
Abstract
Aims and Background
Oropharyngeal candidiasis is a common disorder in head and neck cancer patients (HNCPs) who underwent (chemo)-radiotherapy. An Italian survey was conducted in order to investigate radiation oncologists' behavior in regard to diagnosis, prevention, and treatment of oral candidiasis.
Methods and Study Design
Between April and May 2013, a national online 18-question survey was sent to major Italian radiotherapy centers.
Results
All Italian regions were represented and 86 radiation oncologists were involved. Eighty-three percent of responders estimated that oropharyngeal candidiasis occurred in 30%-40% of their HNCPs. The majority of responders were able to recognize oral mycosis when it occurred in a localized pseudomembranous form and all responders agreed with the fact that oral candidiasis was always associated with mucositis. A prophylactic therapy was prescribed occasionally by 35% and routinely by 20% of responders. Forty percent prescribed an antifungal drug in the case of suspected mycotic infection and 20% waited for symptomatic clinical evidence before prescribing a therapy. In the presence of candidiasis, mainly topical fluconazole (59%) and itraconazole (36%) were prescribed. Concomitant chemo-radiotherapy was first identified as a risk factor for mycosis occurrence and development. Ninety-nine percent of responders believed that oral mycosis was associated with increased toxicity and 44% of them interrupted treatment due to candidiasis.
Conclusions
A variety of approaches to oropharyngeal candidiasis emerges from this survey; further clinical trials are necessary to identify the best approach for oral mycosis prevention and treatment and to establish specific international guidelines for HNCPs.
Introduction
Head and neck cancers (HNCs) represent about 3% of all malignancies in Italy. Each year, about 12,000 new cases are observed (1). At diagnosis, HNC is often locally advanced, requiring combined modality treatment (2); a survival benefit of approximately 6% for chemo-radiotherapy over radiotherapy alone was documented by meta-analysis (3), but these treatments are related to increased toxicity. Recently, supportive care has been developed to improve quality of life and compliance with treatment in order to avoid toxicity-related interruptions limiting local control. In HNC patients (HNCPs), the most common adverse events of these treatments are mucositis and oral cavity infections, including fungal, whose major form is oropharyngeal candidiasis (OPC) (4). Oropharyngeal candidiasis is a common disorder among HNCPs during and following (chemo)-radiotherapy. A review revealed that during chemo-radiotherapy, 74.5% of HNCPs had an oral fungal colonization, which often led to increased rates of clinical oral fungal infection. These data suggest the need for greater vigilance and the usefulness of prophylaxis (5). Oropharyngeal candidiasis usually causes uncomfortable oropharyngeal symptoms and complications such as pain, dysgeusia, anorexia, mucositis aggravation, malnutrition, and systemic fungal infection. Correct management of OPC is crucial, since a clinical fungal infection might lead to interruption and protraction of radiotherapy. Treatment interruption may be correlated with the risk of reduced antitumor efficacy, impairing local tumor control and patient survival (6). Oropharyngeal candidiasis clinical management appears to be variable, and different approaches are reported in the literature. Due to this wide spectrum, we proposed a national survey in order to understand how OPC is commonly observed and diagnosed in HNCPs in Italy and to investigate radiation oncologists' behavior regarding OPC prevention and treatment.
Materials and Methods
Between April and May 2013, a national survey was conducted among major Italian radiotherapy centers in order to investigate radiation oncologists' behavior concerning oropharyngeal mycosis. The survey was created with an online survey program (www.SurveyMonkey.com) and administered by e-mail. It consisted of 18 questions to analyze prevention, diagnosis, and treatment of oral mycosis in HNCPs treated with radiotherapy alone or chemo-radiotherapy. Twelve questions had a single answer option and the remaining 6 allowed for multiple answers. The survey was supported by the Head and Neck Study Group of the Italian Association of Radiation Oncologists and was subdivided into 4 sections. In the first section, personal data were investigated and divided into optional data fields (name, address, city, e-mail address, and phone number) and mandatory ones (region and district). Interviewees were asked for the number of HNCPs seen per month (less than 5, from 5 to 10, or more than 10) (Tab. I), which was considered indicative of responders' expertise. The second section of the survey analyzed the expected oropharyngeal candidiasis rates (less than 10%, about 20%, or 30%-40%), the clinical type (erythematous mycosis, localized or extensive pseudomembranous form, or angular cheilitis), concomitant mucositis grade associated with mycosis, and, in the case of symptomatic OPC, if a cultural examination on the oral cavity had been performed (Tab. II). The third section analyzed the timing of mycosis treatment (in a preventive or curative setting), the topical or systemic treatment adopted, and observed side effects (Tab. III). The last 4 sections analyzed factors considered to increase the risk of OPC and the general recommendations adopted in order to improve oral care or to prevent mycosis (Tab. IV).
Distribution of respondents for italian districts
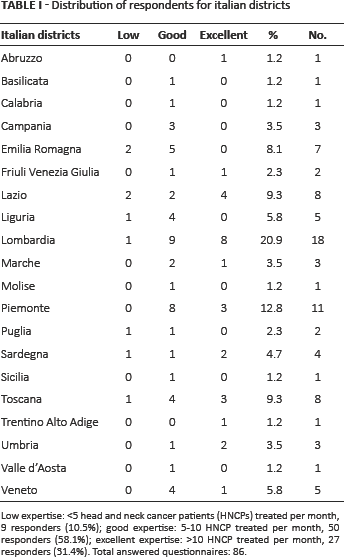
Low expertise: <5 head and neck cancer patients (HNCPs) treated per month, 9 responders (10.5%); good expertise: 5–10 HNCP treated per month, 50 responders (58.1%); excellent expertise: >10 HNCP treated per month, 27 responders (31.4%). Total answered questionnaires: 86.
Section II: oropharyngeal candidiasis diagnosis
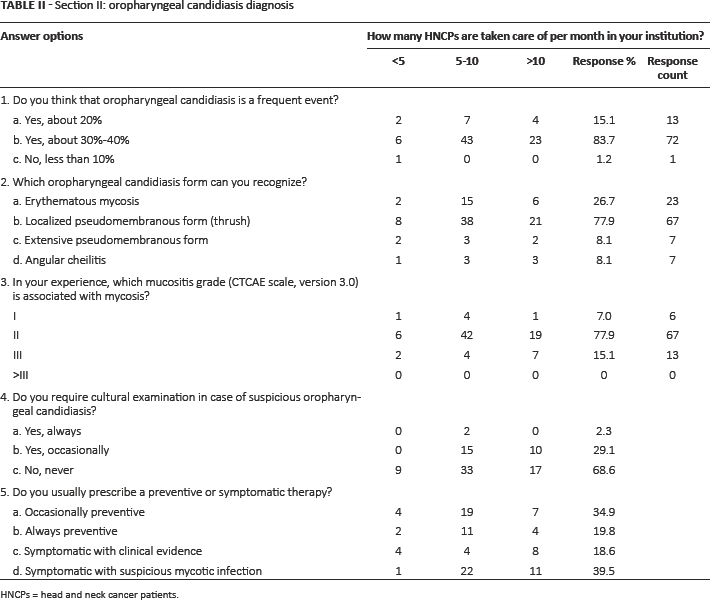
HNCPs = head and neck cancer patients.
Section III: oropharyngeal candidiasis prophylaxis or treatment
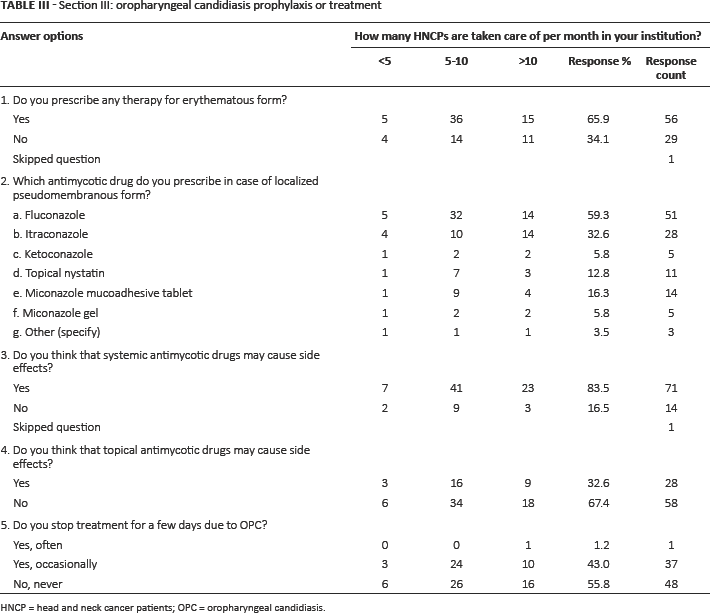
HNCP = head and neck cancer patients; OPC = oropharyngeal candidiasis.
Section IV: general recommendations and factors considered to increase the risk of oral mycosis
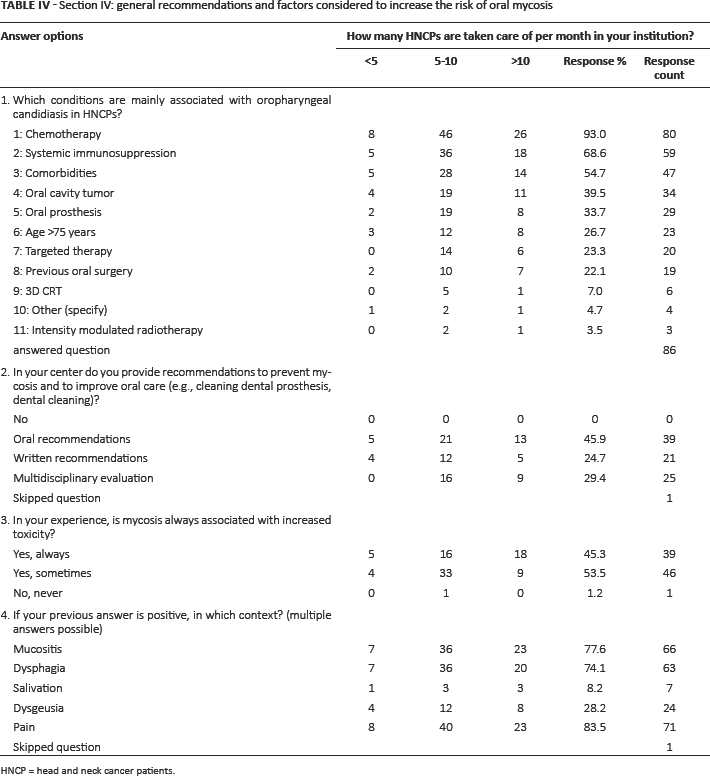
HNCP = head and neck cancer patients.
Analytical overview
Dataset analysis was clustered into 3 groups of responder expertise (low expertise, <5 HNCPs/month; good expertise, between 5 and 10 HNCPs/month; and excellent expertise, >10 HNCPs/month) (Tabs. II, III, and IV). A direct comparison between the 2 best expert groups was performed. The low-expertise group was excluded from comparison.
Statistical analysis
Descriptive statistics, Fisher exact tests (Fisher t [two-tailed]), or χ2 tests (Tx2) were performed using Winpepi software, where appropriate (7). When a significant χ2 association was found, adjusted residuals were calculated to identify those cells that contributed most to the χ2- Using the contingency table of Fisher exact tests, the examined specific endpoint was tested against the sum of remaining endpoints, considered together with the alternative hypothesis.
Results and Discussion
Regarding Section I, all 20 Italian regions were represented and 86 radiation oncologists were involved (Tab. I); the majority of responders (58%) treated 5–10 HNCPs per month, 31% more than 10 HNCPs, and 10.5% fewer than 5 HNCPs. The results of Section II (diagnostic problems relating to OPC), Section III (prophylactic and/or therapeutic treatments), and Section IV (general recommendations and risk factors relating to OPC) are presented in Tables II, III, and IV, respectively. No statistically significant difference was found between the replies from the 2 greater expertise groups.
This national survey showed that OPC is a common problem in HNCPs receiving radiotherapy. This finding may be considered relevant because the majority of radiation oncologists involved in this study were experienced clinicians in HNCP management (Tab. I). Indeed, 31% of responders reported examining more than 10 HNCPs/month and 58% from 5 to 10 HNCPs/month.
The literature indicates that HNCPs have a high risk of OPC and supports the importance of identification and management of the risk factors for OPC development (8, 9). The responders in our study believed that there were certain conditions associated with a greater risk of OPC, related in part to treatment and in part to HNCP characteristics. The first condition identified was combined chemo-radiotherapy. This may be justified by the fact that HNCPs receiving both treatments might be more immunosuppressed and more susceptible to infections. The second condition was that chemotherapy causes damage to the mucosal barrier, which may result in mucosal ulceration. This may in turn be associated with an increased invasion of Candida (5, 6, 8). The other conditions that significantly emerged were systemic immunosuppression and the presence of comorbidities, considering that OPC develops more easily in HNCPs with altered local and general host defense. Finally, the presence of oral prostheses was considered a risk factor. From this survey, other factors (such as combined treatment with targeted therapy or previous surgery on oral cavity and radiotherapy technique) appeared less correlated to OPC development.
In this survey, age >75 years did not seem to be related to a greater OPC rate (26.7%), as also reported in other studies (9), and was correlated with a series of factors, such as the use of smaller fields of radiotherapy due to less nodal involvement among elderly patients and wider involvement of salivary glands among younger patients, as well as the choice of less intensive chemotherapy or no chemotherapy. Other authors reported that elderly HNCPs (>70 years) have a higher incidence of grade III and IV acute toxicity (especially mucositis that is strictly correlated to mycosis) (10, 11) and that combined chemo-radiotherapy increases the toxicity risk in the elderly (2).
In the literature, 3 main clinical OPC features are described: pseudomembranous features, erythematous features, and cheilitis. It was not an aim of this survey to examine radiotherapy schedules and doses that could favor OPC development; the main endpoint of this study was to understand radiation oncologists' attitudes based on experience. The 2 most frequent clinical conditions, in the experience of responders, were erythematous candidiasis and pseudomembranous form (localized and extensive). These forms can be associated with several symptoms and toxicity worsening, which could lead to treatment interruption. Unexpectedly, in our survey we registered up to 43% of occasional therapy breaks, even as long as several days.
Fifty-five percent of responders were prescribed a preventive treatment. In the literature, there are differing data regarding the efficacy of prophylactic therapy. In 2006, Nicolatou-Galitis et al (12) evaluated the impact of fluconazole antifungal prophylaxis on the severity of oral mucositis in HNCPs receiving radiotherapy, and reported significant beneficial effect on the incidence of severe mucositis. This resulted in a significant beneficial impact on radiotherapy interruptions. Moreover, an Italian randomized double-blind trial showed a beneficial effect of oral suspension fluconazole vs placebo in preventing and delaying oropharyngeal candidiasis in HNCPs (13). More recent MASCC/ISOO guidelines published in 2010 highlighted that there is an inconsistency in the efficacy of topical antifungal agents used as antifungal prophylaxis (Level of evidence II, Recommendation grade C) and recommended the use of systemic fluconazole for the prevention of oral candidiasis in HNCPs receiving cancer therapy (Level of evidence I, Recommendation grade A) (5). However, an update in 2011 in HNCPs advised local prophylactic treatment (8). Despite these data, the role of oropharyngeal candidiasis prevention in HNCPs remains to be established.
An increase of non-C albicans infection has been reported (14), and there are concerns about the possible emergence of fluconazole-resistant fungal species (15).
In clinical practice, in regard to OPC treatment, the Infection Disease Society of America recommends topical agents as first-line therapy in milder forms of candidiasis (16), and the use of a broad spectrum of antifungal agents effective in all Candida species to prevent fluconazole resistance. From our study, it emerges that Italian radiation oncologists follow these guidelines and prescribe topically active agents in the case of localized pseudomembranous candidiasis, mainly fluconazole (59%) or itraconazole, but also other local treatment with new delivery mechanisms, such as the recently developed miconazole mucoadhesive tablet (16% of cases). Topical agents require sufficient intraoral residence time in order to interact with organisms and the oral environment. Consequently, specific recommendations for use, including maintaining contact time on the mucosa as long as possible, rinsing, gargling, and swallowing, should be given to these HNCPs (17). Furthermore, HNCP compliance may be low, due to the unpleasant taste and HNCPs' difficulty in swallowing due to mucositis and hyposalivation. Some of these drawbacks might be overcome by using a new form of miconazole mucoadhesive tablet, which may have some advantages over other topical agents, such as once daily application, lack of sugar sweetening, minimal side effects, and excellent compliance, although the cost of this agent has yet to be clarified (18). The drawbacks of topical therapies are associated with a high relapse rate and lead to a large use of systemic agents with the potential risk of causing resistant fungal species to emerge (17–19). Topical therapy has the advantage of a low risk of side effects compared to systemic drugs. This clearly emerges from this survey: 83.5% vs 32.5% of responders consider that systemic antimycotic drugs could cause greater side effects than topical therapies. Based on these observations, a possible useful compromise might be the preemptive treatment only of those HNCPs considered at higher risk of developing OPC.
A cultural examination of the oral cavity should be requested if there is clinical evidence of OPC in order to better select the antimycotic agent and reduce the risk of selecting resistant fungal species. In clinical practice, more than two thirds of responders do not require any cultural examination, even in the case of clinically suspected OPC.
From this study, it appears that clinicians involved in HNCP management are strongly sensitive to these issues. Our data show that all responders gave specific oral or written recommendations on the use of topical agents and specific oral hygiene instructions as indicated by the latest evidence. This survey could be considered highly representative of clinical behaviors in Italian centers, though a limitation might be the small number of responders. Good adherence to international indications is suggested by our study, but further and specific trials in HNCPs are required to prevent OPC development and to improve OPC management in HNCPs.
Footnotes
Acknowledgment
The authors thank the Head and Neck Study Group of the Italian Radiation Oncologist Association.
Financial support: None.
Conflict of interest: None.