
Abstract
Introduction:
Arteriovenous graft (AVG) infection can result in life-threatening sepsis and loss of vascular access. A retrospective study was performed to establish an appropriate treatment strategy for AVG infection.
Methods:
A total of 50 cases of AVG infection were treated between January 2005 and June 2016. The surgical methods used were total graft excision (TGE) (n = 34), or partial graft excision (PGE) with interposition graft (n = 16).
Results:
Infection was noted at a puncture site (n = 22), a prior incision for surgery or endovascular therapy (n = 20), and abandoned (currently unused) grafts (n = 5). Infection occurred within 1 month after AVG creation (n = 1), or any intervention (n = 14), and more than 1 month after creation or intervention (n = 35). Simultaneous remote infection was identified in 7 patients, 2 of whom underwent an operation for infective endocarditis and spondylitis. After PGE, 5 patients (5/16, 31.2%) having recurrent infection were treated with further graft excision; however, no patient showed life-threatening complications. After TGE, a central venous catheter (CVC) was inserted and used for a median period of 90 days. Among 34 patients who underwent TGE, new vascular access was created in 18 patients at a median period of 2 months later, and 12 patients continued to use a CVC until last follow-up or death.
Conclusions:
PGE could be a treatment option for AVG infection to achieve both infection eradication and vascular access preservation in selected patients. Because of a higher risk of recurrent infection, sufficient surgical removal and careful postoperative management are warranted.
Introduction
Vascular access-related problems greatly influence the survival and quality of life of patients with chronic kidney disease. Infection is a common complication in an arteriovenous graft (AVG) created with polytetrafluoroethylene (PTFE); the reported infection rate being fivefold higher compared to an autogenous arteriovenous fistula (1). Prosthetic graft infection can lead to prolonged use of a catheter, a long duration of hospitalization, and life-threatening sepsis (2). Eradication of infection and vascular access salvage are both important considerations. Therefore, the treatment of AVG infection is challenging for vascular surgeons.
Traditionally, total graft excision (TGE) and the insertion of a central venous catheter (CVC) are recommended until the infection is controlled (3). To reduce the morbidities of surgical dissection to control inflow arteries, a subtotal graft excision with a remnant cuff is a preferred method without an increased risk of recurrent infection (4-6). In addition, partial graft excision (PGE) with an interposition graft has been tried in order to preserve vascular access and avoid the use of a CVC (7). PGE is considered a useful surgical method to achieve infection control, as well as vascular access salvage in selected patients.
There are limited data pertaining to the clinical presentation and treatment outcomes in patients with an infected AVG. Additionally, the extent of surgical excision to be performed for AVG infection remains debatable (8). We aim to report our experience regarding surgical treatment of an infected AVG for hemodialysis, to compare the results of PGE and TGE, and to establish an appropriate treatment strategy for both infection control and vascular access preservation.
Methods
Study population
Between January 2005 and June 2016, a total of 2,383 permanent vascular access for hemodialysis were created. Among them, 358 (15.0%) AVGs were created with expanded PTFE. A total of 50 cases of AVG infection were noted during the study period and treated with surgical excision. The estimated rate of AVG infection was 14.0%. Some patients were followed at other hemodialysis clinics, and our study included a few patients who initially underwent AVG creation at other hospitals. Thus, it is an estimated rate and might be lower than the actual rate of AVG infection. Using a retrospective review of medical records, we collected data pertaining to demographics, antibiotics, pathogens, types of AVG, the interval between AVG creation, or any intervention and surgical excision, and complications. This study was approved by the Seoul National University Hospital Institutional Review Board (1703-088-838) with a waiver of informed consent because the research would pose no more than minimal risk to the patients and would not have adverse effects on the subjects.
Diagnosis and management
AVG infection was suspected in a patient presenting with erythema, tenderness, purulent drainage, hemorrhage from the graft, or an exposed graft. In the absence of definitive clinical features of AVG infection, a duplex study was performed to determine the presence of fluid collection around the prosthetic graft. All patients with suspected AVG infection were admitted to the hospital, and intravenous empirical antibiotics were initiated after blood cultures were obtained. The duration of antibiotic treatment varied based on culture results and the patient’s clinical course. Echocardiography and fundus examination of the eye were performed to evaluate simultaneous remote infection.
The type of surgical technique used was based on: (i) the presence of fever; (ii) whether infection occurred within 30 days of the creation of the AVG or any surgical intervention; and (iii) whether well-incorporated segments could be detected during surgical exploration (Tab. I). If patients had fever, or if infection was noted to occur within 30 days after an operation or after any kind of intervention, TGE was preferred over PGE. Additionally, if we could find a well-incorporated segment during the operation, we changed the plan and tried to perform PGE with an interposition graft, even though the patient had a fever.
Indications for total versus partial graft excision
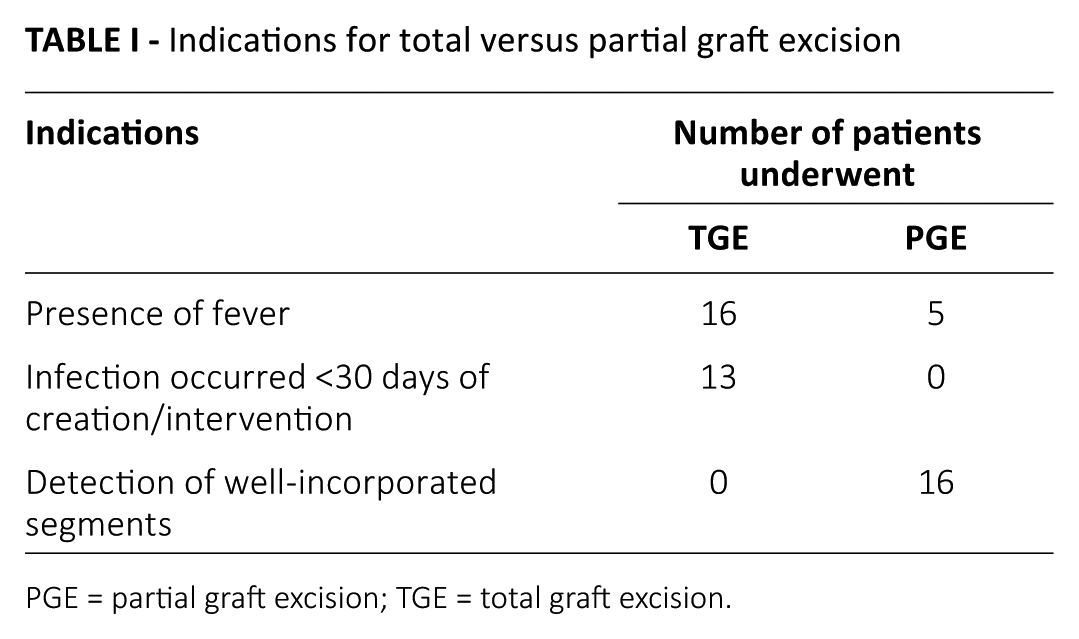
PGE = partial graft excision; TGE = total graft excision.
After TGE was performed, a temporary untunneled CVC was used, followed by the insertion of a tunneled permanent catheter after confirming that there was no bacteremia. Heparin or 0.9% normal saline was used for flushing CVCs. Following PGE, uninvolved segments were used for hemodialysis, and the newly inserted segment was used 2 weeks later.
Operation
For both TGE and PGE, those areas which grossly appeared clean were explored to locate sterile segments. A sterile segment was defined as a well-incorporated segment encased by adjacent tissue. If it was found, a new sterile PTFE graft was tunneled through the adjacent uninfected area and anastomosed to the sterile segment. After wound closure, the infected area was explored, and the infected graft and surrounding tissue were completely excised. If infection was suspected throughout the length of the graft, the graft was completely removed with only a 2 mm graft cuff remaining in the arterial anastomosis. The infected wound was left open and delayed wound closure was performed several days later. The excised graft and discharge were sent for microbiologic examination and culture. The operation was usually done under local anesthesia.
Postoperative care and follow-ups
Postoperatively, parenteral antibiotic treatment was instituted, usually with vancomycin, which was subsequently adjusted based on culture results. If the preoperative blood culture was positive, we performed it again until the result converted to negative. After discharge, patients had regular 3- to 6-month follow-up visits. Perioperative mortality was defined as death occurring within 30 days of the operation. Recurrent infection was defined as any sign of systemic infection requiring prolonged hospitalization or antibiotic use, or local infection requiring further excision within 3 months after the initial operation.
Statistical methods
Continuous data were summarized as a median with a range or mean with standard deviation, and compared with the t-test or Mann-Whitney test. Categorical data were summarized as proportions and percentages, and were compared using the chi-square test or the Fisher’s exact test. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS 18.0 software (SPSS Inc.).
Results
Patient characteristics
Our study included 50 cases of AVG infection in 47 patients, because 3 patients were observed to develop more than 1 episode of AVG infection. The median age was 66.5 (range 29-84) years, and the study included 33 men and 17 women. Thirty-seven (74%) had hypertension and 23 patients (46%) had diabetes mellitus. The median duration for which patients had been receiving hemodialysis was 37.5 months (range 2-432) (Tab. II).
Baseline characteristics of patients and vascular access
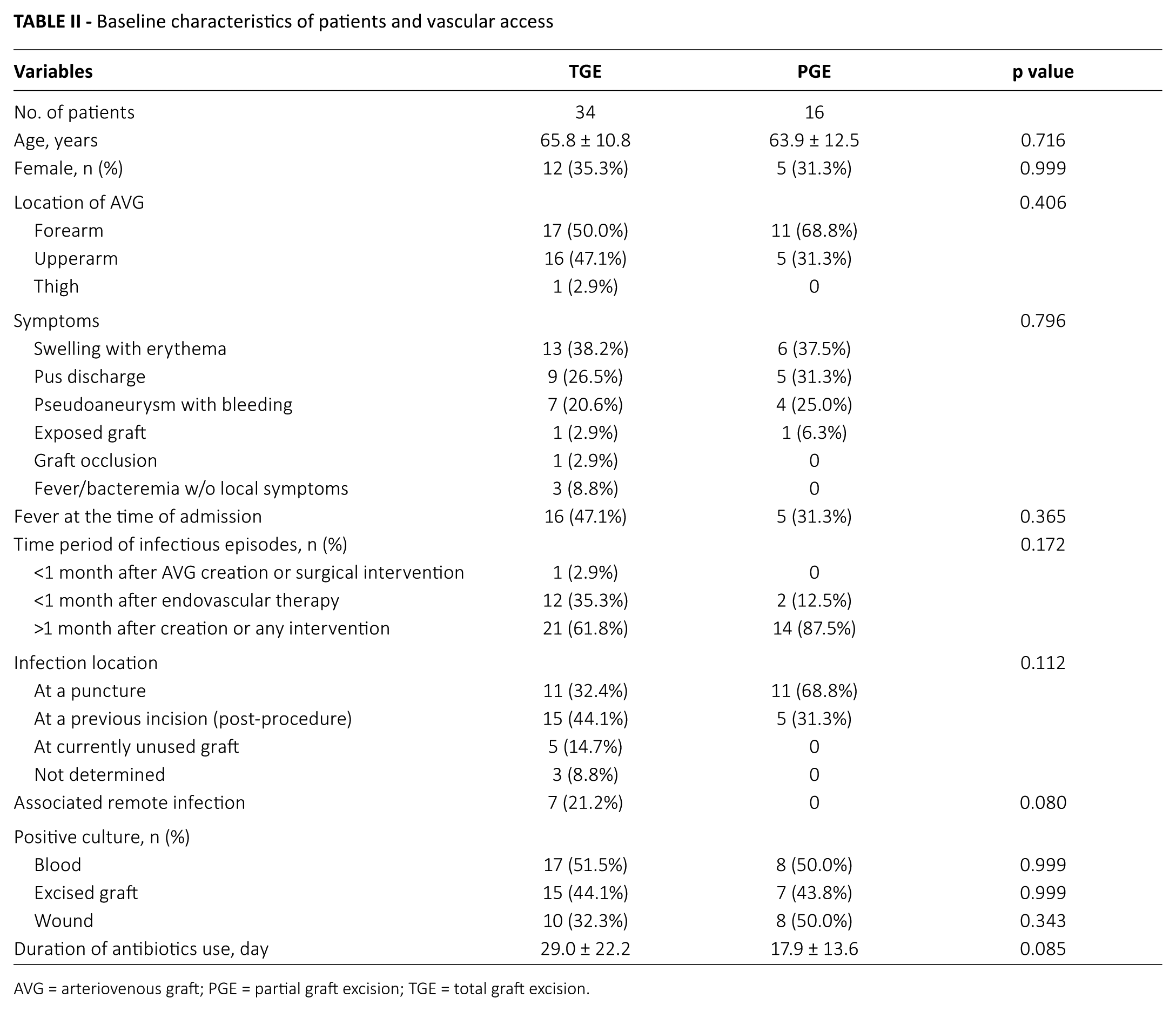
AVG = arteriovenous graft; PGE = partial graft excision; TGE = total graft excision.
Vascular access
The types of AVG were brachial-antecubital forearm loop access in 23 cases (46%), radial-antecubital forearm straight access in 2 (4%), brachial-axillary access in 18 (36%), femoral-saphenous inguinal loop access in 1 case (2%), and segmental graft in the autogenous access in 6 cases (12%). The median interval between the creation of vascular access and an episode of AVG infection was 23.5 months (range, 0-168). The median interval between previous intervention and an episode of AVG infection was 2.5 months (range, 0-35). The time periods for the occurrence of an infection within 1 month after AVG creation (n = 1) or after any intervention (n = 14), and more than 1 month after creation or intervention (n = 35) were noted.
Clinical and microbiologic manifestation
The most common symptoms were swelling with erythema in 19 cases (38%) followed by the discharge of pus in 14 (28%), pseudoaneurysm with or without overt bleeding in 11 (22%), graft exposure in 2 (4%), and simple graft occlusion in 1 case (2%). In 3 cases, the patients were admitted with fever and diagnosed with AVG infection during evaluation, including a duplex study. In 21 cases, the patients (42%) presented with fever at the time of admission. Among afebrile patients (n = 29), 5 had been treated with antibiotics from an outside hospital. The median duration of symptoms was 4 days (range, 1-21). Infection occurred at a puncture site in 22 cases (44%) and at a prior incision for surgery or endovascular therapy in 20 (40%). In 5 cases (10%), infection developed in a currently unused and thrombosed graft.
In 10 cases, the patients had been treated with antibiotics at some other hospital at the time of admission. In hospitalized patients, vancomycin (n = 37) and cefazolin (n = 5) were the common antibiotics used. The median duration of antibiotic treatment, including intravenous and oral modes of administration was 16 days (range, 3-80). Surgical wound culture was positive in 18 cases (36%), mostly with Staphylococcus aureus (n = 15). Blood culture was positive in 25 cases (50%); 23 grew S. aureus, 1 showed growth of Pseudomonas aeruginosa, and 1 had a culture positive for Serratia marcescens. A culture study performed on the removed graft was positive in 22 cases (44%), mostly for S. aureus (n = 20).
Remote simultaneous infection was noted in 7 cases. In 2 cases, the patients had infective endocarditis, and 1 of them underwent mitral valve replacement with the removal of infected thrombus from the mitral valve and superior vena cava. One patient had infectious spondylitis requiring a laminectomy. Two patients had septic arthritis: 1 developed osteomyelitis, and 1 developed concomitant bacterial pneumonia.
Surgical outcomes of TGE
TGE was performed in 34 cases (68%). The median duration of hospitalization was 12 days (range, 1-240). After excision, the wound was left open in 15 cases (15/34, 44%) and repaired at a mean of 5 days later. Recurrent infection occurred in 2 cases (2/34, 5.9%): 1 with continued bacteremia and the other with discharge from the operative wound. Both required excision of the remnant graft in 4 and 10 weeks after the initial operation, respectively. An 84-year-old man died 4 days after the operation due to sepsis. He presented with AVG occlusion with erythema and initially underwent endovascular therapy. After the percutaneous endovascular procedure, a TGE was performed for suspected infection, but he failed to recover from septic pneumonia.
The median duration of follow-up was 10 months (range, 1-66). The median duration of tunneled or untunneled CVC use was 90 days (range, 14-1,000), and no patient was noted to have a catheter-related infection. New vascular access was created in 18 cases. The median interval between graft excision and the creation of new vascular access was 2 months (range, 1-4). The types and locations of new vascular access were: an ipsilateral arteriovenous fistula (AVF) in 1, a contralateral AVF in 4, an ipsilateral AVG in 8, and a contralateral AVG in 5 cases. In 12 cases, the patients continued to use a CVC until last follow-up (n = 6), death (n = 5), or kidney transplantation (n = 1). In 4 cases, AVG infection occurred in the abandoned graft and new vascular access was not required (Fig. 1) (Tab. III).
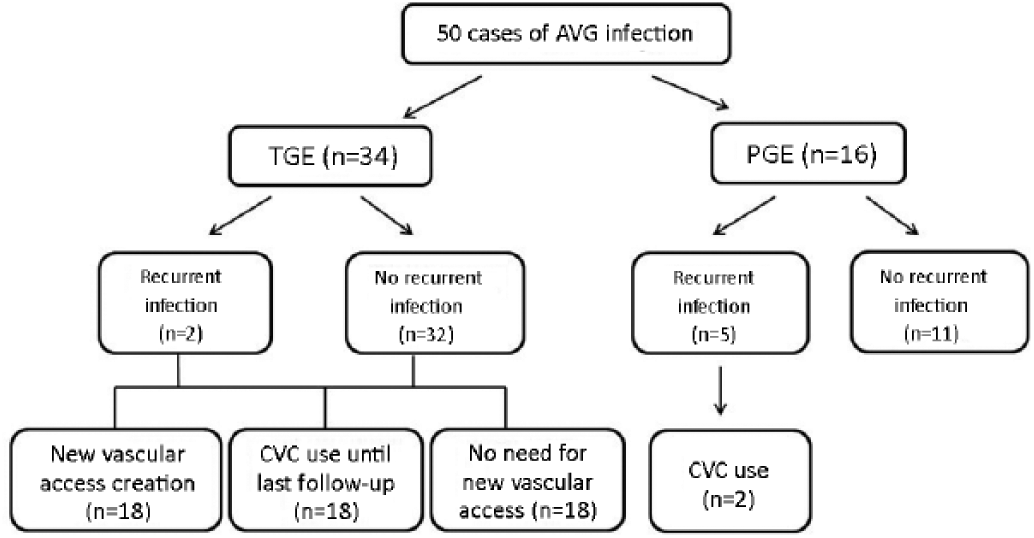
Summary of management and outcomes of AVG infection. AVG = arteriovenous graft; CVC = central venous catheter; PGE = partial graft excision; TGE = total graft excision.
The outcomes of total graft excision
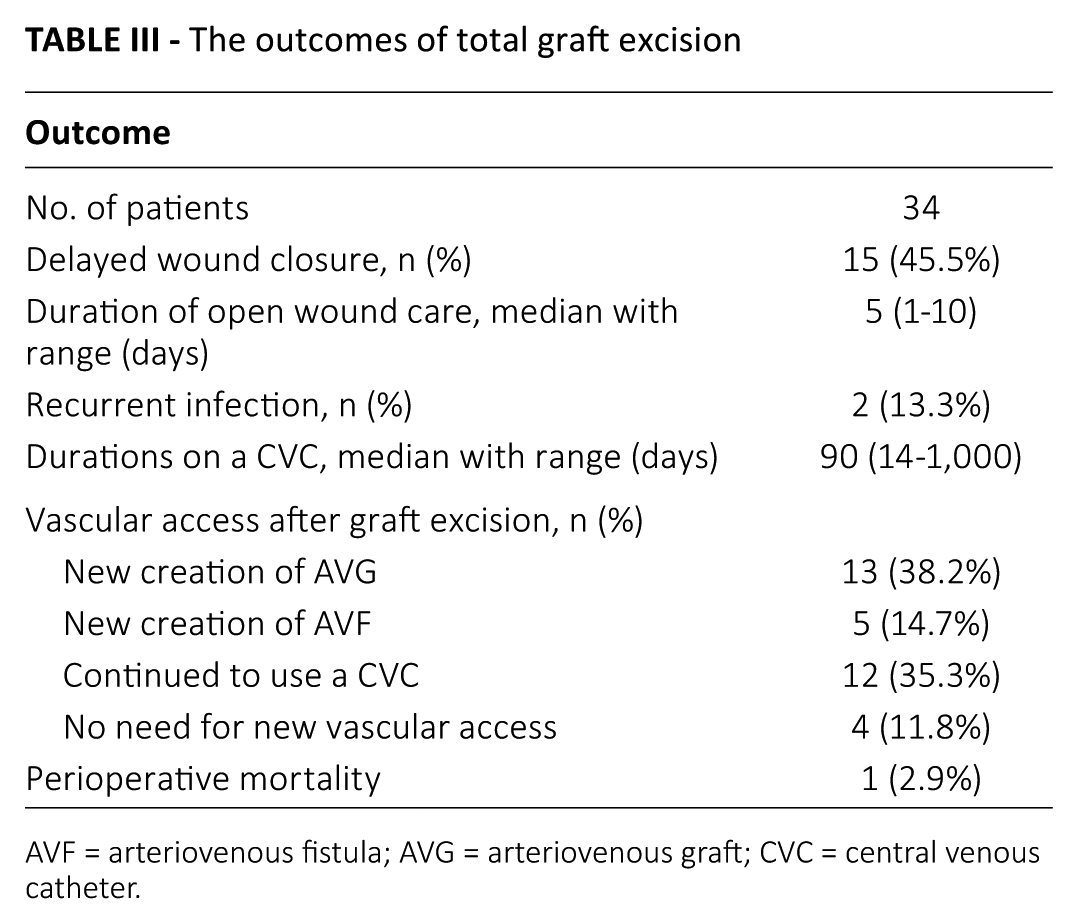
AVF = arteriovenous fistula; AVG = arteriovenous graft; CVC = central venous catheter.
Surgical outcome of PGE
PGE with an interposition graft was performed in 16 cases (32%). The median duration of hospital stay was 8 days (range, 1-24). Recurrent infection occurred in 5 cases (5/16, 31.2%). They were treated with further excision of grafts within 8 to 12 weeks after initial PGE. One patient eventually underwent conversion to TGE 5 months after the initial excision. After PGE, 2 patients with recurrent infection had a CVC inserted after further excision of the graft.
We compared patients with and without recurrent infection using Fisher’s exact test or Mann-Whitney U-test, and found no significant risk factor for re-infection. The characteristics that were analyzed included age, diabetes, fever, type of AVG, time period, and cause of infection, the duration of antibiotic treatment and the results of a culture study (Tab. IV). In patients who underwent PGE, 5 had fever at the time of admission and 2 of them developed recurrent infection. Additionally, 8 patients had bacteremia at the time of admission and 2 of them showed recurrent infection. However, neither the presence of fever nor bacteremia was a statistically significant risk factor for recurrent infection.
Clinical features of patients with and without recurrent infection after partial graft excision
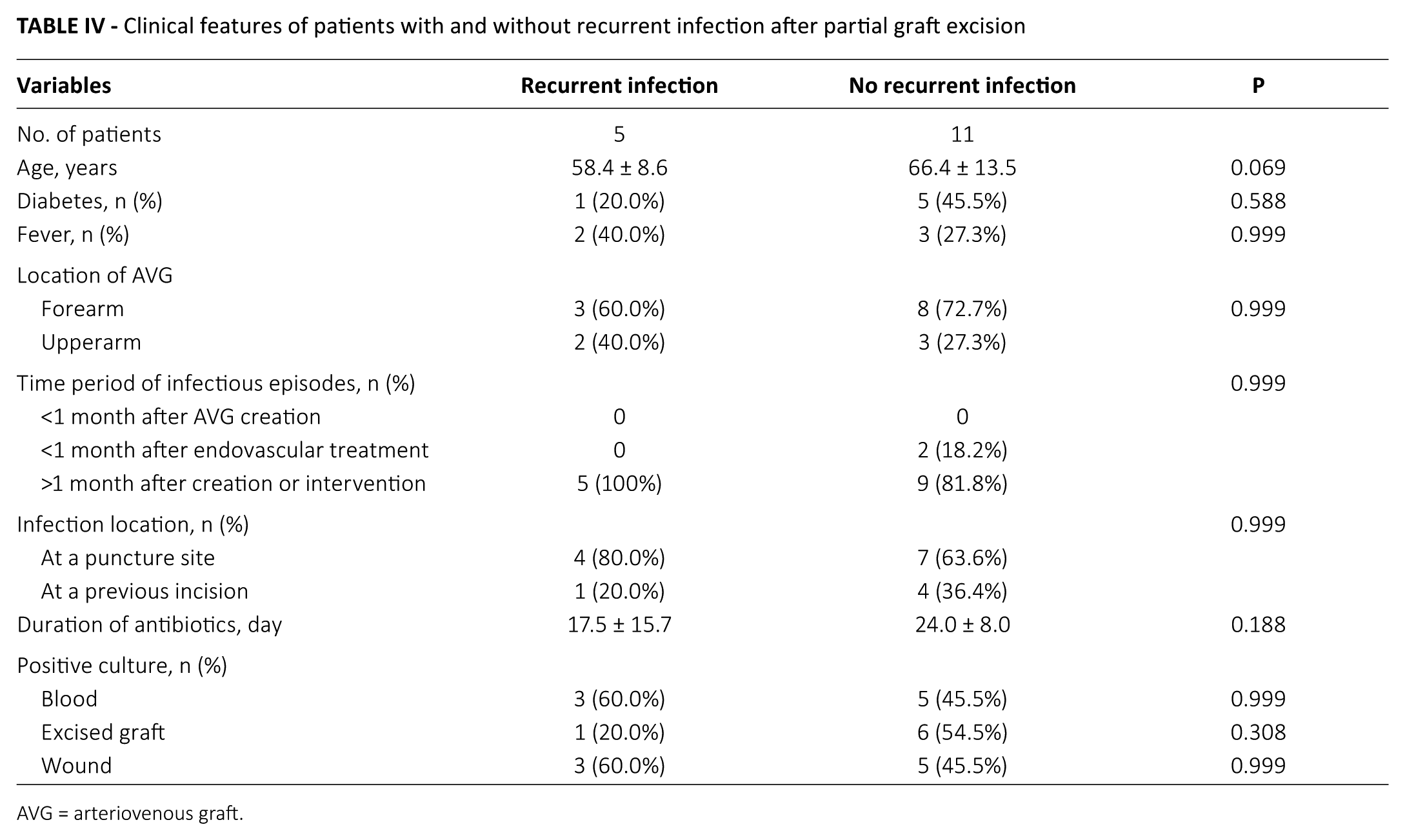
AVG = arteriovenous graft.
Discussion
In the treatment of AVG infection, it is imperative to aim for a balance between infection control and vascular access preservation, because of the limited anatomic options for vascular access creation. The earlier reports, regarding the partial removal of infected segment and the restoration of blood flow by Raju (9), showed 90% of graft salvage rate. Many centers adopted this surgical method; however, the feasibility of PGE for the eradication of infection is controversial.
Several studies have reported the outcomes of PGE. Ryan et al (3) have reported that graft patency and wound healing were achieved in 17 of 23 cases of infected AVG treated with PGE. They attempted PGE in cases where infection was localized to 1 segment and ultrasound revealed no fluid collection around the uninfected portions. Schutte et al (10) studied 91 cases treated with PGE, and reported that 18 patients developed recurrent local infection. In our study, 11 out of 16 patients were successfully treated with PGE. Based on these studies, PGE is feasible and acceptable in selected patients. Choosing patients who appropriately match selection criteria is important for successful PGE.
In this study, the choice of surgical methods was determined by 3 factors. First, the presence of fever was an indication for TGE. Vascular graft infection associated with systemic sepsis mandated complete graft removal, because remnants of the graft can serve as a reservoir for persistent bacteremia (11). Second, recent history of surgical manipulation mandated complete removal. Because a recently implanted graft is not sufficiently well incorporated to resist “tracking” of infection along the entire graft (12). Third, intraoperative finding was one of the most important considerations. An infected prosthetic graft does not get encased in scar tissue. This can be easily determined by experienced vascular surgeons (3, 5, 7, 13).
Although some patients experienced recurrent infection after PGE, they were all successfully treated with further local excision of the graft. No one showed life-threatening complications, such as sepsis or bleeding. Additionally, using the treatment algorithm, all patients with simultaneous remote infection were treated with TGE. Therefore, our criteria for patient selection were acceptable and reliable to determine the severity of infection. Some patients with fever or bacteremia were treated with PGE. They could possibly undergo PGE because intraoperatively the surgeon could find well-incorporated segments for the interposition graft.
Recurrent local infection is a major concern when attempting PGE. In an effort to avoid the insertion of a CVC, insufficient removal of an infected graft is possible (12). When PGE is attempted, sufficient removal is important until the surgeon encounters sterile well-encased segments. Achieving a balance between infection eradication and vascular access preservation must take precedence over strictly avoiding the insertion of a CVC. Additionally, vascular access preservation should not be the first priority over complete eradication of infection. A newly inserted interposition graft usually needs 2 weeks before needling occurs. If the length of the graft is not sufficient to allow needling, a temporary catheter may be used for a short period of time.
Patients treated with TGE should use a CVC for a few months. Many did not have new vascular access due to poor general condition and lack of a suitable anatomic site, which led to prolonged and repeated hospitalization and health care costs. Additionally, a CVC itself carries inherent risks of infectious complications. Although PGE carries a higher risk of recurrent infection, it should be considered in selected patients, especially in those who have already exhausted all possible anatomic sites for vascular access.
There was no clear guideline for the optimal duration of antibiotic use. For vascular graft infection, experts recommended an extended course (i.e., 4-6 weeks) of parenteral agents, although there are no randomized, controlled trials to support the recommendation (11). Recently, a French multidisciplinary group recommended postoperative parental antibiotic treatment for 6 weeks for prosthetic vascular graft infection (14). Several authorities advocate at least 4 weeks of antibiotic therapy for S. aureus bacteremia (15). Currently, it is ideal to follow general principles for vascular graft infection.
Some observations from this study have important clinical implications. First, we noted that 7 patients had simultaneous remote infection and 2 of them required major surgery for such infection. S. aureus, particularly, is known to be profoundly virulent with an associated 33% rate of metastatic complications (16). Simultaneous remote infection must be suspected when the patient develops sustained fever or bacteremia after graft excision. Second, in 10% of the patients, infection involved the currently unused graft. Infection can occur at a site of abandoned vascular access, which, therefore, should be carefully evaluated when the patient is being assessed for fever (13, 15). Third, utilizing an endovascular approach in management of an infected graft could cause septic emboli and serious complications. Thus, when an endovascular procedure is planned for a thrombosed graft or pseudoaneurysm, the possibility of infection should be evaluated.
Our study has several limitations. We only analyzed the outcomes in surgically treated patients, and information on medically treated cases were not included. An interposition graft was placed after PGE using only a PTFE graft. It would be useful to study and compare the benefits of other types of grafts, such as cryopreserved veins. We could not compare results based on microbiological studies, such as Gram-negative species, due to the small sample size.
In summary, PGE should be considered in selected patients to achieve both infection eradication and vascular access preservation. The presence of fever and a recent history of surgical intervention mandate a TGE, and intraoperative findings of a well-incorporated graft would be an indication for PGE. Because of a higher risk of recurrent infection after PGE, proper patient selection and sufficient surgical removal until the surgeon encounters sterile segments are essential. Additionally, effective postoperative management, such as with extended courses of antibiotics and careful wound care, is warranted.
Footnotes
Disclosures
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.