
Abstract
Aims and background
The aim of this study was to monitor the mircostructure change of temporal lobe during the acute and subacute stage of radiation-induced brain injury using magnetic resonance diffusion tensor imaging (DTI) in nasopharyngeal carcinoma patients.
Methods and Study Design
Eighty patients diagnosed with nasopharyngeal carcinoma and treated with the first radiotherapy from July 2010 to May 2012 were enrolled. Routine brain magnetic resonance imaging (MRI) and DTI were conducted in all patients before and during radiotherapy (radiation dose was 20, 40, and 60 Gy, respectively). The MRI and DTI were also performed in the 1st, 2nd, and 3rd month after radiotherapy in 47 cases of 80 patients. The apparent diffusion coefficient (ADC) and fractional anisotropy (FA) of DTI during different stages were dynamically observed and analyzed.
Results
The ADC values were increased and the FA values were decreased with the increase of radiation dose (20, 40, and 60 Gy) during the radiotherapy, but there was no significant difference in ADC value or FA value between before and during radiotherapy (p>0.05). Compared with before radiotherapy, the ADC values were significantly increased and the FA values were significantly decreased at the 1st month, 2nd month, and 3rd month after radiotherapy (all p<0.05).
Conclusions
Diffusion tensor imaging reflects the microstructure change of radiation-induced brain injury in the acute and subacute stage, which provides an objective basis for early intervention of potential irreversible brain injury in the late delayed stage, and has important significance for improving the overall efficacy of radiotherapy.
Introduction
Nasopharyngeal carcinoma is a common head and neck tumor in southern China, and radiotherapy is the preferred treatment method (1, 2). As nasopharyngeal carcinoma often develops invasively, the radiation cannot avoid damage to important areas such as temporal lobe and brainstem. The range of fringe radiation on the lower front of bilateral temporal lobe is wide. This can lead to radiation-induced brain injury (RIBI), which affects the overall efficacy of radiotherapy, patient survival, and quality of life (3). Effective monitoring and control of RIBI are critical.
Magnetic resonance imaging (MRI) technology has provided a new research method for RIBI. It mainly includes magnetic resonance spectroscopy (MRS) and diffusion tensor imaging (DTI). Magnetic resonance spectroscopy is the most commonly used method that provides information about cellular energy metabolism, neuronal function, and selective neurotransmitter activity (4). In previous studies, single-voxel 1 H-MRS was used during and after radiotherapy to monitor the change of metabolite content (5). Two-dimensional or 3D multivoxel spectroscopy was also used by a minority of researchers in follow-up after radiotherapy (6). However, the complex mechanism of occurrence and development of RIBI is not clear (7). The combination of a variety of methods from different angles is helpful for further elucidating the mechanism of RIBI (8). Diffusion tensor imaging is an imaging method in which the physical and biochemical characteristics of brain tissue microstructure are reflected by the speed and direction of water molecule diffusion (9, 10). It was used earlier for studying cerebral infarction and brain tumor, and later for studying RIBI, with a small sample size (11, 12). The advantages and value of DTI for RIBI need further investigation.
In this study, DTI was performed on the temporal lobe in 80 patients who were diagnosed with nasopharyngeal carcinoma and treated with first radiotherapy. The dynamic change of temporal lobe microstructure during and after radiotherapy was observed and analyzed. The objective is to provide an objective basis for prevention of irreversible brain injury.
Materials and Methods
General data
Eighty patients (53 male and 27 female) who were first diagnosed with nasopharyngeal carcinoma by biopsy were enrolled in this study. Their ages were 33-76 years, with average age of 53.7 years. Patients with nasopharyngeal carcinoma combined with other brain diseases, systemic metabolic diseases, immune disorders, or temporal lobe defect were excluded. Cases with upward growth nasopharyngeal carcinoma were selected in this study and the radiation beam was mainly concentrated in the temporal lobe. All patients were treated with the first radiotherapy through the faciocervical field. The irradiated sites included the nasopharynx, neck, and bilateral temporal lobe. A standard fractionation radiotherapy (20 Gy/d, 5 days per week) was performed. Informed consent was obtained from patients before therapy and examination. Routine brain MRI and DTI were conducted in all patients before and during radiotherapy (radiation dose was 20 Gy, 40 Gy, and 60 Gy, respectively). For 47 cases of 80 patients, the examinations were also performed in the 1st, 2nd, and 3rd month after radiotherapy, respectively.
MRI method
All the examinations were performed in the same superconductive MRI scanner (GE Signa 1.5T Twinspeed/Excite II). The routine MRI sequences included axial plane T1-weighted imaging (repetition time [TR], 400 ms; echo time [TE], 15 ms), T2-weighted imaging (TR, 4000 ms; TE, 120 ms), and T2 fluid-attenuated inversion recovery (FLAIR) (TR, 6000 ms; TE, 120 ms; inversion time, 2000 ms). Axial plane echoplanar imaging was used for DTI, with scope and layer in line with T2 FLAIR. The imaging parameters were as follows: TR, 6000 ms; TE, 40 ms; layer thickness, 5.0 mm; interval, 0; field of view, 24 cm × 24 cm; resolution, 128 × 128; number of excitations, 1; b value, 1000 s/mm2. The DTI map was obtained from the diffusion sensitive gradient of 13 linear directions.
Image processing and data analysis
On the DTI map, the bilateral anterior temporal lobe was selected as region of interest to measure the average diffusion coefficient (ADC) and fractional anisotropy (FA) value, respectively. In order to avoid overlap between brain tissue and target region, the location and voxel size of each measurement were the same. The skull base sclerotin and bilateral ventricular temporal horn were avoided.
Statistical analysis
Statistical analysis was performed using SPSS 11.5 statistical software. Data are expressed as mean ± SD. One-way analysis of variance and Student t test were performed to determine the statistically significant differences among different groups. p<0.05 was considered as statistically significant.
Results
General characteristics of patients
No patients were treated with hormone, neurotrophic drug, or vasodilator during the observation stage. No obvious cerebral edema, intracranial hypertension, or nerve injury was detected by routine brain MRI. The colors of bilateral anterior temporal lobe on ADC and FA pseudocolor image were close. There was no obvious color difference between anterior and posterior parts of the bilateral temporal lobe.
Effect of radiotherapy on ADC and FA values
As shown in Table I, the ADC values were increased and the FA values were decreased with the increase of radiation dose (20, 40, and 60 Gy) during the radiotherapy, but there was no significant difference of ADC value or FA value between before radiotherapy and during radiotherapy (p>0.05). Compared with before radiotherapy, the ADC values were significantly increased and the FA values were significantly decreased at the 1st month, 2nd month, and 3rd month after radiotherapy (all p<0.05) (Tab. II).
Variations of ADC and FA values during radiotherapy

ADC = apparent diffusion coefficient; FA = fractional anisotropy.
Data expressed as mean ± SD, n = 80.
Variations of ADC and FA values within 3 months after radiotherapy
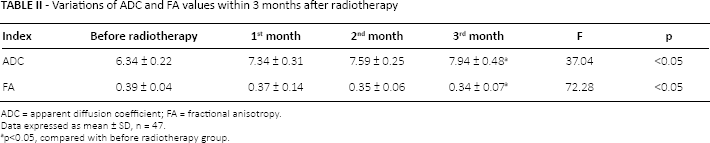
ADC = apparent diffusion coefficient; FA = fractional anlsotropy.
Data expressed as mean ± SD, n = 47.
p<0.05, compared with before radiotherapy group.
Discussion
Radiotherapy efficacy for nasopharyngeal carcinoma is significantly positively correlated to radiation dose, but the increased radiation dose can enhance the degree of injury in normal tissue. Radiation-induced brain injury is the main factor for limiting the radiation dose (1). The incidence of RIBI in nasopharyngeal carcinoma is 5%-24% (13). According to the time of symptom appearance after radiotherapy, the course of RIBI comprises 3 stages: acute stage, early delayed stage, and late delayed stage. The acute stage includes 2 weeks, in which a few symptoms will soon be restored. The early delayed stage, namely subacute stage, includes 3 months, with short-term symptoms and good prognosis. The late delayed stage includes several months to several years, in which the brain injury is progressive and irreversible, and the active treatment can only relieve the symptoms (14). Therefore, the RIBI in acute and subacute stage has become a hot topic for research.
Diffusion tensor imaging is a rapidly developing functional imaging method based on routine diffusion-weighted MRI (DW-MRI). In this method, the physical and biochemical characteristics of brain tissue microstructure are reflected by the speed and direction of water molecule diffusion, and the tissue microstructure, trend, and membrane permeability are detected without trauma. In infinite medium, the diffusion capacities of water molecules in different directions are the same, which is called isotropy, i.e., the same ADC. In different biological tissues, as influenced by cell membranes or macro-molecules, the diffusion capacities of water molecule in different directions are not the same, which is called anisotropy. The medullary white matter has high directivity. It is confirmed that the marrow phospholipids and cell membranes are the barriers perpendicular to medullary white matter fiber tracts. The normal medullary white matter fiber tracts are anisotropic, and the diffusion capacities are different in different pathologic conditions (15). Diffusion tensor imaging was originally used for detecting cerebral infarction and brain tumor. With the improvement of magnetic resonance equipment performance, DTI technology has become increasingly sophisticated and widely used in other diseases of the central nervous system and the whole body (16). In this study, DTI was applied to monitoring the microstructure change of RIBI in acute and subacute stages.
Results of this study show that, during the whole observation stage, the ADC value is increased while the FA value is decreased. The decreased amplitude of FA value during stage with radiation dose of 40-60 Gy is larger than before. This indicates that, from the beginning of radiotherapy to the stage with radiation dose of 60 Gy, the microcosmic structure of neural tissue has been changed, which affects the water molecule diffusion speed and direction in white matter fiber tracts. The effect of radiation on water diffusion direction is higher than on diffusion speed. There are several interpretations about the action mechanism of radiation on water diffusion capacity in cerebral white matter fiber tracts. On the one hand, the action of radiation on nervous tissue causes mitochondrial dysfunction. Thus the Na+-K+ pump on cell membrane cannot work normally, leading to the change of distribution ratio of intracellular and extracellular water molecules. Excessive extracellular water molecules enter the cell. The diffusion space of intracellular water molecule is restricted, resulting in reduction of diffusion speed. On the other hand, the increased intracellular water molecules cause the enlargement of cell volume and reduction of extracellular gap, which affects the diffusion of white matter fiber (17). It is believed that the biological effects of radiation can cause the medullary areosis, leading to change of ratio or existing state of free water and bound water. This is also one of the causes of decline of water molecule diffusion capacity. In this study, during radiotherapy, the FA value is more sensitive than the ADC value in reflecting the spatial structure change. This supports the view in a certain degree that the change of intracellular and extracellular water molecule distribution ratio dominates in this stage (18). The MRS study shows that, during the acute stage of RIBI, there is mainly cellular energy metabolism disturbance caused by impairment of mitochondrial function, without cell structure breakage (19). The 2 values can speculate the change of RIBI from spatial structure and material metabolism with good consistency, respectively.
In this study, in 3 months after radiotherapy (subacute stage of RIBI), the ADC value is significantly increased, while the FA value is significantly decreased with larger amplitude than during radiotherapy. Although no radiation directly acts with nervous tissue in this stage, the ionizing radiation-induced brain injury during radiotherapy has time continuity, and does not stop due to termination of radiation action. The mechanism of RIBI mainly includes direct brain tissue injury, cerebral vascular injury, immunologic injury, and free radical damage (12). With the aggravation of cerebral vascular injury, intimal hyperplasia and vessel wall hyaline degeneration appear, leading to vascular permeability change and formation of vasogenic edema (20). The increase of intercellular water molecules and reduction of molecule gap can limit the diffusion speed. In addition, there may be inflammatory reaction in this stage in a certain degree. The inflammatory cell infiltration can limit the diffusion speed and direction of water molecules. Unlike the acute stage, the brain injury in the subacute stage is not with a single injury mechanism, but the combined effect of several mechanisms. This leads to the decrease of FA value with larger amplitude than that during radiotherapy. This study illuminates that, after radiotherapy, the value of DTI reflecting the microstructure change of RIBI is further embodied, with aggravation of cellular edema and formation of vasogenic edema. This is consistent with a previous study (21). Through the retrospective analysis, we find that patients with nasopharyngeal carcinoma with larger decrease of FA value in subacute stage have episodic dizziness and headache symptoms. These symptoms last for a week and are spontaneously relieved or relieved after drug treatment. Thus the FA value in the subacute stage is correlated with the clinical symptoms.
The specific mechanism of RIBI is not clear. The evolution process and degree of brain injury are related to various factors such as irradiation field design, total radiation dose, fractionated dose, irradiation time and frequency, and individual differences. All patients in this study were treated with the standard fractionation radiotherapy. In every week, there is a 2-day buffer after receiving 10 Gy radiation. Although no abnormal sign was found during the observed stage, the microcosmic change of temporal lobe in brain tissue after edge radiation could be detected through dynamic follow-up with DTI. The morbidity of temporal lobe necrosis (TLN) is lower in the patients with nasopharyngeal carcinoma who received the repeated irradiation than in the neurogliocytoma patients who received the repeated high-dose irradiation. In this study, TLN was not found in the patients with nasopharyngeal carcinoma who received the repeated irradiation. However, the mechanism of TLN is complex. Sometimes, TLN happens a few years or even 10 years after radiotherapy. Therefore, we continue to follow-up the patients with nasopharyngeal carcinoma who received the repeated irradiation, and explore the correlations among TLN, ADC, and FA values.
Conclusions
Diffusion tensor imaging can reflect the microstructure change of RIBI at the molecular level, in the acute and sub-acute stage. It has provided an objective basis for early intervention of potential irreversible brain injury in the late delayed stage, and has important significance for improving the overall efficacy of radiotherapy in nasopharyngeal carcinoma and the quality of life of patients.
Footnotes
Financial support: Supported by the National Natural Science Foundation of China (No. 81360233; No. 81271389), the Key Project of Science and Technology of Hainan Province (No. ZDXM20130069), the Natural Science Foundation of Hainan Province (No. 812154), and the Scientific Research Project of Hainan Provincial Department of Health (No. 2011-23; No. 2012PT-19).
Conflict of interest: None.