
Abstract
Introduction
Children requiring long-term hemodialysis often face significant challenges due to their young age and small-vessel caliber for arteriovenous (AV) access creation. In this study, we report our experience of staged basilic vein transposition (BVT) in pediatric patients.
Methods
All patients undergoing staged BVT at a tertiary care pediatric hospital from 2003 to 2015 were reviewed. Indications for staged BVT included inadequate cephalic conduit or failed AV fistula using cephalic vein. Pertinent clinical variables were analyzed to determine treatment outcomes.
Results
Forty-two children (24 males, 57%) underwent 46 staged BVT during the study period. Median age was 12.8 ± 4.8 years (range 3-18). The mean weight was 47 ± 5.1 kg (range, 13-126 kg), with four children (10%) weighing ≤20 kg. Mean operative times for initial brachiobasilic AV fistula and staged BVT were 39 ± 12 minutes and 66 ± 17 minutes, respectively. Mean follow-up period was 5.4 ± 1.8 years. Functional maturation was achieved in 93% of BVTs. Early fistula thrombosis within 30 days following BVT occurred in four patients (10%). Late BVT thrombosis occurred in 13 patients (31%). Primary patency rates at 2 years and 4 years were 78% and 72%, respectively. Secondary patency rates at 2 years and 4 years were 86% and 82%, respectively.
Conclusions
Staged BVT is a durable and reliable autologous hemodialysis access in children who do not have adequate cephalic venous conduit.
Introduction
The prevalence of end-stage renal disease (ESRD) in the pediatric population has steadily risen in recent decades. It is estimated that there are more than 5000 pediatric patients undergoing hemodialysis in the USA each year (1). Although pediatric patients requiring hemodialysis (HD) account for less than 1% of the total patient population requiring HD in the USA (2), the ideal choice of vascular access in these young patients remains both a controversial and challenging issue.
In the pediatric population, HD access creation is often complicated by several anatomical and physiological variables, including lack of available upper extremity veins, fragility of the venous conduit, and propensity for venous spasm and subsequent occlusion due to small vessel caliber (3). Available options of HD access in children include HD catheter, arteriovenous (AV) fistula, and AV graft. According to the Vascular Access Work Group, a native AV fistula is the HD access of choice over other options, particularly in the upper extremities (4). In patients who have adequate cephalic veins, a radiocephalic or brachiocephalic AV fistula should be attempted as the initial access of choice. In the pediatric population, however, the suitability of these venous conduits is often limited due to inadequate venous caliber. Several studies have recommended a transposed brachiobasilic AV fistula before placing a prosthetic graft in patients with limited superficial venous conduits (5–7).
By comparison, the basilic vein offers several advantages over the cephalic vein as a venous conduit for AV access creation. First, the basilic vein is generally unused for routine venipuncture or intravenous access due to its deep location near the brachial plexus in the upper arm. In contrast to the cephalic vein, the basilic vein is typically free from scarring or superficial thrombophlebitis, which can be caused by frequent venipuncture. Second, the basilic vein is the largest superficial vein in the upper extremities, which can be twice the diameter compared to the cephalic vein. Once a basilic vein transposition (BVT) is created, this large transposed basilic vein allows AV fistula maturation with relatively easy cannulation for HD. This ease of access cannulation due to the large venous caliber represents a significant benefit in children with small superficial veins.
Although many studies have demonstrated BVT in children is feasible, reports on long-term outcome in the pediatric population remains scarce (5, 7–9). In this study, we report our experience and treatment outcomes of BVT in children.
Patients and Methods
A retrospective review of all children on chronic HD who underwent BVT procedure by faculty physicians of an academic vascular surgical group at a tertiary pediatric hospital from January 2003 to June 2015, was undertaken. Institutional Review Board approval was obtained for the study. Patients aged 4 to 18 years who underwent BVT were included in the study, and all BVT procedures were performed in a two-staged fashion. A brachiocephalic or radiocephalic AV fistula creation is considered as the first access of choice whenever possible, and BVT is considered when native cephalic vein was inadequate or unavailable for fistula reconstruction. Indications for BVT included inadequate cephalic venous conduit or previously failed radiocephalic or brachiocephalic AV fistula. Data analyzed included demographic information, etiology of kidney disease, date of initial HD, and transplantation history. In patients who had bilateral BVT fistula creation, the fistula in each arm was analyzed separately.
All patients underwent preoperative venous duplex ultrasound to ensure upper arm basilic vein was patent and >2.5 mm in diameter. In all patients, a first-stage brachiobasilic vein AV fistula was performed, which was followed by a second-stage BVT six weeks later. The brachiobasilic AV fistula was performed by making a longitudinal incision just above the antecubital fossa followed by the exposure of the basilic vein and brachial artery. The basilic vein was transected distally and the distal vein was ligated. The proximal basilic vein was transposed to the adjacent brachial artery in an end-to-side fashion using 7-0 polypropylene suture creating a brachiobasilic anastomosis. Once the fistula reached maturity, a second-stage transposition of the basilic vein fistula was performed. This was done by making two longitudinal incisions in tandem along the medial portion of the upper arm to expose the entire segment of the basilic vein from the antecubital to axillary fossa. Care was taken to avoid injury to the medial cutaneous nerve of the forearm that surrounds the vein along its course. The basilic vein was then transected in the antecubital region, with all venous branches ligated. The basilic vein was transposed using a GORE semicircular tunneling device (WL Gore, Flagstaff, AZ) to a subcutaneous lateral plane. Care was taken to avoid axial rotation, especially near the axillary vein junction. An arteriotomy was made in the distal brachial artery, and the transposed basilic vein was connected to the brachial artery in an end-to-side fashion using 7-0 polypropylene suture to create a brachiobasilic anastomosis.
Postoperative follow-up was made at 2 weeks and 6 weeks for wound check and clearance for fistula access. Surveillance duplex ultrasound was performed at three months and six months following BVT and every 6 months thereafter. Endovascular intervention was performed when ultrasound detected diminished or outflow obstruction based on previously published criteria (10). Additional follow-up was made as needed for children with any fistula-related issues, such as pseudoaneurysm formation, BVT thrombosis, steal syndrome, or wound infection. Records from HD units were used to confirm patency in patients who no longer required postoperative follow-up. Primary outcome measures were 2-year and 4-year primary and secondary patency. Primary patency was defined as the time from AVF creation until any intervention performed to maintain patency or abandonment of the fistula for any reason without intervention. Secondary patency was defined as the patency of the AVF from creation to abandonment for any reason, including the interval before and after any interventions to re-establish patency in malfunctioned AV access.
Statistical comparison of the patency rates between children of varying weight groups was performed using Pearson's Chi-square test. All statistical analysis was performed using a statistical software program (SAS Institute, Cary, NC). All values were expressed as mean ± SEM. Statistical significance was accepted with a p value of less than 0.05.
Results
During the study period, 46 BVTs were performed in 42 children. The mean age of the children was 12.8 ± 4.8 years (range 3-18). Twenty-four patients (57%) were male. The mean weight was 47 ± 5.1 kg (range, 13-126 kg), with four children (10%) weighed ≤20 kg. For comparison purposes, 164 children underwent 178 AV fistula creations during the study period with a resultant AVF creation rate of 80%. Etiological factors contributing to their renal failure include obstructive uropathy in eight patients (19%), systemic lupus erythematosus in seven patients (17%), acute glomerulonephritis six patients (14%), nephrotic syndrome in four patients (10%), focal segmental glomerulosclerosis in four patients (10%), metabolic disease in four patients (10%), sarcoidosis in three patients (7%), hemolytic uremic syndrome in three patients (7%), and primary hyperoxaluria in three patients (7%). Among them, four (10%) failed their previous renal transplantation, resulting in subsequent necessity of hemodialysis.
At the time of BVT, eight patients (19%) had two or more central venous tunneled catheters. Thirty-four patients (81%) were receiving HD through a central venous tunneled dialysis catheter, with a mean length of HD dependence of 14 ± 6.5 months. Thirty-eight patients (90%) had received HD via at least one tunneled dialysis catheter, which included jugular vein catheter (n = 24, 57%), subclavian vein catheter (n = 7, 17%), or femoral vein catheter (n = 7, 17%).
The mean operative time of initial brachiobasilic AV fistula creation was 39 ± 12 minutes (range 35-64 minutes), while the mean operative time of BVT procedure was 66 ± 17 minutes (range 47-87 minutes). The mean follow-up period was 3.6 years. Functional maturation was not achieved in three transposed basilic vein fistulas (7%). The overall complication rate was 45% (19 patients), and these complications included thrombosis (17 patients, 40%) and steal syndrome (2 patients, 5%). Among the 17 patients (40%) who developed thrombosis, 4 were early thrombosis (≤30 days) and 13 were late thrombosis (>30 days). For those who developed early thrombosis, open surgical revision was performed on two fistulas (5%) while percutaneous thrombectomy was performed in the remaining two patients (5%) using AngioJet thrombectomy device (Boston Scientific, Natick, MA). Probable causes of these early thromboses included immediate postoperative hypotension (three patients), and small vessel caliber (one patient). Late BVT thrombosis occurred in 13 patients (31%). Eight of them (19%) underwent successful surgical thrombectomy and patch angioplasty of sclerotic or narrowed segment of the transposed basilic vein. The remaining five patients (12%) underwent percutaneous intervention including balloon angioplasty and endovascular thrombectomy. These endovascular interventions included percutaneous thrombectomy using AngioJet device (Boston Scientific) and transluminal balloon angioplasty. Time period of BVT thrombosis ranged from 0 to 436 days. Two patients developed steal syndrome, which occurred 16 month and 22 months, respectively, following the BVT creation. Their steal symptoms included hand pain and finger cyanosis. Arterial steal syndrome was documented using arterial duplex ultrasound and angiogram in both patients. Both patients underwent successful distal revascularization and interval ligation with saphenous vein graft. Twenty-two patients (52%) received a kidney transplant during the postoperative period, and these included five living-related donors, four living-unrelated donors, and thirteen cadaveric kidney organs. The mean time to transplant was 452 days (range 64-683 days). One patient was converted to peritoneal dialysis one year following BVT.
Primary patency rates at 2 and 4 years were 78% and 72%, respectively (Fig. 1). Secondary patency rates at 2 and 4 years were 86% and 82%, respectively (Fig. 2). In a subgroup analysis, age greater than 10 years and weight greater than 20 kg were associated with improved primary and secondary patency rates compared to those younger than 10 years of age or less than 20 kg of bodyweight (p<0.03).
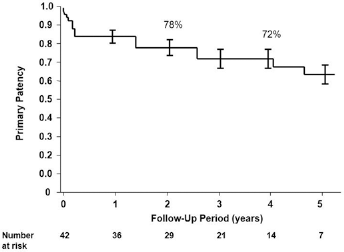
Kaplan-Meier curve of primary patency of pediatric basilic vein transposition.
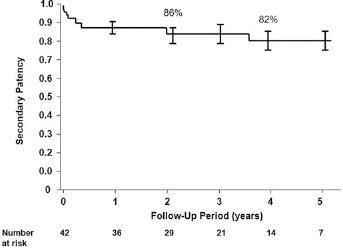
Kaplan-Meier curve of secondary patency of pediatric basilic vein transposition.
Discussion
The number of pediatric patients on hemodialysis has been on the rise, but AV fistula use in this patient population remains low with most children receiving hemodialysis through a central venous catheter (CVC) and only <15% receiving hemodialysis through an AV fistula (1). The lower rate of AV fistula placement in pediatric patients compared to adults may be attributed to many factors which include the fact that many surgeons are often reluctant to create an AV fistula in pediatric patients given the small caliber of the veins. Another factor that has been stated is using the CVC as a bridge to transplant, despite the fact that only 38% of pediatric patients receive a kidney transplant in their first year (11, 12). With the International Pediatric Fistula First Initiative recommending a fistula first approach in children, it is widely recognized that AV fistula creation offers several advantages over CVC or prosthetic AV graft. These include better patency, lower infection rate, and fewer long-term complications (11). In pediatric patients with suboptimal cephalic vein caliber or previously failed AV fistula, a staged BVT is our AV access of choice. Our experience described in this report notably represents the largest clinical series of pediatric BVT with long-term follow up.
Our preference for BVT compared to more distal forearm radiocephalic or antecubital brachiocephalic AV fistula veins is based on several considerations. First, these pediatric patients generally do not have adequate forearm or antecubital veins due to their frequent hospitalizations whereby these superficial veins are routinely punctured for blood draw or intravenous access. Additionally, the small caliber of these superficial veins in these children is not amenable to surgical manipulation of AV access creation. Notwithstanding these factors, one potential drawback of a transposed basilic vein AV fistula is high flow rate, which may predispose to a steal phenomenon. Nonetheless, we found the basilic vein is a better venous conduit for AV access creation due to its caliber. Since this procedure was first reported by Dagher et al in 1976, BVT has been used widely in adult patients with excellent results (13).
Due to the deep lying plane of the basilic vein, BVT requires an initial brachiobasilic anastomotic reconstruction and subsequent superficialization of the basilic vein, which can be performed either as a single-stage or two-stage procedure. Many researchers believe a two-stage BVT is superior to a one-stage procedure for multiple reasons. First, it allows the vein to mature and arterialize thereby reducing trauma, which is very relevant in the pediatric patient population in the setting of small caliber fragile veins. Other benefits of the two-stage approach are identifying problems that arise after the first-stage procedure such as steal syndrome, hematoma, or failure of the vein to mature, which can be dealt with prior to transposition or, in selected cases, the second-stage procedure can be abandoned all together (5, 14, 15). It also has been reported that twisting and hematoma formation is less common with the two-stage procedure as compared to the single-stage procedure, given the less robust size of the basilic vein, which is more susceptible to hematoma formation or twisting during tunneling (4). Another potential complication with the one-stage procedure is that the vein can be restricted from maturation by the surrounding subcutaneous tissues after tunneling, which may result in failure of the access (5, 14–16).
Studies on AV fistula creation in pediatric patients with BVT is relatively scarce compared to adult literature. Kim and associates recently reported their experience of 15 children who underwent a two-staged BVT versus 13 children who underwent a one-stage BVT (5). The authors reported a 100% maturation rate in the two-stage basilic vein transposition compared to 52% in the rest of the AVF including one-stage BVT, and their one-year overall patency rate was 91% compared to 47%, respectively. The limitation of the study, which is similar to other AV access studies in the pediatric population, relates to the relatively small number of patients, with only 15 out of 42 AV access patients with a two-staged BVT (5). A recent study by Wartman et al (7) reported a single institutional experience of 93 children who underwent AF fistula operation, and this included 20 children who underwent BVT. The authors noted a remarkable overall two-year primary patency rate of 83% for all AV fistulas, with 89% for BVTs, which were performed in one stage. In contrast to other reported studies in the literature, Wartman and associates (7) did not find location of the AV fistula to be a factor that significantly affected patency rate. Bourquelot et al reported his institutional experience of 380 children undergoing AV fistula using microsurgical techniques during a 10-year interval, and found distal wrist AV fistula creation was possible in 78% of the children (17). The immediate patency rate was 96%. The non-maturation percentage was 10%. The 2- and 4-year secondary patency rates were 85% and 60% for radial-cephalic AV fistula, 72% and 60% for brachial-basilic AV fistula. In a subsequent report, the authors attributed their remarkable outcome to meticulous microsurgical technique and the use of elastic bandage for tourniquet to reduce arterial spasm (18). In our series, we found small children were particularly challenging, as those aged <10 years and bodyweight <20 kg were associated with lower patency rate compared to children of older age or greater bodyweight. This finding may be attributed to smaller venous caliber commonly encountered in younger or small children.
The complications in our series were largely related to thrombosis and steal syndrome. Early complication rate was minimal in our patients, which correlated with the reported complications in pediatric patients in the literature. In the series reported by Kim et al (5), the overall complication rate for two-staged BVT was 47% (7/15) including three patients with thrombosis, five patients with hematoma or bleeding and one patient with steal syndrome (treated with ligation). In the study reported by Wartman et al (7), the overall complications were minimal and included two steal syndrome patients out of the 20 BVT, who were treated with distal revascularization with interval ligation (DRIL). The relatively low complication rate observed in our study and other BVT studies might be partially attributed to the relatively good patency of the procedure, as complications, and specifically hematomas, have been associated with fistula thrombosis and failure (14, 15, 19).
Undoubtedly, there are several limitations in our study. All patients included in this study were children with inadequate cephalic venous conduit or failed AV fistula. Consequently, it is difficult to compare the outcome of this particular patient cohort with published reports of children with brachiocephalic or radiocephalic AV fistulas. Although our experience showed two-stage BVT is our preferred treatment strategy, this was not based on a comparative analysis with one-stage treatment strategy. Given the small patient sample size in our series, it was difficult to analyze our patient cohort with a control group. Lastly, the retrospective nature of this clinical study was certainly associated with patient and treatment selection bias. Despite these notable study shortcomings, we believe our study highlights the important role of two-stage BVT in children with difficult venous conduit for dialysis access.
In conclusion, two-stage basilic vein transposition is an excellent AV access with remarkable treatment outcomes when done properly in pediatric patients. Further large studies that compare two-stage basilic vein transposition to one-stage transposition are required to further assert the superiority of the technique and assess for other variables such as patient quality of life and cost effectiveness. Finally, the presence of a multidisciplinary approach in dealing with this patient population with an early referral to a specialized center with an experienced surgeon in pediatric AV access is of utmost importance.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.