
Abstract
Background
Central vein thrombosis or obstruction is a common complication associated with central venous catheters placed for intermittent hemodialysis. The reported outcomes of percutaneous catheter-based interventions reveal high rates of lesion recurrence with varying and frequently limited patency intervals. We present the case of open venous bypass in the treatment of catheter-associated chronic central vein occlusion.
Methods
We report a case of symptomatic arm swelling secondary to central vein stenosis and failed endovascular venous intervention treated by central vein bypass with prosthetic graft through median sternotomy.
Results
Patient had an open axillary to innominate venous bypass via median sternotomy incision, which resulted in resolution of patient's symptoms and uninterrupted patency of the pre-existing vascular access.
Conclusions
Open venous bypass is a reliable alternative to endovascular intervention in the symptomatic patient with extensive central vein occlusion as a primary intervention or in whom prior endovascular therapy has failed.
Case report
Our patient is a 36-year-old African-American female with medical history of diabetes mellitus (DM), hypertension and end-stage renal disease (ESRD). She had multiple types of hemodialysis access in the past, including central venous catheters as well as arteriovenous (AV) fistulas on both upper extremities using native veins and prosthetic grafts. Subsequently, she developed massive left upper extremity swelling secondary to placement of left brachial artery to axillary vein graft with complete central outflow occlusion (Fig. 1). She was referred to our clinic for surgical evaluation for possible surgical reconstruction of central venous system.
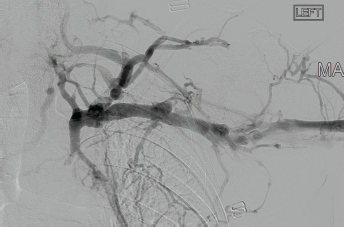
Preoperative fistulogram. Imaging study showing occlusion central veins causing AV fistula malfunction.
Preoperative angiography demonstrated left subclavian vein occlusion with diffuse collateralization and proximal reconstitution at the level of left innominate vein. All surgical and endovascular interventions were discussed with the patient including additional endovascular interventional options. A decision was made to proceed with open venous bypass via median sternotomy and possible infraclavicular incision. All procedural risks and benefits were explained to the patient and informed consent was obtained.
The patient was taken to the operating room, where a median sternotomy was performed (Fig. 2). There were multiple arterialized venous chest wall collaterals with considerable time spent in order to control them. The confluence of left innominate vein with the superior vena cava (SVC) was dissected and innominate vein was patent, which corroborated with angiogram findings. A large thymus gland was noted and the left lobe was resected along with isthmus to open the space for the bypass graft and give better access to the innominate vein. The innominate vein was very scarred and calcified. It was transected at the patent segment, adjacent to cavo-atrial junction. Then, internal mammary artery retractor was placed to elevate the left chest wall and innominate vein was dissected off the aortic arch to the level of left subclavian vein, which was very tedious due to extensive adhesions. At this point, patient was systemically heparinized and vascular clamp was placed on intrathoracic portion of the subclavian vein and it was transected. A left infraclavicular incision was then made to access the left subclavian vein distally. Subclavian vein was tightly adherent to the subclavian artery from multiple previous interventions and very careful dissection was employed to free the subclavian vein without injuring any collaterals. Vein was found to be patent at the junction of proximal and middle portions where it measured 8 mm in diameter. An 8 mm Propaten Gore-Tex graft (Gore Medical, Newark, DE) was brought to the field and an end-to-end anastomosis completed. The tunnel was created by resecting 2-inch portion of the medial side of the left clavicle. The graft was then routed in a curvilinear fashion through this area and under the sternal manubrium and brought to the confluence of left innominate vein and SVC where an end-to-side anastomosis was performed. Protamine was given and adequate hemostasis was achieved. Closed suction drains were placed in the left infraclavicular wound and mediastinum and right tube thoracostomy.
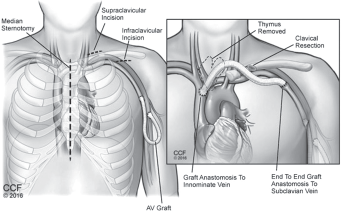
Illustration of the procedure. Artist drawing of the procedure performed, showing the approach and the anatomy.
Postoperative angiography demonstrated excellent flow in the graft (Fig. 3). Patient did very well in immediate and late postoperative periods. There was gradual resolution of left upper extremity edema in the postoperative period.
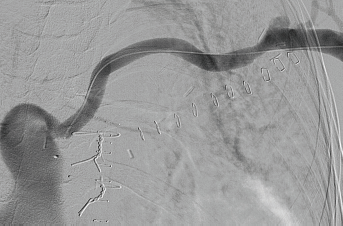
Postoperative angiogram. Imaging study showing patent prosthetic bypass graft.
Discussion
In the hemodialysis patient population, thrombosis and/or complete obstruction of the subclavian vein occurs in 35% (15%-50%) and 3% within the internal jugular vein (1). Clinically, central vein stenosis frequently leads to a painful arm swelling when an IV fistula is present on the same side (2). When such symptoms develop and persist, the current practice is for endovascular intervention with venous angioplasty in an attempt to salvage the vascular access and improve the often disabling arm swelling. Unfortunately, endovascular interventions on the central venous system lack durability and when restenosis or occlusion inevitably develops, few options exist save ligation and abandonment of the ipsilateral vascular access.
In the USA, up to 80% of incident patients initiate hemodialysis via central venous catheters (CVCs). Thus, chronic central venous stenosis is a frequent cause for AV vascular access (VA) failure, the presence of which may eliminate all VA options for the ipsilateral extremity. Clinical symptoms of limb edema are more likely to occur in the presence of high hydrostatic pressure that results from VA (1, 2). The resultant upper extremity, head, face and neck swelling and pain may dramatically affect the quality of life and the ability to cannulate the functioning VA. These symptoms are usually non-responsive to non-operative treatment with arm elevation and arm wrapping. Ligation of the VA is the most aggressive treatment. However, this has the obvious consequence of leaving the patient without permanent access and necessitating placement of a CVC on the contralateral extremity as the means for hemodialysis. This option may be a more appropriate measure for a VA which is poorly functioning and requiring multiple maintenance interventions or in a medically compromised patient in whom life expectancy is limited.
In most centers, symptomatic central venous stenosis/occlusions are largely managed with endovascular therapies. Various recanalization techniques have been described for occlusions. Definitive management of the lesion after it has been crossed is controversial and no consensus exists. In short, venous angioplasty with provisional stenting may be used. Unfortunately, venous angioplasty patency is reported to be 30%-60% at 6 months with the treatment of recanalized occluded vessels on the low end of this expected patency. The best choice stent in this setting is unclear as well. Options include bare self-expanding, covered self-expanding when branch vessels do not require preservation, and balloon expandable covered devices. Each possess benefits depending upon the specifics of the treated pathology. Inevitably however, any central venous intervention is likely to fail given the patency limitations in the hostile environment of vascular access. It was confirmed by Lumsden et al (3) who showed that balloon angioplasty provides short-term patency and the role for endovascular stent placement remains to be defined, but early results are not optimistic. Prevention of central venous stenosis by avoiding subclavian catheterization is optimal (3).
The management of central venous obstruction can be divided into endovascular and open repair types. There are many papers comparing these types of repair. According to Wisselink et al (4), symptomatic relief at 1 year was achieved in 88% in the surgical group versus 36% in the angioplasty group, and at 2 years in 71% versus 0%, respectively, suggesting higher long-term success rate of operative reconstruction. Two other studies showed early restenosis and eventual need for multiple repeat percutaneous interventions with percutaneous angioplasty only, which improved with addition of stenting (5, 6).
Open surgical repair involves graft bypass with or without thrombectomy and relies on reconstruction of the venous outflow tract. Several surgical techniques were described, ranging from venous diversion and bypass with prosthetic grafting to right atrial bypass grafting (6, 7). Various biologic and prosthetic graft options exist including PTFE, Dacron, Homograft and Bovine carotid (artegraft). Gradman et al (5) suggested venous repair and patching rather than a bypass due to high infection rates and repeated thrombosis (5). Axillary vein to internal jugular vein bypass was also described as an efficient procedure to resolve severe upper extremity swelling while salvaging the dialysis access (7). Axillary-femoral venous bypass with long prosthetic graft was utilized by a group of authors in patients with central venous thrombosis. Venous bypass of the obstructed vein to right atrial appendage using large caliber prosthetic graft was performed in extreme cases after previously failed endovascular interventions and thrombosed vein-to-vein bypass grafts (8). Possibly the most minimally invasive approach avoiding median sternotomy was described by Glass et al (9). The study included performing subclavian vein to atrial appendage bypass through retrosternal tunnel created by performing claviculectomy and third intercostal space “mini-pericardiotomy”.
There is also a combined procedure, described by Illig et al (10), which included venous stenting combined with bony decompression by means of first rib resection.
All of the procedures mentioned above can be utilized in case of symptomatic central venous obstruction in patients with AV dialysis access on the ipsilateral extremity.
Conclusion
Open surgical reconstruction of central veins remains an excellent option in symptomatic central venous stenosis in dialysis patients and should remain a viable option in patients who are not candidates for endovascular treatment.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.