
Abstract
Background
While the use of technologies such as ultrasound and electrocardiographic (ECG) guidance systems to place peripherally inserted central catheters (PICCs) has grown, little is known about the clinicians who use these tools or their work settings.
Methods
Using data from a national survey of vascular access specialists, we identified technology users as PICC inserters that: (a) use ultrasound to find a suitable vein for catheter placement; (b) measure catheter-to-vein ratio; and (c) use ECG for PICC placement. Individual and organizational-level characteristics between technology users versus non-users were assessed. Bivariable comparisons were made using Chi-squared or Fisher's exact tests; two-sided alpha with p<0.05 was considered statistically significant.
Results
Of the 2762 PICC inserters who accessed the survey, 1518 (55%) provided information regarding technology use. Technology users reported greater experience than non-technology users, with a higher percentage stating they had placed >1000 PICCs (55% vs. 45%, p<0.001). A significantly greater percentage of technology users also reported being certified in vascular access by an external agency than non-technology users (75% vs. 63%, p<0.001). Technology users were more often part of vascular access teams with ≥10 members compared to non-technology users (35% vs. 22%, p<0.001). Some practices also varied between the two groups: for example, use of certain securement devices and dressings differed between technology users and non-users (p<0.001).
Conclusions
Technology use by vascular access clinicians while placing PICCs is associated with clinician characteristics, work setting and practice factors. Understanding whether such differences influence clinical care or patient outcomes appears necessary.
Keywords
Introduction
As with other healthcare sectors, the development of innovative technology to improve clinical care and patient outcomes has grown substantially in the field of vascular access (1–2–3). With the advent of technologies such as ultrasound to measure vein size and electrocardiography (ECG) to guide the catheter tip to the appropriate location, this type of advancement is most evident when it comes to insertion and use of peripherally inserted central catheters (PICCs) (4, 5).
Early data suggest that the promise of this technology is substantial. For instance, use of ultrasound to calibrate PICC size to vein diameter has been shown to reduce risk of thrombosis (6, 7). Similarly, evidence suggests that more appropriate guidance of catheter tips using ECG can improve patient outcomes by reducing occlusion and thrombosis (8, 9). There is little doubt that these technologies and practices, coupled with advances in catheter design and operator training, have significantly improved PICC outcomes (10, 11).
Despite growing availability, the extent to which vascular access specialists who place PICCs use these technologies is not known (12). Furthermore, whether the individual characteristics or work settings of technology users differ from non-technology users is also not known. This knowledge gap is important as differences in use of technology may affect patient safety. Therefore, we used data from a national survey of vascular access specialists to identify and compare characteristics of those who do versus those who do not use modern technology when placing PICCs. We hypothesized that users of technology would differ from non-technology users in important ways, including individual (e.g., number of PICCs placed, vascular access certification status) and work setting (e.g., academic medical center, number of vascular access nurses) characteristics.
Methods
Study setting and participants
Partnering with the Association for Vascular Access (AVA) and the Infusion Nursing Society (INS), we distributed a survey aimed at vascular access specialists who place PICCs. AVA, a multidisciplinary vascular access professional organization and INS, a professional nursing organization whose members participate in various aspects of infusion therapy including PICC insertion, both maintain membership directories that can be used for surveys deemed relevant to the specialty. Following review and approval of the survey instrument by both organizations, the study was announced to members by an email that included an electronic link to the survey. The survey was also publicized on each organization's website. Reminder emails were sent to encourage participation over a period of five weeks.
Development and validation of the survey
Development of the survey instrument (PICC1) began with a literature search to identify relevant evidence regarding vascular access practices, including use of contemporary technologies. The literature search was conducted using search strategies from published systematic and narrative reviews (13–14–15), as well as those used for the creation of the Michigan Appropriateness Guide for Intravenous Catheters (MAGIC) (16). Retrieved articles were scanned for titles and abstracts that examined use of technology for insertion of PICCs. Articles identified were then used to inform the development of questions about PICC use, including facility details, clinical practices, and availability and use of technology. The initial survey instrument was pre-tested by clinicians experienced in PICC placement and refined based on feedback. The revised instrument was then programmed into an online survey administration tool (SurveyMonkey®) and tested by members of the study team to ensure functionality. After final testing, the instrument was disseminated by AVA and INS as previously described. To encourage participation, a $US10 Amazon gift card was offered to those who completed the survey.
Identification of technology-users
To distinguish technology users from non-users, we evaluated responses to the following three questions: (i) “Do you routinely use portable ultrasound to find a suitable vein for PICC insertion?”; (ii) “Do you routinely use portable ultrasound to estimate the catheter-to-vein ratio prior to PICC insertion?”; and (iii) “Do you routinely use ECG-guidance assisted systems to place PICCs?” We chose these three questions because (a) the technologies represented have been associated with safer insertion practice and outcomes and (b) they are not yet routinely used in practice in the USA (16–17–18). Respondents who answered yes to all three questions were defined as technology users for this study. Conversely, respondents who used some, but not all of these technologies, or those who used none of these tools were considered non-technology users.
Statistical analysis
Descriptive statistics were used to characterize responses. Responses were not required to all questions; therefore, frequency estimates for each individual question were calculated using the total number of responses for the question as the denominator. In accordance with our hypothesis, we compared specific individual and work setting characteristics by technology user versus non-user status. Individual characteristics included certification status, leadership position and experience as determined by volume of PICCs placed. Work setting characteristics examined included type of work location, number of vascular access nurses, affiliation with medical or nursing schools and number of PICCs placed per month. In addition to individual and work setting characteristics, we also compared practices that involved use of specific tools (i.e., trimming devices) and advanced securement devices, which we believed might also be more frequently used by technology users. Bivariable comparisons were made using Chi-squared or Fisher's exact tests, as appropriate, for categorical data.
Two-sided alpha with a p value <0.05 was considered statistically significant. All statistical analyses were conducted using Stata 13 MP/SE (StataCorp, College Station, TX).
Ethical considerations
The study was reviewed and deemed exempt from regulation by the University of Michigan Institutional Review Board (HUM00088351).
Role of the Funding Agency/Sponsor
This project was funded through an Investigator Initiated Research Grant from the Blue Cross Blue Shield of Michigan Foundation (Grant Number 2140.II; PI. Chopra). This work was also supported by the Department of Veterans Affairs, Health Services Research and Development Service and National Center for Patient Safety. Both funding sources had no role in study design, data acquisition, analysis or reporting of the data.
Results
Of the 2762 respondents who accessed the survey and indicated that their current position included inserting PICCs, 1518 (55%) provided information regarding technology use and were included in this analysis (Fig. 1). A total of 804 reported using all three technologies, whereas 714 did not. However, among respondents who used technology, the use of individual tools was variable. For example, respondents most frequently reported use of portable ultrasound to find a suitable vein (96%), followed by estimation of catheter-to-vein ratio (83%). Use of ECG-guidance to place PICCs was least common (62%) among all respondents who used technology to place PICCs. Similarly, among non-technology users, 561 (79%) reported using two of the three technologies, 122 (17%) reported using one of the three, and only 31 (4%) reported using none of the three technologies.
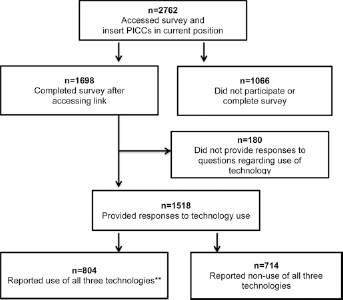
Study flow diagram.
Individual-level characteristics
As shown in Table I, technology users reported more experience than non-technology users, with a greater proportion stating they had placed >1000 PICCs (55% vs. 45%, p<0.001). A significantly higher percentage of technology users also reported being certified in vascular access (either vascular access-board certified (VA-BC) or being certified as registered nurse in infusion (CRNI) from AVA or INS, respectively) than non-technology users (75% vs. 63%, p<0.001). However, there was no significant difference between technology users and non-users with respect to serving as vascular access lead for their organization (54%, vs. 50%, p = 0.14).
Individual characteristics of technology users compared with non-users
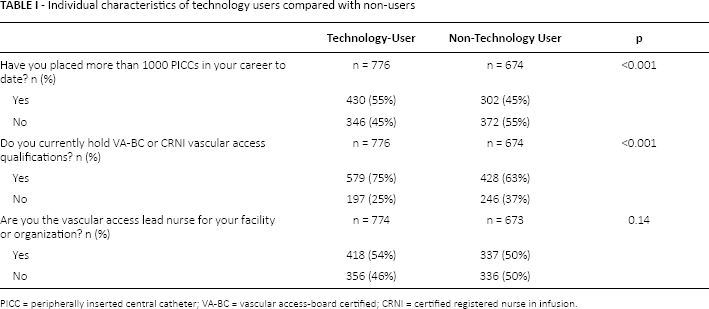
PICC = peripherally inserted central catheter; VA-BC = vascular access-board certified; CRNI = certified registered nurse in infusion.
Technology users often reported different job descriptions and professional vocations than non-technology users (Tab. II). Although the total number of respondents in each category was small, respiratory therapists (i.e., non-physician, licensed specialists who are trained to evaluate and deliver care for acute and chronic dysfunction of the cardiopulmonary system) most often reported use of all three technologies (81%, n = 39) followed by physician assistants (non-physician, licensed specialists who work under the supervision of a doctor to provide clinical care) or advanced practice nurse (69%, n = 44) and physicians (n = 13, 59%). Only half of the respondents who identified themselves as vascular access nurses reported using all three technologies (52%, n = 672).
Reported professional vocation/training (by technology use status)

Work setting characteristics
Important differences in work setting characteristics between technology users and non-users were noted. For example, work locations differed significantly (p<0.001), with a higher percentage of technology users reporting employment by for-profit community-based hospitals as compared to non-technology users (21% vs. 16%). We noted that the setting of respondent practice also influenced technology use. For example, respondents who reported placing PICCs solely in outpatient settings such as skilled nursing facilities, less frequently reported technology use compared to respondents who stated they only placed PICCs in hospital settings (36% vs. 55%, p = 0.02) (Tab. III).
Location of PICC placement (by technology use status)

PICC = peripherally inserted central catheter.
Technology users more often reported being part of vascular access nursing teams that included 10 or more members compared to non-technology users (36% vs. 23%, p<0.001). Technology-users also reported placing more PICCs per month at their facilities than non-technology users (p = 0.01). Although more technology users reported that their facility was affiliated with a nursing school than non-technology users (62% vs. 55%, p = 0.01), no differences in characteristics such as total bed size, or affiliation with a medical school were observed. Differences in the perceived level of overall support from hospital leadership between technology users and non-users were noted (p = 0.003) (Tab. IV).
Work setting characteristics of technology users compared with non-users
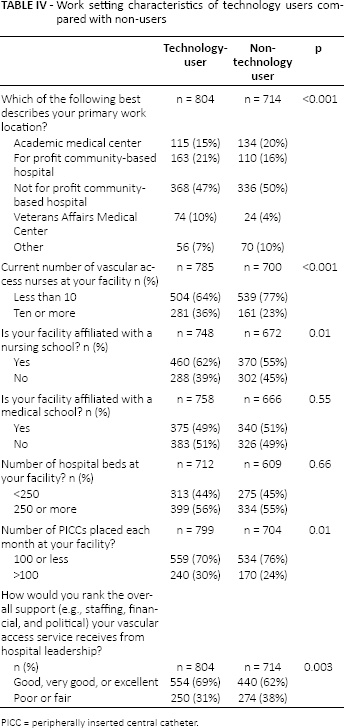
PICC = peripherally inserted central catheter.
Variation in practices between technology users and non-users
With respect to PICC insertion practice, technology users more often reported receiving assistance from other vascular access specialists when inserting PICCs (52% vs. 44%, p = 0.001). Technology users also more often stated that they routinely trimmed PICCs to length following insertion (94% vs. 91%, p = 0.04), and differences in the trimming tool used for this purpose between the groups were noted (p = 0.002). Use of securement devices differed between technology users and non-users (p<0.001), with technology users more frequently using advanced securement devices to prevent PICC dislodgement than non-technology users (8% vs. 3%) (Tab. V).
Use of certain practices by technology users versus non-users
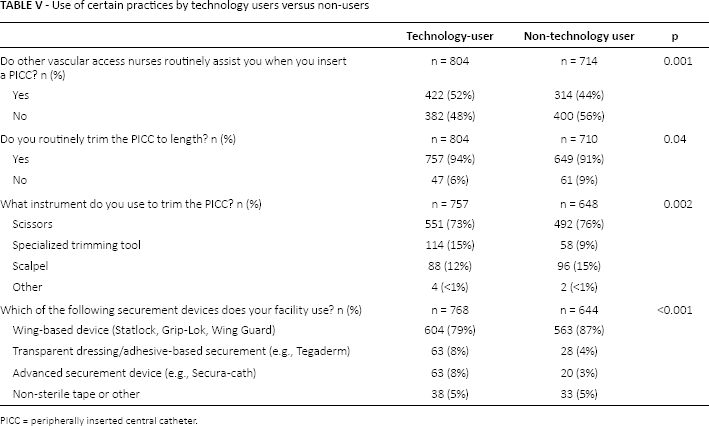
PICC = peripherally inserted central catheter.
Discussion
This analysis of the PICC1 survey of vascular access specialists suggests that certain individual and organizational factors distinguish those that use technology for PICC insertion from those that do not. For instance, technology users appear more experienced and have greater rates of certification in vascular access than non-technology users. Similarly, differences in work location, team size, and perceived support from hospital leadership were noted between these two groups. Notably, factors such as hospital bed size were not necessarily associated with technology use, suggesting that it is more than just a single facility characteristic that influences the adoption of technology. Even though one or two contemporary technologies were used by almost all respondents, our findings suggest that technology users who use all three of these tools are a unique subgroup of vascular access specialists. Studies to further understand the reasons behind differences in technology adoption and whether such aspects influence patient outcomes may be important.
Since the introduction of the original hand-crank introducer unit to advance PICCs from peripheral extremity veins to the cavoatrial junction in the 1970s (19), technology has been a defining feature of these devices. Over the past two decades, innovations such as ultrasound to measure veins and gauge appropriate catheter size, as well as ECG guidance to optimally position PICC tips, have led to even safer PICC insertion and potentially reduced the risk of various PICC-related complications. Despite the emergence of studies that have examined the efficacy of these technologies, few have examined users of these tools. Understanding individual and work setting characteristics of technology adopters is vital for optimizing access, effective use and a workforce trained to harness the promise of this technology. Our study thus helps shed new light on this important issue.
Some of our findings are intuitive. For instance, one might expect technology adopters to be more likely to hold external certification and have greater experience. Similarly, technology users would be expected to use more “advanced” aspects such as securement devices or specific trimming tools than non-technology users. However, some findings run counter to expectations. For example, we observed that technology users more frequently report receiving assistance from a vascular access nurse during PICC placement. This, at first, appears odd given that technology is designed to facilitate the insertion process. However, it is possible that technology users are more likely to recognize their limits and call for help during insertion. Alternatively, this finding may indicate that technology is not a panacea or a means to reduce workforce; rather, for effective use, assistance from others is required. Since the survey-based nature of our study does not allow further exploration of these issues, additional studies that examine this question more closely are clearly needed.
Our study has limitations. First, we used data from the PICC1 survey that targeted vascular access specialists belonging to two large professional organizations; thus, selection bias and non-response to the survey could affect our study findings. Second, we defined technology users as those who followed three specific practices; findings may differ if other criteria are used to define such users. However, because these three factors represent state-of-the-art practice as defined in current literature, we believe our approach captures the users who were the focus of this study. Third, why some specialists adopt technology while others do not cannot be determined from this study. For example, it is possible that technology users adopt practices simply as a result of facility requirements or contracts. However, available literature suggests a myriad of factors influence technology adopters and non-adopters in various health-related settings (20–21–22). As vascular specialists often advise hospital leadership on device and practice considerations, it is plausible that they are the driving force for technology adoption.
Despite these limitations, this study has important strengths. First, to our knowledge, this is the most comprehensive study to evaluate use of technology in vascular access related to PICCs. The individual and work setting variations observed in technology adoption is interesting and worthy of further exploration. Future studies that begin to focus on the costs and benefits of technology use on patient outcomes would be welcomed. Using randomized or quasi-experimental designs, such studies might also focus on the effect of technology adoption on process measures (e.g., time for PICC insertion), provider and patient satisfaction, and complications (e.g., thrombosis and infection). Second, our study suggests that technology users differ from non-users in important ways, some of which may influence patient care and safety. Given this finding, future work dedicated to understanding motivations behind adopting technology and its impact on practice would be welcomed. In particular, studies that examine the relationship between unit and organizational safety culture, workflow and protocols with respect to technology adoption would be welcomed. These data, in turn, could better inform the value and impact of a vascular access specialist team concept (23).
In conclusion, important differences between those that use three state-of-the-art technologies when inserting PICCs versus those that do not, exist. Future studies to understand drivers of technology use and association between these factors and patient outcomes now appear necessary.
Footnotes
Financial support: This project was funded by an Investigator Initiated Research Grant from the Blue Cross Blue Shield of Michigan Foundation (Grant Number 2140.II, PI: Chopra). The funding source played no role in study design, data acquisition, analysis or decision to report these data. Dr. Chopra is supported by a career development award from the Agency for Healthcare Research and Quality. This work was also supported by the Department of Veterans Affairs, Health Services Research and Development Service and National Center for Patient Safety. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the US government. Dr. Krein is supported by a VA Health Services Research and Development Research Career Scientist Award (RCS 11-222).
Conflicts of interest: Peter J. Carr has received “speakers’ bureau” payment from CareFusion in 2013 and Becton Dickinson in 2014 for lectures on vascular access. He received a grant from CareFusion to attend a scientific meeting and a part-funded Scholarship from Becton Dickinson to support research activities. All other authors declare no conflicts of interest.