
Abstract
Introduction:
Arteriovenous access (AVA)-related pain treated successfully with runoff-venous decompression of the causative nerve, following ultrasound (US)-assisted preoperative evaluation, has never been reported.
Case presentation:
A 57-year-old man suffering from constant exhausting pains along the outflow cephalic vein of the radiocephalic arteriovenous fistula at the wrist and the antecubital fossa, was treated surgically after the diagnosis of AVA-related pain derived from cephalic vein compression on two peripheral cutaneous nerves, the superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve (LACN).
Technique:
The SRN and LACN, which ran along and/or provided sensory innervation to the painful regions in the upper limb, were traced using ultrasonography in the short axis and proved to be compressed by and in contact with veins where the pain existed, at the wrist and the antecubital fossa. Once diagnostic US-guided blocks of both were performed and pain disappeared, they were identified as the causative nerves. The cephalic venous decompression surgeries that separated and transposed the veins away from the SRN and the LACN were performed sequentially under pneumatic tourniquet inflation to improve nerve visualization.
Results:
The pains disappeared after the operations. An adequate length of the runoff cephalic vein was maintained for needle cannulations during hemodialysis.
Conclusions:
Outflow venous compression to the peripheral nerves may be a cause of AVA-related pain. US-guided assessments of the nerves may improve the safety and efficiency of venous decompression surgeries to treat AVA-related pains.
Introduction
Hemodialysis patients frequently develop upper limb pain, especially following ipsilateral arteriovenous access (AVA). Various etiologies of AVA-related pain include needle cannulation during hemodialysis, nerve injury during vascular access operation (i.e., superficial radial nerve [SRN] injury during radiocephalic AVA creation), and non-physiological blood circulation in the upper limb that causes steal syndrome, venous hypertension, and ischemic monomelic neuropathy (1, 2). Meanwhile, compressive peripheral neuropathies, such as carpal tunnel syndrome, cubital tunnel syndrome, Guyon’s canal syndrome, and cervical vertebral syndrome, have often been differentially diagnosed from AVA-related pain and treated as orthopedic or plastic surgery conditions (1-3).
The Japanese Society for Dialysis Therapy vascular access guidelines propose treatments of AVA-related pain related to steal syndrome and venous hypertension. However, detailed therapeutic approaches for other conditions are not stated (1) because relatively few patients develop access-related pain and, in most cases, the causes of the pain are unclear.
Recently, impressive technological developments in ultrasound (US) imaging have enabled close visualization and diagnoses of peripheral fine nerve impairments (4, 5). Therefore, we considered whether US examination could be used to evaluate AVA-related pain and to clarify whether there was a correlation between peripheral nerves and the pain.
Herein, we report the case of a patient who developed AVA-related neuralgia (radiocephalic AVA in the right wrist), and in whom the causative nerves were compressed by the outflow cephalic vein and could be localized on US-assisted assessments. The patient underwent curative surgical venous decompression of the affected nerves. We focus our description on the techniques used to identify the contributing nerves, using US scanning, and the safe and reliable performance of venous decompression surgeries.
Case description
A 57-year-old man had constant exhausting pain along the outflow cephalic vein of the radiocephalic arteriovenous fistula (AVF) in the right wrist. He was referred to our hospital after anesthesiologic and orthopedic consultations at another hospital. Malignant hypertension had led to chronic renal failure, and the patient had undergone hemodialysis for 78 months. He also had diabetes mellitus and vasospastic angina. The patient’s history of vascular access involved a first radiocephalic AVF created in the left wrist, which was repaired three times by percutaneous transluminal angioplasty within a year of creation. AVF ligation was performed for vessel pain that was similar to the problematic pain in the right forearm. The pain in the right wrist, which had gradually appeared 54 months after AVF creation and had persisted all day for 10 months, was located along the runoff vein from the AV anastomosis to the mid-forearm. The pain, exacerbated by compression, had worsened to the point where pregabalin in combination with non-steroidal anti-inflammatory agents was ineffective, and was interfering with daily living and sleeping. Radiating pain from the antecubital fossa to the axilla in the right upper arm was felt only during hemodialysis. There was no swelling of the upper arm, forearm, hand, and fingers. The needles for hemodialysis were cannulated proximally at the cephalic vein, cubital fossa as a blood-drawing site, and cephalic vein of the mid-upper arm as a blood-returning site to avoid punctures at the painful cephalic vein in the forearm (Fig. 1). He had never worn a tight wristwatch, or experienced trauma or job-related strenuous exertion of the forearm. The patient provided signed informed consent for inclusion in this study.
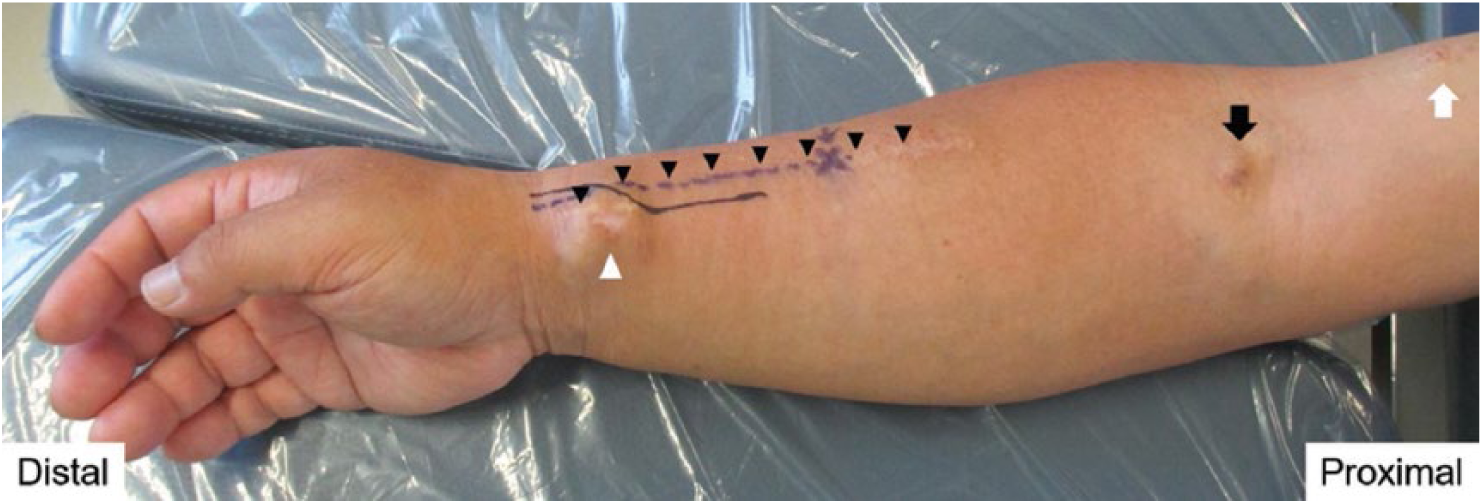
Location of the arteriovenous fistula, hemodialysis needle cannulation sites, and presenting pain in the right upper limb. White arrowhead indicates the arteriovenous fistula in the wrist. The skin elevation at the arteriovenous fistula was caused by the tortuous radial artery at the anastomosis and not by the anastomotic aneurysm. Black arrowheads indicate the painful lesion along the runoff cephalic vein. Black arrow locates the cannulation site for blood drawing and white arrow shows blood returning during hemodialysis.
Clinical and neurological examinations
The pain along the cephalic vein in the forearm was exacerbated by forced forearm pronation and palmar ulnar flexion of the wrist. The symptoms indicated entrapment of the SRN between the brachioradial muscle and long radial extensor muscle of the wrist (6). Tenderness over the lateral antecubital lesion, which also indicated radial nerve irritation, was observed (7).
Nerve conduction studies and others
Nerve conduction studies were performed to examine if the pain was associated with other peripheral nerve disorders such as carpal tunnel syndrome and cubital tunnel syndrome. Although distal latencies of the bilateral median nerves were slightly prolonged (4.08 msec [right] and 4.12 msec [left]), clinical features such as Tinel and Phalen signs associated with carpal tunnel syndrome were not observed. Motor nerve conduction velocities of the bilateral ulnar and radial nerves were normal. The findings of cubital tunnel syndrome, such as the delay of ulnar nerve velocities between areas above and below the elbow were not seen. Sensory nerve conduction velocities of the bilateral median nerves were mildly slow (43.6 msec [right] and 44.6 msec [left]) with distal sensory latencies slightly prolonged. Sensory nerve conduction velocity in the right ulnar nerve was slightly slower (42.9 msec) than normal and normal in the left. Sensory nerve conduction velocity of the left radial nerve was normal, but that of the right radial nerve could not be accurately measured due to pain. Diabetic peripheral neuropathy and amyloidosis with hemodialysis might affect the electrophysiological findings in these nerve conduction studies.
Cervical magnetic resonance imaging showed intervertebral disk bulging between the sixth and seventh cervical vertebrae. This clinical condition, which could have possibly been causing the pain, one of the neural symptoms of the radial nerve, was an indication of internal analgesic use and was not critical enough to warrant surgical treatment orthopedically.
Ultrasound visualization of peripheral nerves in the upper limb
Using ultrasonography, we examined the course of the SRN and musculocutaneous nerve (MCN) terminating as the lateral antebrachial cutaneous nerve (LACN) in the forearm, two nerves that were possibly stimulated by the outflow veins that caused the pain. The SRN ran closely along the cephalic vein in the distal forearm, consistent with previous descriptions (8), and the LACN, which provides sensory innervation to the anterolateral forearm where the cephalic vein is located, was in contact with the cephalic vein at the antecubital fossa (9) (Fig. 2).
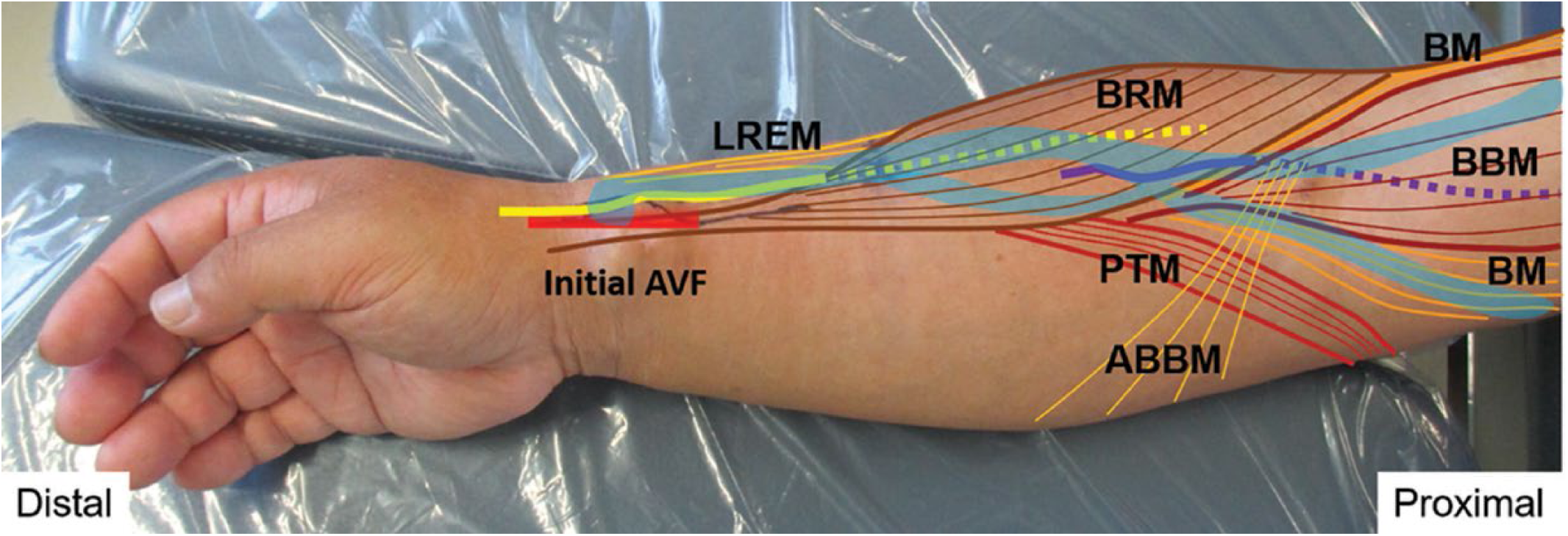
Anatomy of subdermal superficial radial and lateral antebrachial cutaneous nerves in relation to muscles and outflow veins of the arteriovenous fistula. The superficial radial nerve (subcutaneous segment in the wrist, yellow line; intermuscular segment in the forearm, yellow dotted line) courses subcutaneously behind the outflow cephalic vein (blue) two-fifths of the way along the distal forearm and from that point, runs deeply beneath the brachioradial muscle (BRM) apart from the vein. In the proximal forearm, the lateral antebrachial cutaneous nerve (subcutaneous segment at the antecubital fossa; purple line) passes behind the outflow vein (blue) and, as the musculocutaneous nerve (purple dotted line in the upper arm), runs deeply and apart from the vein between the biceps brachii muscle and the brachial muscle. ABBM = aponeurosis of biceps brachii muscle; AVF = arteriovenous fistula; BBM = biceps brachii muscle; BM = brachial muscle; BRM = brachioradial muscle; LREM = long radial extensor muscle of wrist; PTM = pronator teres muscle.
From the wrist to the elbow, US (HI VISION Avius: Hitachi Aloka Medical, Ltd, Tokyo, Japan) visualization of the SRN was performed by US tracing using the transducer (5-18 MHz) along the short axis (10). At the AV anastomosis, the SRN was adjacent to the outflow cephalic vein (posterior to it) and ran proximally, attached closely to the vein. The SRN ran deeply beneath the brachioradial muscle and separated from the cephalic vein from the wrist to approximately two-fifths of the length of the forearm. More proximally, it passed along the radial artery, located on the border of the brachioradial muscle and the long radial extensor muscle of the wrist. At the elbow, the SRN joined the posterior interosseous nerve and ran proximally as the radial nerve between the brachioradial muscle and brachial muscle (Fig. 3A, B, Video 1, available online as Supplementary material at www.vascular-access.info). The cephalic vein at the painful region was in contact with the SRN.
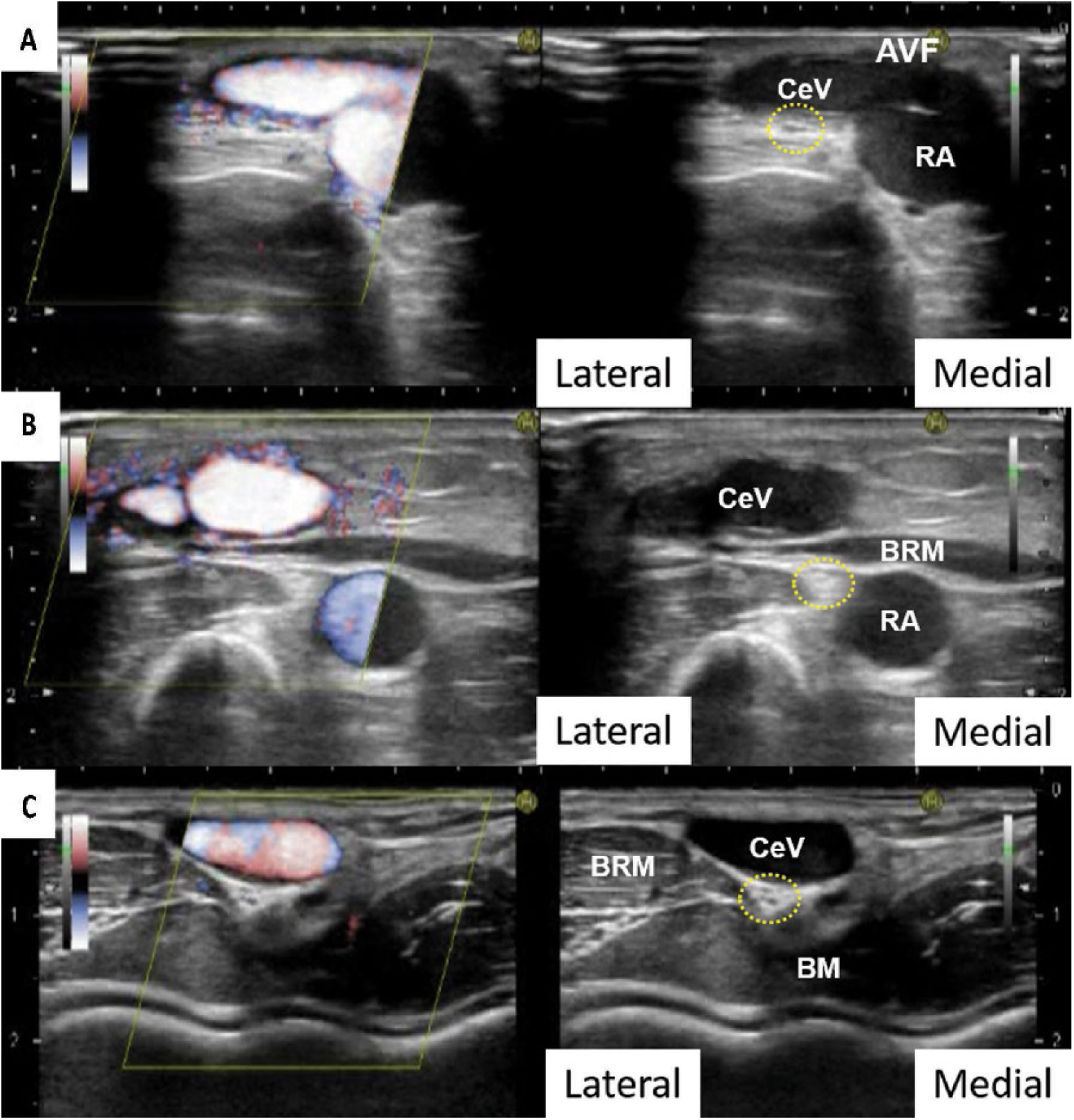
Ultrasounds of the superficial radial and lateral antebrachial cutaneous nerves in the upper limb in the short axis. (
From the antecubital fossa to the axilla, the MCN was traced in the transverse axis. The LACN, as a terminal of the MCN, was located just behind the cephalic vein at the antecubital fossa (Fig. 3C). It ran proximally, apart from the vein, as the MCN and passed deeply between the biceps brachii muscle and the brachial muscle. Near the axilla, it was located between the biceps brachii muscle and the coracobrachialis muscle (9) (Video 2, available online as Supplementary material at www.vascular-access.info). There was no nerve swelling, a sign of injury, on US (4, 5).
Diagnostic ultrasound-guided selective nerve blocks
To rule out the causative nerve, we performed US-guided selective nerve blocks on the MCN and SRN using 2.5 mL of 1% lidocaine for each nerve, as described previously (10). First, the MCN was blocked at the axilla without pain relief, but pain was subsequently ameliorated by SRN blockade at the middle of the forearm.
Hemodynamic assessment of the ipsilateral upper limb with AVF
We assessed the arterial inflow volume of the upper limb with AVA by Doppler US using the mean trace measurement. The flow volumes of the brachial artery and proximal radial artery to the AVF were 1405 mL/min and 1120 mL/min, respectively. The distal radial artery to the AVF had a retrograde flow of 102 mL/min. Arteriosclerosis was not observed in the upper limb.
Therefore, based on preoperative assessments, mainly using US-assisted nerve evaluations, we comprehensively diagnosed the hyperalgesia in the forearm as AVA-related pain caused by compressive stimulation of the SRN by the outflow cephalic vein.
Operative procedures of the first decompression surgery
Separation of the compressive cephalic vein from the SRN, by recreating the radiocephalic AVF proximal to the existing AVF and partial resection of the distal cephalic vein to the recreated AVF, was performed. The blood-drawing puncture sites of the cephalic vein in the forearm remained.
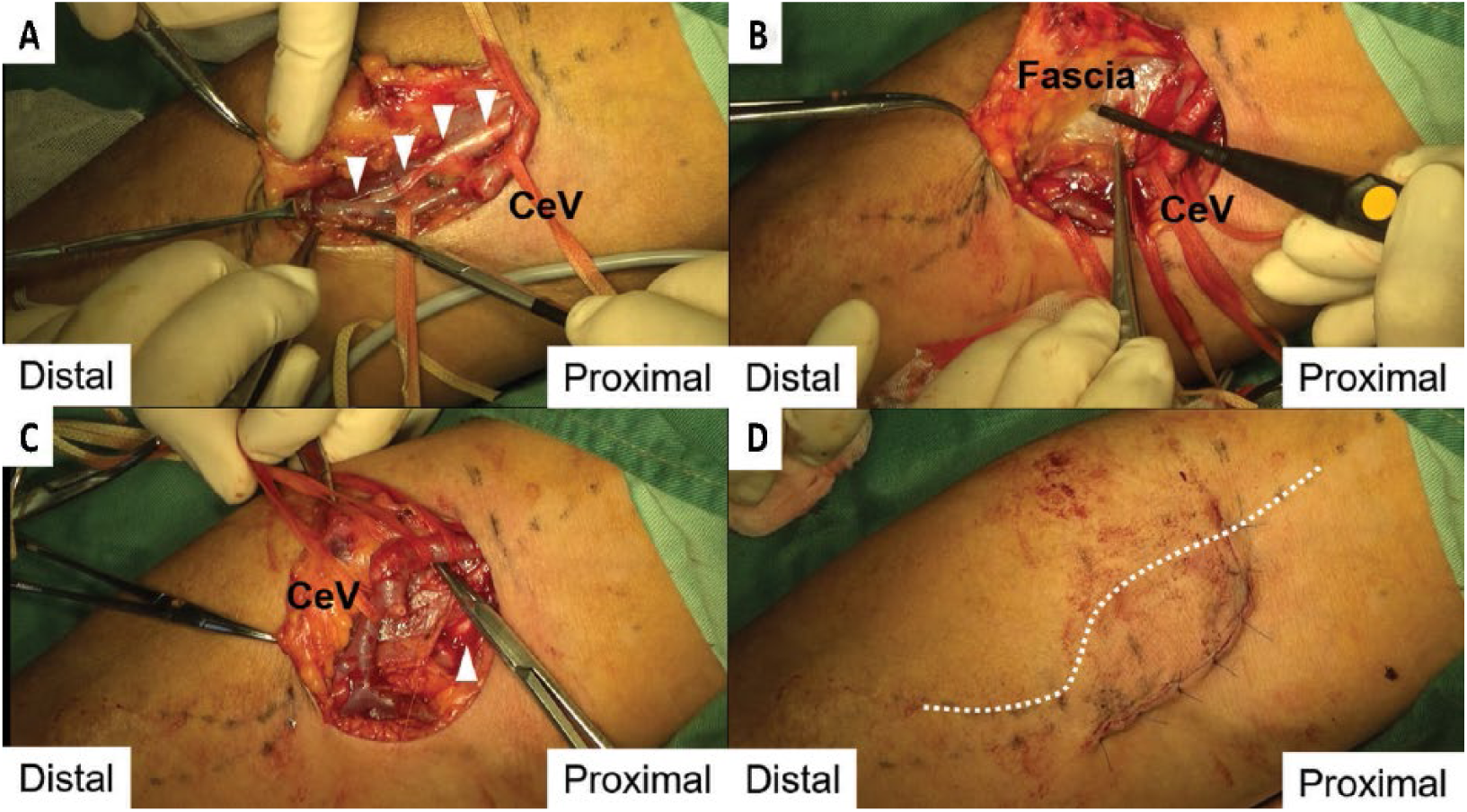
The operation began after administering a mixture of 1% lidocaine (2.5 mL), and 0.75% ropivacaine (2.5 mL) (9) for US-guided blockade of the MCN, which provided sensory innervation to the skin incision lesion in the wrist and had been diagnosed as the non-causative nerve. The procedure involved pneumatic tourniquet inflation in the upper arm with Esmarch exsanguination, to reduce hemorrhage and improve visualization of the SRN without the use of electronic cautery, which causes thermal damage to the SRN during release from the vein. The MCN was blocked to shorten the tourniquet inflation time without additional local anesthesia. A 6-cm longitudinal skin incision was made in the right wrist, proximal to the existing AVF. The outflow cephalic vein was encircled by a vessel loop and isolated from the surrounding soft tissue. Following identification of the SRN behind the vein, it was separated from the SRN between the existing AVF and the point where the SRN coursed beneath the brachioradial muscle (Fig. 4A, B, C). Immediately after releasing the vein from the SRN, the preceding spontaneous and oppressive pain along the cephalic vein disappeared. Subsequently, the proximal radial artery to the existing AVF was dissected and encircled by a vessel loop, and the tourniquet was released with a total inflation time of 37 minutes without use of additional local anesthesia. A small radiocephalic AVF, which was 3 mm in longitudinal diameter and 3 cm proximal to the initial AVF, was reconstructed and the resection of the cephalic vein compressing the SRN between the initial and neo-AVF was complete (Fig. 4D). The operation required 97 minutes.
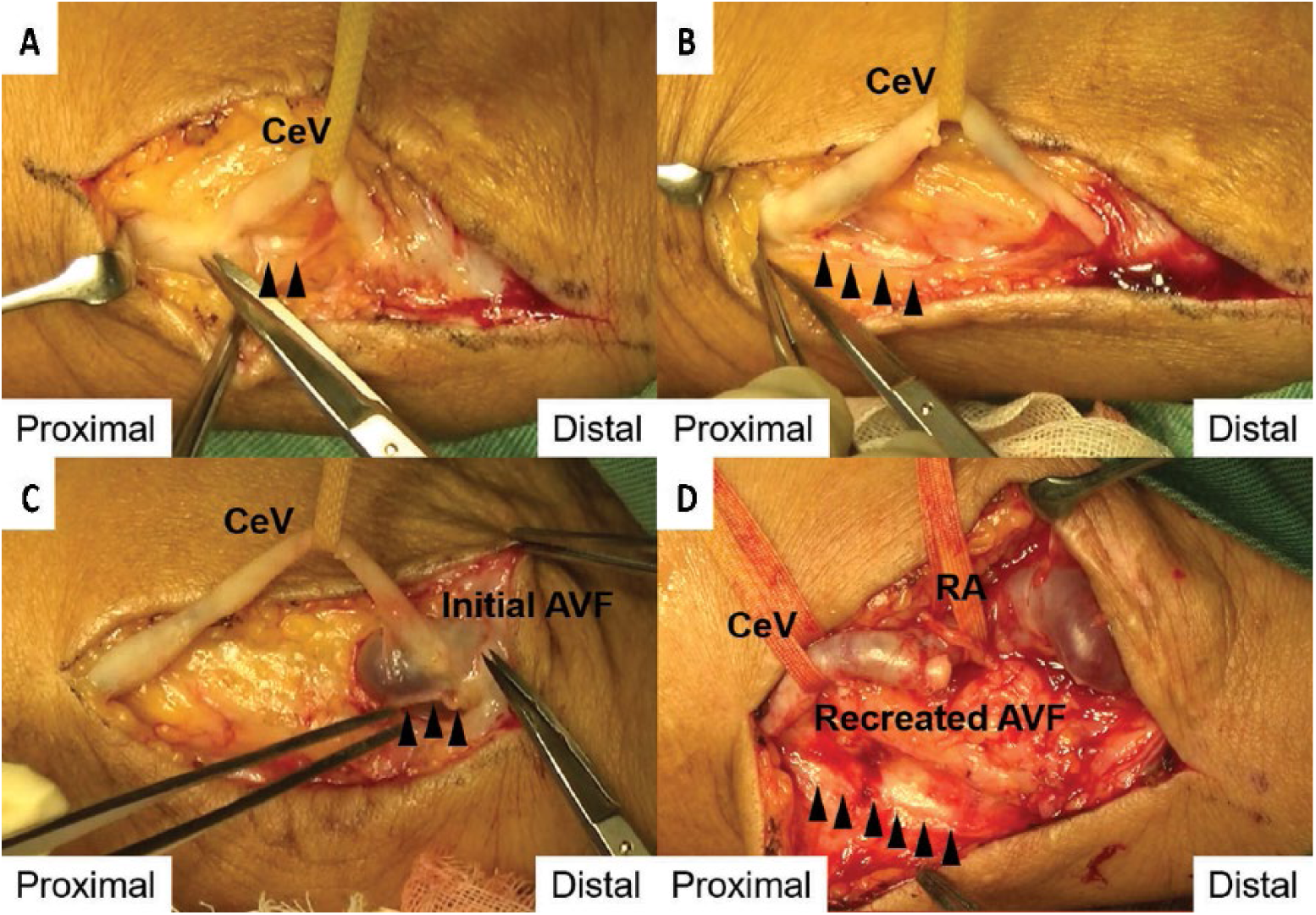
Cephalic venous decompression of the superficial radial nerve and proximal recreation of arteriovenous fistula in the right wrist. (
Clinical course after the first decompression surgery
The day after surgery, flow volume of the ipsilateral brachial artery measured by Doppler US decreased to 991.5 mL/min. After the operation, the hemodialysis-related radiating pain in the upper arm also disappeared. Paresthesia, which could be caused by intraoperative nerve injury, was not observed in the dorsal surface of the hand innervated by the SRN. The US image showed that the SRN was separated from the outflow vein in the peripheral forearm. After surgery, blood-drawing needle cannulation could be carried out at the cephalic vein in the forearm. Pain did not recur in the ipsilateral upper limb for two months after the operation, even during hemodialysis.
Shortly thereafter, continuous antecubital pain gradually occurred along the cephalic vein in the right upper limb, which radiated to the axilla and was aggravated during hemodialysis. The pain occurred according to the increase in flow volume of the ipsilateral brachial artery, without recurrence of the previous pain in the wrist. Three months after the operation, the flow volume of the brachial artery had increased to 1530 mL/min, which was almost the same as the preoperative flow volume. Therefore, the patient underwent outflow cephalic vein banding just proximal to the recreated AVF, for flow reduction, which reduced the flow to 1090 mL/min; however, the recurrent pain did not improve.
Four months after the first decompression surgery, a second decompression surgery was performed to separate the cephalic vein from the LACN, following the diagnostic US-guided selective MCN (terminating as the LACN) block. The cephalic vein at the painful antecubital region had been proved with ultrasonography to compress the LACN proximal to the branching for 4 cm in length.
Operative procedures of the second decompression surgery
An arc incision was made in the antecubital fossa under local anesthesia (1% lidocaine) and pneumatic tourniquet inflation in the upper arm with Esmarch exsanguination was performed as in the first decompression surgery. The MCN, the terminal of which was the causative LACN and provided sensory innervation in the antecubital incisional area, was not blocked because of the risk of intraoperative unawareness of the LACN injury. The cephalic vein was encircled by a vessel loop and separated from the LACN beneath (Fig. 5A). After releasing 4 cm of the cephalic vein from 4 cm of the LACN, the LACN was wrapped with surrounding soft tissue and the dissected fascia of the brachioradial muscle (Fig. 5B, C). The medial cubital vein connecting the cephalic vein to the basilic vein in the upper arm also remained, although two communicating branches to the deep vein were ligated and severed. The isolated portion of the cephalic vein, the main outflow route via the AVF, remained and was transposed to the subcutaneous pocket, separated from the wrapped LACN route (Fig. 5D). The tourniquet inflation time was 26 minutes and the operation time was 67 minutes.
Cephalic venous decompression of the lateral antebrachial cutaneous nerve and soft-tissue wrapping in the antecubital fossa. (
Clinical course after the second decompression surgery
The antecubital pain disappeared, even during hemodialysis. An US image confirmed separation of the LACN from the vein with soft connective tissue placed between them. Three months after the second decompression, recurrences of wrist and antecubital pain were not reported by the patient.
Discussion
In Japan, where hemodialysis durations are outstandingly longer than in other countries (11), vascular access guidelines (1) refer to problematic AVA-related pain broadly, whereas vascular access guidelines from other regions do not raise this issue, except for AVA-induced ischemic pain (12, 13). Usually, AVA-related pain is caused by needle cannulation during hemodialysis and hemodynamic change in the upper limb after AVA creation. Not many patients who develop AVA-induced space-occupying lesions that compress peripheral nerves of the upper limb have been treated successfully by their surgical removal or resections of the AVAs themselves (14, 15). Furthermore, no English reports have described AVA-related pain from venous thrill treated by decompression surgery using US-assisted preoperative evaluations.
Recently, ultrasonographic visualization of peripheral nerves along the upper limb has become general clinical practice (4, 5, 9, 10). First, US tracing of the peripheral nerve paths that are near and/or provide sensory innervation to the painful lesion are beneficial, to identify whether the nerves contact the outflow vein. Second, diagnostic US-guided selective nerve blocks can achieve pain relief (6, 7, 10, 16). We suggest that nerves that may cause runoff-venous compressive pain in the upper limb are the SRNs, which may be in contact with the cephalic vein at the wrist in the distal forearm, the LACN, which is the terminal of the MCN and may be in contact with the cephalic vein at the antecubital fossa, and the medial antebrachial cutaneous nerve, which may be in contact with the basilic vein in the distal upper arm (8-10, 17). One Japanese study reported AVA-related pain that was caused by outflow-venous compression on the LACN in the antecubital fossa and surgically treated using neurolysis without preoperative diagnostic imaging (1). We speculated that chronic and constant outflow-venous stimulation of the contacted peripheral nerves, such as by venous pressure and thrill from arterial blood inflow, may have caused the pain (1). The pain-causing portions of the peripheral nerves in contact with the superficial veins might be positioned proximally to the sensory-innervated skin region and may also be candidates for injury during venipuncture (10, 17).
Following identification of the causative nerve, we suggest that surgical strategies should be organized based on the anatomical relationships between the nerves and compressive superficial veins. Dellon has also recommended aggressive surgical treatment of upper extremity pain caused by nerve compression using diagnostic nerve blocks in plastic surgery (16). Appropriate surgical treatment for outflow-venous compressive pain, indicated in cases of refractory and debilitating pain, is considered decompression surgery since it liberates the causative nerve from the compressive vein. Procedures should separate the outflow vein from the cutaneous nerve, maintaining the existing AVA. In our case, proximal AVF recreation in the first operation and outflow-venous transposition in the second operation were performed successfully and both maintained adequate length of the runoff vein via the AVF by separating it from the causative nerves. In other cases, closure of the initial AVA, including resection of the contacted vein and creation of a new AVA in the contralateral upper limb, might be needed.
Pneumatic tourniquet has been used effectively and safely for both vascular access surgery and decompression surgery of entrapment neuropathy in the upper limb (18-20). For decompression of the peripheral nerves in the upper limb in which blood inflow has increased with AVA, pneumatic tourniquet may improve nerve visualization and reduce bleeding, without electrocautery and thermal damage. Tourniquet use facilitates safe runoff vein release from the fine nerve, without bleeding, under precise visualization.
Preoperatively, circulation in the ipsilateral limb might be considered to influence wrist and antecubital pain. In our patient, the existing AVF had comparatively high inflow volume. Therefore, to reduce the AVF flow, we first recreated a small AVF, 3 mm in diameter. Following pain recurrence resulting from increased AVF flow, we banded the outflow vein, based on a report that high access flow was related to nerve entrapment, presumably because the increased venous pressure and engorgement of surrounding structures pressed against the nerve in chronic hemodialysis patients (3). However, the recurrent antecubital pain was not controlled by flow reduction alone in our case. Further studies of whether high AVF flow volume influences access-related pain and whether AVF-flow reduction relieves pain are required.
In conclusion, direct runoff-venous compressive stimulation to peripheral cutaneous nerves may be one cause of AVA-related pain. Assessments of the positional relationship between the peripheral nerves and outflow veins, and diagnostic selective nerve blocks under US guidance, may inform strategies for venous decompression surgery of the nerves.