula (AVF) and 4% with an arteriovenous graft (AVG) (8). Recent studies uncovered significant heterogeneity in the advantages and disadvantages related to specific vascular access types when age and other comorbidities were considered. In this article we will discuss some of the vascular access challenges and strategies across different stages of chronic kidney disease (CKD) in the elderly for whom HD was elected as a means of ESRD treatment.
Elderly with Pre-dialysis CKD
Two fundamental medical questions that frequently arise in elderly patients who have CKD are if and when to refer for permanent vascular access surgery. Relative to younger population of similar kidney function, elderly with advanced CKD have a much lower rate of kidney function decline (-3.46 mL/min/1.73 m 2 vs. −1.6 mL/min/1.73 m 2 ) and are more likely to die from an unrelated or comorbid illness rather than survive to initiate dialysis (adjusted hazard rate [HR] for mortality 0.75 vs. 2.95 for younger and elderly, respectively) (9, 10). In a European cohort of 177 octogenarians with CKD stage 4 followed for 5 years, 36% did not have progression to later stages of CKD, 64% had further CKD progression, 38% initiated dialysis, and 18% died (11). Discerning which outcome will prevail (death vs. ESRD) is a vexing task, with concerns of imperfect outcome estimation and dilemmas for whether surgical intervention for permanent vascular access is warranted. O'Hare and colleagues indicated that in the event of AVF referral of all elders with estimated glomerular filtration rate (eGFR) <20 mL/min/1.73 m 2 , only 22% of all created fistulas would need to be used for HD (9). In a recent study comprising 3418 patients aged ≥70 years with advanced CKD who underwent placement of AVF or AVG before dialysis, 15% died before dialysis, 18% survived dialysis free, and 67% started dialysis by the end of the 2-year follow-up. Increasing age was associated with decreased likelihood of initiating dialysis; patients aged ≥85 years were less likely to start dialysis, death being a competing event compared with the reference group age 70-74 years old (adjusted HR 0.83; p = 0.01) (12). Compounding this issue is that of those who undergo permanent access placement pre-dialysis, the chance of having a functional AVF at dialysis initiation is quite low. An important finding in the study by Lee and colleagues was that older patients who received an AVG pre-dialysis had lower likelihood of needing a TCVC at dialysis initiation compared with those who received an AVF (28% vs. 46%, respectively, p<0.001), which renders AVG access in this population a useful “catheter-sparing” strategy (12). Although the majority of patients with pre-dialysis vascular access placement had early nephrology evaluation (of more than one year prior to dialysis initiation), a substantial proportion underwent AVF surgery too late to optimize the likelihood of initiating dialysis with mature AVF – an observation that speaks for the difficulty in estimating dialysis needs and timing for vascular access referral in elderly patients (12).
The intricate relationship between the type of pre-dialysis access, age, comorbidity and dialysis survival adds to the complexity of choosing between AVF and other forms of vascular access as the first pre-dialysis access in the elderly with CKD. DeSilva and colleagues evaluated dialysis survival as a function of the first vascular access created pre-dialysis – which was not necessarily the access used at dialysis initiation – in different age groups (67-79, 80-89, and ≥90 years), further stratified for the comorbidities of malignancy, peripheral vascular disease and diabetes (13). Their study showed a dialysis survival advantage for pre-dialysis AVF placement compared to AVG in patients aged 67-79 who had no history of malignancy, peripheral vascular disease or diabetes (HR, 1.10; 95% confidence interval [CI], 1.02 to 1.17; p = 0.007); and in those aged 80-89 years with history of malignancy (HR, 1.31; 95% CI, 1.02 to 1.67; p = 0.03). Conversely, there was no difference in dialysis survival between pre-dialysis placement of AVF and AVG in patients aged 80 years and older without history of malignancy (HR, 0.94; 95% CI, 0.85 to 1.03; p = 0.19), independent of peripheral vascular disease (HR, 0.98; 95% CI, 0.88 to 1.09; p = 0.69) or diabetes history (HR, 0.98; 95% CI, 0.86 to 1.11; p = 0.72); and in patients aged 67-79 years with history of malignancy (HR, 1.12; 95% CI, 0.91 to 1.38; p = 0.27), peripheral vascular disease (HR, 1.12; 95% CI, 0.97 to 1.29; p = 0.12) and non-diabetics (HR, 1.09; 95% CI, 0.97 to 1.23; p = 0.14). Notably, the rate of TCVC use at dialysis initiation was higher among patients who had an AVF placed as their first pre-dialysis vascular access (43.2%) than among those with pre-dialysis AVG (25.4%). However, patients who had a TCVC as their first pre-dialysis vascular access had inferior survival compared with those who underwent pre-dialysis AVF placement, independent of the age group and comorbidities (HR, 1.77; 95% CI, 1.73 to 1.81; p<0.001) (13).
Studies describing the technical success for AVF surgical intervention in the elderly delivered incongruent results. Age per se, in many studies evaluated as 65 years and older, was associated with much higher rates of primary and secondary AVF failure (14). In a cohort of 168 patients with CKD who underwent AVF surgery and compared elderly patients to younger ones, the 12-month primary assisted patency was 35% and 67%, respectively (p = 0.002); and secondary patency was 36% and 67%, respectively (p = 0.004) (15). A meta-analysis of 13 studies concluded that older patients have 80% higher risk of secondary AVF failure (16). In a separate study, elderly were 2.5 times more likely to experience primary functional patency loss (17). Nevertheless, similar fistula patency rates between older and younger individuals have been reported (18, 19). Bias by selection for surgical intervention or surgical referral could explain the discrepant results. It has been well appreciated that significant variability exists in the level of pre-operative surgical assessment and eligibility criteria used for fistula creation (20). In a retrospective study by Olsha and colleagues, patients who were aged ≥80 years underwent fistula intervention only if the vein size was ≥3 mm in diameter on pre-operative vein mapping; otherwise, an AVG was placed (19). In a questionnaire study, octogenarian age and comorbidities combined dissuaded more than 40% of the nephrologists from referring for fistula surgery (21). Therefore, differences in medical and surgical practice could create selection of ‘healthier’ older patients (who inherently have higher chances of AVF maturation) in some centers and account for dissimilar results between studies. Anatomical location of AVF can impact the rate of fistula success. Within the group of older patients specifically, distal AVF location (radio-cephalic) has a lower success rate than brachiocephalic fistulas (16, 22). Recently, Hod and colleagues evaluated the optimal time window for pre-dialysis AVF placement in the older population (aged 67 years and older) that would balance a better rate of fistula success (defined as using the AVF for the first HD session) for a lower rate of interventional access procedures (23). Based on their study, preemptive placement of AVF 6 to 9 months before dialysis initiation yields higher success rate for having a functional AVF at dialysis initiation than when AVF is created 1 to 3 months pre-dialysis. Even though similar fistula success rate was noted in those who had the AVF placed more than 9 months before dialysis initiation, these patients underwent more interventional procedures in order to salvage the fistula. The rate of access interventions steadily increased over time starting at 3 months, with a mean of 0.64 procedures per patient for AVF created 6 to 9 months compared with 0.72 procedures per patient for AVF created more than 12 months pre-dialysis (p<0.001). Acknowledged by the authors was that the total number of vascular access interventions might have been even greater had they not excluded the patients with placement of a second AVF after failure of the initial fistula (23).
When an elderly patient with CKD is encountered, several important long-term planning decisions need to be pondered, the most important being consideration of whether (or not) the patient would have meaningful gain from renal replacement therapy. In some, the decision to offer renal replacement or not could be straight forward. In many others, based on associated comorbidities, this decision may have to be deferred to a later time point until CKD progression. Thus, it is important to consider if the patient is a candidate for: (a) renal replacement, (b) expectant management, or (c) conservative/palliative management. If the patient is a candidate for renal replacement and the modality chosen is HD, a decision needs to be made regarding the type of access. If the patient is a candidate for an AVF, an attempt need be made to place an AVF, ideally a few months prior to initiation of dialysis. Some patients may not have anatomy suitable for AVF but may be candidates for AVG; in these scenarios, AVG is better placed closer to the date of initiation of dialysis.
Treatment decisions ought to be guided by the goals of care and prognosis estimation; providers, patients and health-care proxies should share in the decision making (Tab. I). Potential complications with hemodialysis such as hypotension, arrhythmias, cognitive and functional decline; as well as advantages and disadvantages associated with each form of vascular access need to be outlined during patient and family education regarding renal replacement modalities. Surgical placement of AVF or AVG stands as the optimal approach for all elderly who have a higher likelihood of needing dialysis, are good candidates for dialysis and opted for HD, and have otherwise a good prognosis. Expectant management has not been much delineated in the literature although, in our opinion, it is relatively commonly employed in clinical practice. Treatment planning in some elders might fall into “middle of the road” approach when there is uncertainty over needing dialysis or how the patient will tolerate dialysis. One could argue that if there is uncertainty about whether an older patient will tolerate dialysis, there is even greater uncertainty whether he or she would benefit from this treatment. However, predicting dialysis tolerance is not always straightforward, and a time-limited trial of dialysis is sometimes elected by the physician and/or patient (24). Not infrequently, elderly display much anxiety about preemptive dialysis preparation and prefer to accept the risk of using a TCVC given uncertainty about the need for dialysis or the outcome of permanent vascular access intervention. There are instances when although the physician considers that dialysis would prolong sufferance at limited gain for some frail elderly with multi-morbidity, the patient and/or family members want to pursue dialysis contrary to the physician's advice (25). In our opinion, in these latter circumstances expectant management with TCVC placement at dialysis initiation (should dialysis become necessary) is a rational approach. Ulterior assessment for an alternative vascular access (AVF or AVG) based on clinical course must be outlined in the initial plan of care.
Steps to decision making for hemodialysis vascular access in elderly patients
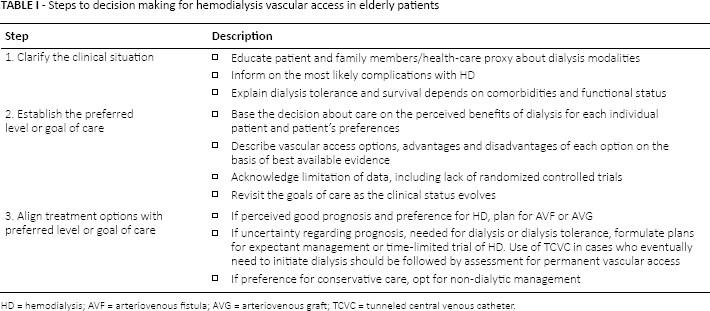
HD = hemodialysis; AVF = arteriovenous fistula; AVG = arteriovenous graft; TCVC = tunneled central venous catheter.
Until we will have better prognostic means to target those who are most likely to start dialysis and experience successful AVF development, both the morbidity burden and the functional status of each individual patient ought to be the tools we use for prognostication, clinical decision making, and vascular access planning (26). A large number of elderly patients with pre-dialysis CKD have significant functional impairment: 95% have at least one instrumental activities of daily living dependency with a median of five dependent daily activities; 75% are unable to rise from a chair without the use of their arms or an aid; and 68% are unable to attempt a tandem stance (27, 28). Importantly, functional status outperforms comorbidity burden as a predictor of mortality. Alfaadhel and colleagues prospectively evaluated a cohort of 360 incident dialysis patients and showed that for each point increase in clinical frailty scale the HR for death was 1.22 (95% CI, 1.04 to 1.43; p = 0.02) adjusted for age and comorbidity (29). Therefore, an holistic approach that takes into consideration the functional status, can position decision making in the context of frailty to better inform those who experience decisional conflict or ambivalence towards dialysis.
Elderly with Incident ESRD
Catheters are the most common form of vascular access used at dialysis initiation in all patients, including the elderly. Factors that lead to use of TCVC in incident patients include, but are not limited to, late placement of AVF pre-dialysis, primary AVF failure, urgent dialysis initiation following AKI, unexpected decline in kidney function, patient choice, or lack of pre-dialysis nephrology care. Barring patients who have a developing fistula or graft at dialysis initiation, referral for permanent AV access placement is essential in those who exhibit good prognosis. In the remainder of patients, vascular access selection is to be finalized by the treating team based on prognosis and goals of care (30, 31).
To ascertain each individual's clinical prognosis, the comorbidity burden, the severity of comorbid conditions, and the cognitive and functional status are critical pieces of information. Older patients on HD with a Charlson comorbidity index (CCI) score ≥8 have a 50%-60% mortality rate within the first 12 months of dialysis, independent of the functional performance (6, 32). Other comorbidity indexes also showed a direct correlation between the baseline disease burden and survival on dialysis (33, 34). Physical and functional disability not only is very prevalent among elderly with pre-dialysis CKD but also worsens significantly after the start of dialysis, with most of the physical decline taking place within the first 3 months of dialysis start (27, 28). Incremental changes in the level of frailty after dialysis initiation was shown to strongly associate with death in this population (35). Sedentary elderly (those who never or almost never exercised) have 62% higher risk of death within the first year of dialysis initiation compared with non-sedentary individuals (36).
Research has evidenced that the survival benefits associated with the type of HD access used at dialysis initiation are age- and comorbidity-dependent. Overall, having a functional AVF at dialysis initiation is superior to using AVG or TCVC in all the patients, including elderly patients, with a few possible exceptions among patients aged ≥90 years (8, 37). The differences in dialysis survival between AVF and AVG and between AVG and TCVC as the first vascular access used at HD initiation in specific elderly groups appear to be more complex. In the study by Hicks and colleagues, using AVG compared to TCVC at HD initiation rendered survival benefit for all patients aged 75-89 years, but not for those older than 89 years (8). DeSilva and colleagues analyzed dialysis survival in older incident HD patients as a function of the first vascular access used for HD. In their cohort, there was no difference in survival between AVG and TCVC in those aged 70 to 80 years with history of malignancy; 81 to 90 years and history of malignancy or peripheral vascular disease; and in all patients aged >90 years irrespective of malignancy, peripheral vascular disease, or diabetes history (37). In the US Renal Data System (USRDS) Wave II prospectively collected dataset comprised 764 incident patients aged ≥65 years who initiated HD with either AVF or AVG, there was no difference between fistulas and grafts in rates of intervention (odds ratio [OR], 1.49; 95% CI, 0.76 to 2.9; p = 0.24 in diabetics; OR, 1.48; 95% CI, 0.95 to 2.3; p = 0.08 in nondiabetics) or mortality (OR, 1.34; 95% CI, 0.92 to 1.95; p = 0.123 in diabetics; OR, 1.05; 95% CI, 0.81 to 1.36; p = 0.735 in nondiabetics) (38). These results challenge the notion of fistula before graft approach in elderly and would support a strategy of a more liberal use of grafts in this patient population.
Elderly with Prevalent ESRD
It is not uncommon for elderly patients on HD who had a functional AVF or AVG to experience subsequent AV access failure and require placement of TCVC. Whether we should treat these patients with a secondary fistula, a prosthetic graft, or catheter alone is another predicament that physicians frequently encounter. To our knowledge, clinical studies that evaluate patient and access survival based on the type of subsequent vascular access in elderly who underwent creation of more than one AV access are lacking. A retrospective study to analyze this issue would be seriously confounding, and compromise the accuracy of drawing sound conclusions. While we endorse pursuing a new fistula or graft attempt in younger patients, re-engaging the elderly patients in this pursuit warrants more examination. Whereas fistula or graft intervention was a strategy of choice in an elderly patient before or soon after dialysis initiation, this might not remain the case year(s) after dialysis. As the clinical course unfolds – often with unanticipated alterations in functional, cognitive or clinical status – patient's goals and preferences may also change and the vascular access level of intervention needs to realign with the overall goals of care.
The main reason for converting the vascular access from TCVC to AVF or AVG access is to avoid catheter-related bloodstream infection (CRBSI). Catheter-related infections are considered a main reason for higher all-cause mortality, cardiovascular mortality, and sudden death in patients who receive HD via TCVC. Two points deserve more discussion in this context. First, patients who received an AVF or AVG that successfully developed to be used for HD likely differ (medically, functionally, socially etc.) in ways that cannot be fully captured in retrospective survival analysis studies. In a retrospective study by Woo and colleagues encompassing 16,464 dialysis-dependent patients aged 66 years and older who underwent either first AVF (75.2%) or first AVG (24.7%) surgery, those in the index graft group had significantly higher mean total covered billed charges in the 12 months before the index surgical date, higher incidence of living in a zip code associated with overall lower socio-demographics, and a higher incidence of diabetes, heart failure, stroke, ischemic heart disease, and chronic obstructive pulmonary disease (39). In the first 12 months after the index surgery, the mortality in the fistula group was 28.2% versus 29.9% in the graft group (p = 0.03). The incidence of repeat AVF/AVG creation and TCVC placement was substantially higher in the first 12 months after fistula creation (44.4% of patients) compared with grafts (33.7% of patients, p<0.001). At longer follow-up, one-year repeat fistula/graft/catheter-free survival was lower in the index fistula group (39.7%) than the index graft group (46.0%, p<0.001) (39). Nevertheless, as indicated above, the study showed that the group with AVF attempt had a modest 1.7% adjusted survival advantage at 12 months. Second, the elderly might be at lower risk of developing CRBSI compared to non-elderly patients, based on a single-center retrospective study and two separate reports from USRDS (40-42). In these studies, however, access-related infections were more common in those with TCVC compared to those with AVF or AVG (41, 42). Therefore, based on these data, in the oldest HD patients who experience AVF access failure, placement of an AVG while reserving TCVC for patients who are perceived to have a remaining life expectancy of less than one year is a sensible approach.
Patient's preference for a certain vascular access and impact on quality of life should not be ignored. Quinn and colleagues showed that patient-reported views towards vascular access differ significantly between age groups. Younger patients are more likely to be bothered by TCVC for having to shield the catheter (vascular access symptom score 35 vs. 11% for non-elderly vs. elderly; p = 0.05), and interference of the catheter with social activities (22 vs. 6%; p = 0.02). In contrast, older patients are more likely to be bothered by AVF due to bleeding (vascular access symptom score 20 vs. 6% for non-elderly vs. elderly; p = 0.02) and bruising (24 vs. 4%; p<0.01), and less likely to be bothered by catheters (43).
Conservative Management
The option of conservative (non-dialytic) management supported by palliative care is a judicious alternative under certain circumstances. Several studies showed that for octogenarians with multiple co-morbidities and poor performance status, dialysis might not significantly prolong survival compared to conservative care (44-46). Moreover, up to 30% of the octogenarians on dialysis choose to withdraw dialysis, this being the most common cause of death for elderly patients in France and Australia (47, 48). For elderly with multiple comorbidities, severe dementia, and metastatic or incurable cancer, close interaction between patient, family members and nephrology, geriatrics and palliative team is essential (49). Along this concept, there is a growing recognition that palliative care training needs to be incorporated into the nephrology fellowship curriculum (50). The REnal specific Advanced Communication Training (REACT) program developed in UK to improve Advance Care Planning for renal patients showed an increase in confidence in communicating end-of-life issues between renal professionals and patients (51).
Conclusions
In clinical practice, planning for dialysis and vascular access in the elderly with advanced kidney disease extends beyond ‘fistula first’ approach. Selection of elderly who would benefit from a permanent vascular access and selection of the type of pre-dialysis permanent access ought to be tailored to each individual patient. Achieving a functional AVF is the sublime goal; the key is to recognize when a functional fistula is a tenable goal. Grafts are a reasonable alternative to be considered in situations when AVF is not a fit option. Emerging data show that in some elderly patients, grafts might confer similar survival benefit, higher surgical success rate, and might be more likely to reduce catheter dependence compared to fistulas. Conservative medical management may be employed in those with very high comorbidity and frailty scores. The approach could be different not only from one patient to another, but also from one clinical stage to another within the same individual. The relative benefits and harms of each form of vascular access vary based on patient's characteristics, prognosis, preference, and goals of care – all of which may longitudinally change.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: Neither of the authors has financial interest related to this study to disclose.