
Abstract
Background
Aromatase inhibitors (AIs) are standard hormone therapy (HT) for the adjuvant treatment of postmenopausal endocrine-sensitive early breast cancer. Treatment discontinuation due to toxicity is an important issue that may help clinicians identify effective clinical interventions to allow adequate treatment duration. We reviewed the main reasons for interruption of AIs at our institution from 2006 to 2009.
Methods
236 patients treated with adjuvant AIs were eligible for analysis. Median age was 64 years (35-89), median follow-up 53 months (6-60). Prior adjuvant chemotherapy was taxane based in 47 patients and anthracycline based in 43 patients. 118 patients had received letrozole, 101 anastrozole, and 17 exemestane.
Results
Twenty-four patients (10%) needed discontinuation of the first AI assigned as a result of toxicity. Grade 2/3 arthralgia was the main reason for discontinuation in 13/24 patients. No differences in the incidence of arthralgia were noted in patients who had received taxanes or anthracyclines. Headache, alopecia, itching, diffuse skin reaction, allergic reaction with hypertensive crisis, xerostomia and xerophthalmia, insomnia and somnolence were the other reasons for discontinuation. In multivariate logistic regression analysis, age (65 years) and HT were independent factors associated with the onset of arthralgia (p = 0.006 and p = 0.008, respectively; OR 2.65, 95% CI 1.32-5.31). Alternative HT (AI or tamoxifen) was offered to patients who wanted or needed to permanently interrupt the ongoing drug.
Conclusions
In our analysis, 10% of patients discontinued the first AI assigned because of toxicity. Median time course of all adverse events leading to HT discontinuation was 155 days and 135 days for arthralgia. A switch to alternative HT with toxicity monitoring is a recommended option for avoiding premature and permanent interruption of an effective treatment.
Introduction
The majority of early breast cancers are diagnosed in postmenopausal women and are mainly estrogen receptor positive. The current standard adjuvant treatment consists of aromatase inhibitors (AIs), which are used as upfront treatment as well as in a switch strategy after 2-3 years of tamoxifen (1, 2). The most recent studies have shown higher activity of AIs in the postmenopausal setting in terms of progression-free survival. The results of these clinical trials have also demonstrated a favorable safety profile for AIs compared with tamoxifen (3-9). The discontinuation of adjuvant hormonal therapy (HT) can have a major clinical impact. Previous studies conducted in patients receiving tamoxifen have demonstrated the importance of adherence to adjuvant therapy (10-16). The discontinuation of adjuvant HT before the conclusion of the recommended years of treatment ranges between 20% and 50% in different studies. The discontinuation of adjuvant AIs in clinical trials ranged between 10% and 25%. In the ATAC trial, discontinuation due to adverse events was reported to be 28.3% for tamoxifen and 24.1% for anastrozole after 4 years (6). The discontinuation rates for letrozole and tamoxifen were lower, about 12%, after approximately the same period in the BIG trial (7). In the trial conducted by Huiart et al (12), 13,479 women with breast cancer who received at least 1 prescription of tamoxifen or AIs between 1998 and 2008 were analyzed. In the subgroup of patients who received AIs, 9.6% (150 of 1,562) switched treatment. Half of them switched from one AI to another AI, and the other half switched from an AI to tamoxifen. Switches occurred within the first year of treatment in 76% of cases, but no reasons are available for this treatment modification (12).
Few details are known about the specific causes for treatment discontinuation of adjuvant AI therapy in clinical practice due to adverse events induced by the drugs. Although these classes of drugs are well tolerated, a percentage of patients interrupt treatment because of toxicity. We conducted a retrospective single-center evaluation to assess the main reasons for the discontinuation of HT by patients with early-stage breast cancer.
Methods
All stage I-III endocrine-sensitive female breast cancer patients who were prescribed and started adjuvant HT with an AI after completing primary treatment for breast cancer since 2006 were eligible. In order for a patient to be considered eligible for analysis, a minimum treatment time up of 1 month and a minimum follow-up of 2 years were required. Adjuvant HT included the 3 approved AI molecules in Italy: anastrozole, letrozole and exemestane. The patients could have been treated with tamoxifen in a switching strategy. Written and oral informed consent to be treated with AIs was obtained from each patient. The e-chart data were reviewed to collect the reasons for discontinuation of endocrine therapy. The National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 4, were used to define the grade of toxicities.
Statistical method
Descriptive statistics were used to summarize pertinent study information. The associations between variables were tested by Pearson's chi-square test or Fisher's exact test as appropriate. Odds ratios (OR) and 95% confidence intervals (CI) were estimated for each variable. A multivariate logistic regression model was also developed using stepwise regression (forward selection) to compare the independent role of the different factors in arthralgia. The enter limit and remove limit were p = 0.10 and p = 0.15, respectively. The SPSS software (version 21.0, SPSS Inc., Chicago, IL, USA) was used for all statistical evaluations.
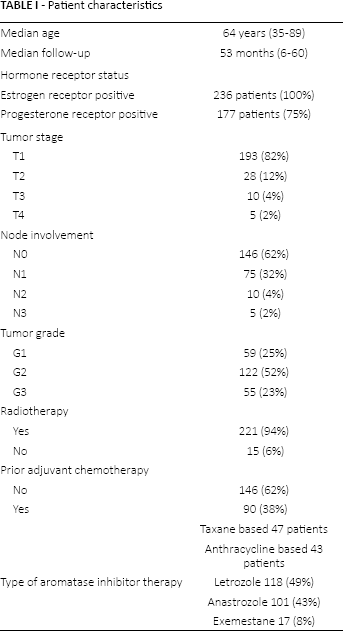
Patient characteristics
The main patient characteristics were: median age 64 years (range 35-89); median follow-up 24 months (range 6-28); prior adjuvant chemotherapy 90 patients, taxane based: 47 patients, anthracycline based: 43 patients. One hundred eighteen patients (49%) had received letrozole, 101 (43%) anastrozole, and 17 (8%) exemestane. Twenty-five (10.5%) patients were treated in a switching strategy with tamoxifen. Other characteristics are shown in Table I.
Patient characteristics
Results
The clinical data of 236 early breast cancer patients were retrieved. Median time of exposure to AIs was 4.3 years (median days of exposure 1,587: range 27-2,585). According to the CTCAE, arthralgia was the main toxicity (26.6%); it was grade 1 in 19.4%, grade 2 in 5.5%, and grade 3 in 1.7%. Overall, 24 of 236 patients (10%) needed discontinuation of AIs as a result of toxicity. Grade 2 and 3 arthralgia was the main reason for discontinuation in 13/24 patients (54%). No differences in the incidence of arthralgia were noted in patients who had received taxanes or anthracyclines. Grade 2 headache (in 2 patients), grade 2 thinning hair/alopecia (2 patients), grade 3 itching (2 patients), grade 3 diffuse skin reaction (1 patient), grade 3 allergic reaction with hypertensive crisis (1 patient), grade 2 xerostomia and xerophthalmia (1 patient), grade 2 insomnia (1 patient), and grade 2 somnolence (1 patient) were the other reasons for discontinuation (Fig. 1).
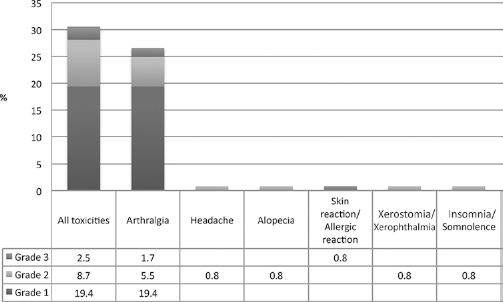
Toxicities leading to discontinuation of hormone therapy.
The median time of exposure to AIs to the most frequent adverse event (arthralgia) was 279 days (range 14-1,433). The median time course of all adverse events leading to discontinuation was 155 days (range 14-1,208), while for arthralgia it was 135 days (range 14-400). Of the 236 patients, 13 (5%) discontinued the first AI assigned in the first year of treatment mainly because of development of grade 2/3 arthralgia, whereas 7 (3%) permanently discontinued the treatment before completing 5 years of therapy. Time to discontinuation is reported in Figure 2.
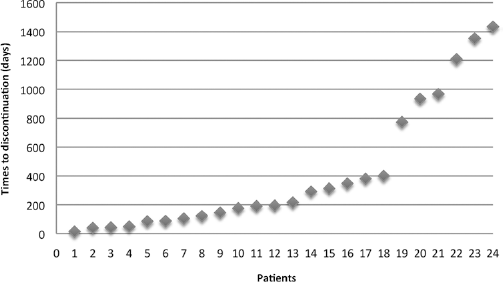
Time to discontinuation of treatment.
In the multivariate logistic regression analysis, age (65 years) and HT were independent factors associated with the onset of arthralgia (p = 0.006 and p = 0.008, respectively; OR 2.65, 95% CI 1.32-5.31). Alternative HT (AI or tamoxifen) was offered to patients who wanted or needed to permanently interrupt the ongoing drug in order to continue adjuvant therapy. Seventeen of 24 patients were switched to exemestane, 5 to tamoxifen, and 1 each to letrozole and anastrozole. In patients who switched to another AI we observed a reduction in the severity of arthralgia but not its complete resolution. Complete resolution of symptoms was observed for the other toxicities except allergic reactions, which recurred after switching from letrozole to anastrozole. Moreover, the patient with the diffuse skin reaction chose discontinuation of HT.
Discussion
Despite the proven benefits of adjuvant HT, patient persistence on and adherence to tamoxifen and AIs are suboptimal. In 503 enrolled women, 32.4% discontinued initial AI therapy within 2 years because of adverse effects; 24.3% discontinued specifically because of musculoskeletal symptoms. Younger age and taxane-based chemotherapy were associated with a higher likelihood of treatment discontinuation (17, 18). In a survey of 622 postmenopausal women, 30% discontinued HT, and 84% did so because of side effects. The most frequently reported reason for changing from an AI to tamoxifen or ceasing to use an AI was arthralgia, although this was frequently reported in combination with other symptoms (19). The intolerance to AIs was evaluated and it was found that after switching from anastrozole therapy to letrozole, 51 patients (28.5%) discontinued treatment due to severe arthralgia (20).
The effects of early discontinuation and non-adherence to HT on mortality were investigated and an unfavorable outcome was reported for early discontinuation as an independent predictor of mortality (21-23). Switching from one AI to another in postmenopausal women with breast cancer who suffer from musculoskeletal adverse events can result in continuation of adjuvant HT (24).
The ATLAS and aTTom trials showed a significant reduction in tumor recurrence and mortality among women who continued adjuvant HT with tamoxifen to 10 years (25, 26). The ASCO guidelines recommended offering women who become definitively postmenopausal the choice of continuing tamoxifen for a total duration of 10 years or switching to an AI for up to 5 years, for a total duration of up to 10 years of adjuvant HT (27). Enhancing the treatment compliance and the adherence to adjuvant HT becomes essential to avoid premature discontinuation. The oncologist should be aware of the time of developing adverse events that could undermine the continuation of treatment. Patients should be advised about the time of onset, the severity of the adverse events, and the consequences of premature treatment interruption. In our analysis 10% of patients discontinued the first AI assigned and 3% interrupted treatment in a definitive way due to toxicity. The onset of toxicity that could potentially lead the patient to request treatment discontinuation is more likely in the first 5 months of treatment (median time course of all adverse events leading to discontinuation: 155 days).
Monitoring the toxicities and the switch to alternative HT is an option that should be offered to patients in order to avoid premature and permanent interruption of an effective treatment. Adequate management of symptoms is fundamental in enhancing patient adherence to treatment.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: The authors declare they have no potential conflicts of interest, including relevant financial interests.