
Abstract
Aims and Background
Bone metastasis below the knee from primary lung cancer is rare. Discussion of such cases in a multidisciplinary team is important to establish the correct treatment approach.
Case report
We analyzed the diagnostic pathway of a 53-year-old female patient with a 5-month history of pain in the right foot. The patient underwent several radiological examinations for the pain. An initial diagnosis of osteoporotic syndrome was made, followed by a diagnosis of primary sarcoma. Only when the patient continued to have pain were other radiological examinations performed and a biopsy of the right ankle taken. This revealed a metastasis from undifferentiated pulmonary adenocarcinoma. A total-body computed tomography scan did not show any tumor locations apart from the primary lung cancer. The patient underwent chemotherapy and palliative therapies. This case has been reported for its rarity.
Keywords
Introduction
The incidence of skeletal metastases varies from 6% to 85% depending on the primary tumor (1). The incidence of bone metastases in lung cancer patients is approximately 30-40% (2). The most frequently involved sites are spine, pelvis, ribs, skull and proximal long bones. The lower limb is least affected by bone metastases with a rate inferior to 0.1% (3). We report the case of a 53-year-old woman who was diagnosed as having a metastasis to the foot from a lung adenocarcinoma. The lesion presented a problematic differential diagnosis which included primary cancer, inflammatory disease, trauma and rheumatoid disorders.
Case report
We present the case of a 53-year-old Caucasian woman who was a moderate cigarette smoker. One year before diagnosis she presented to a rheumatologist for progressive pain in her leg and right foot. The patient underwent magnetic resonance imaging (MRI), which showed ankle edema without fracture. Bone scintigraphy displayed radiotracer uptake in the right distal malleolus. The physician diagnosed Sudeck's syndrome and the patient was prescribed analgesic drugs, with moderate effectiveness.
Five months later (June 2012) the patient presented to our clinic for persistent pain in her leg and right foot. She had severe pain with impaired walking. Physical examination revealed evident edema of the right ankle and the pain increased with the superficial palpation of the right lateral malleolus. A computed tomography (CT) scan showed erosion of the lateral malleolus with edema. Laboratory tests showed an elevated carcinoembryonic antigen (CEA) level of 46.8 ng/mL. These results induced the suspicion of a malignant lesion. An MRI scan of the leg displayed destruction of the distal fibula. Two additional lesions appeared on MRI: one at the medial malleolus and the other lateral to the Achilles tendon. A primary sarcoma was the suspected diagnosis. The case was discussed by a multidisciplinary sarcoma board in Zurich University Hospital. Both surgeons and oncologists agreed that it was not possible to perform an operation because the lesions were multiple and the location not convenient for radical tumor removal. Fine-needle aspiration (FNA) of the largest ankle lesion was performed. Histological analysis showed an undifferentiated adenocarcinoma. FNA of a lymph node in the popliteal region gave the same histological result. Immunohistochemistry showed positivity for thyroid transcription factor-1 (TTF-1), which confirmed a possible lung origin (Fig. 1A and 1B). EGFR and ALK were wild type. A subsequent CT scan of the chest showed a mass in the upper lobe of the right lung measuring 17 × 13 mm. Positron emission tomography (PET)/CT confirmed pathological uptake in the right upper lobe related to a malignant process and in the osteolytic lesion in the right distal fibula. Considering the histological type, the stage of disease and the lack of predictive mutations, the patient was given 3-weekly chemotherapy with 75 mg/m2 cisplatin and 500 mg/m2 pemetrexed (4). The chemotherapy was well tolerated. Palliative radiotherapy was reserved for pain in case of no effectiveness of chemotherapy or at the end of the 6 cycles. The patient refused the administration of a bisphosphonate because she had planned dental care. CT scan after 2, 4 and 6 cycles of chemotherapy showed a decrease in the lung lesion to 12 × 10 mm. Also the tumor marker CEA decreased to 5.4 ng/mL after 6 cycles. The patient continued 3-weekly maintenance chemotherapy with pemetrexed according to the PARAMOUNT study (5). She maintained stable disease after the second cycle of maintenance therapy (Fig. 2A, B, C). MRI scan of right foot and knee showed disappearance of the popliteal lymph node and a partial response of the 3 ankle lesions (Fig. 3A, B, C). Clinically, at the end of 6 cycles of chemotherapy the patient had major pain control. She reduced the NSAID, opioid (fentanyl 50 μg patch) and pregabalin doses. Because of the limited decrease in volume of the ankle metastases she was given palliative radiation (30 Gy total dose) with benefit. In May 2013 the patient walked without support and had stopped taking pain killers. The last CT scan of the chest showed further shrinkage of the primary lung nodule and reduction of all 3 bone metastases in the ankle. Two months after the end of chemotherapy, 2 ankle lesions enlarged and she started to have pain. The case was discussed with the radiotherapist and the patient was given palliative radiotherapy to the ankle with partial benefit. She was in follow-up until September 2013 when a CT scan showed growth of the lung lesion. The patient decided to be followed further in another center.
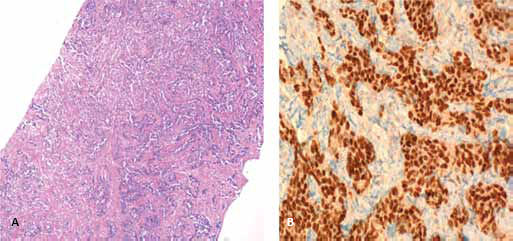
A) Histological picture and B) immunohistological stain showing TTF-1 positivity.
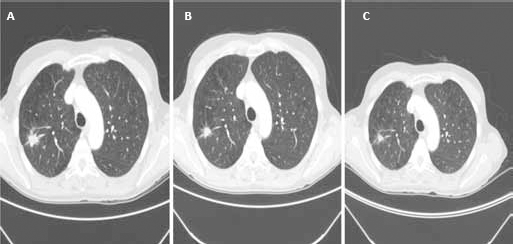
Computed tomography A) at the beginning of chemotherapy, B) after 4 cycles with a decrease in the lung lesion, and C) after 2 maintenance chemotherapy cycles showing stable disease.
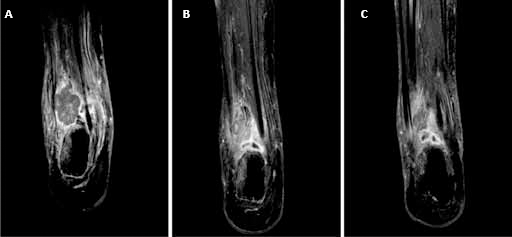
MRI scan of right foot A) at the beginning of chemotherapy, B) after 6 cycles showing reduction of the fibula lesion, and C) further reduction after 2 cycles of maintenance chemotherapy.
Discussion
The skeleton is the third most common site of cancer spread. Whereas lung and liver metastases are often not detected until the patient experiences symptoms, bone metastases are generally painful soon after their onset. The majority of bone metastases originate from cancers of the breast, lung and prostate, followed by thyroid and kidney (1, 3). Although metastatic disease to the skeleton affects 30% of cancer patients, acrometastasis (metastases to the foot and hand) is extremely rare (0.007% to 0.3%) (6). Metastases to the feet are often solitary or they are a manifestation of widely disseminated disease (7). The case presented here was characterized by some complexities. First of all, the painful lesion of the foot had multiple possible causes including primary cancer, inflammatory disease, trauma, and rheumatoid disease. The first MRI showed only edema without fracture. The long-lasting pain led to an initial misdiagnosis. One of the reasons for the delayed diagnosis was probably the rarity of this metastatic site and the absence of pulmonary symptoms. This case highlights the palliative role of radiotherapy for the treatment of pain, with improved quality of life. A retrospective review of foot metastases reported 694 patients with histologically proven metastatic skeletal disease (8). Only 14 cases of metastatic lesions to the foot were identified. The most common bones involved were the calcaneus and the talus (in 6 patients each) (8).
The literature on metastases to lower limb bones is scarce. Letanche et al (9), Ganjoo et al (10) and Pauzner et al (11) have described cases of metastases below the knee or elbow from lung cancer. The rarity of a malignant tumor located in the foot can lead to misinterpretation of a lesion visible on MRI and bone scan. The patient described by us had a metastasis from severely undifferentiated adenocarcinoma. Stage IV NSCLC is an incurable disease.
Conclusion
Very few cases of acrometastasis have been described in the absence of other previous metastases. A multidisciplinary approach involving experts of different medical fields is essential to reach an early and correct diagnosis. Meanwhile, a personalized therapeutic approach for symptom control is warranted.
Footnotes
Financial support: None.
Conflict of interests: None.