
Abstract
Aims
To evaluate outcomes in patients with sinonasal squamous cell carcinoma (SCC) treated with definitive radiotherapy (DRT) and postoperative radiotherapy (PORT).
Methods
Between 1990 and 2013, 73 patients with sinonasal SCC were treated with radiotherapy. Fifty-two patients (71.2%) were treated with DRT and 21 (28.8%) were treated with PORT. The primary tumor sites were the maxillary sinus in 47 patients (64.4%), the nasal cavity in 18 (24.7%), the ethmoid sinus in 7 (9.6%), and the frontal sinus in 1 (1.4%). Four (5.4%), 11 (15.1%), 24 (32.9%), 17 (23.3%), and 17 (23.3%) patients had T1, T2, T3, T4a, and T4b tumors, respectively. N stage was N0, N1, N2a, N2b, N2c, and N3 in 60 (82.2%), 6 (8.2%), 2 (2.7%), 2 (2.7%), and 3 (4.1%) patients, respectively. The median follow-up period was 23 months (range 3-196).
Results
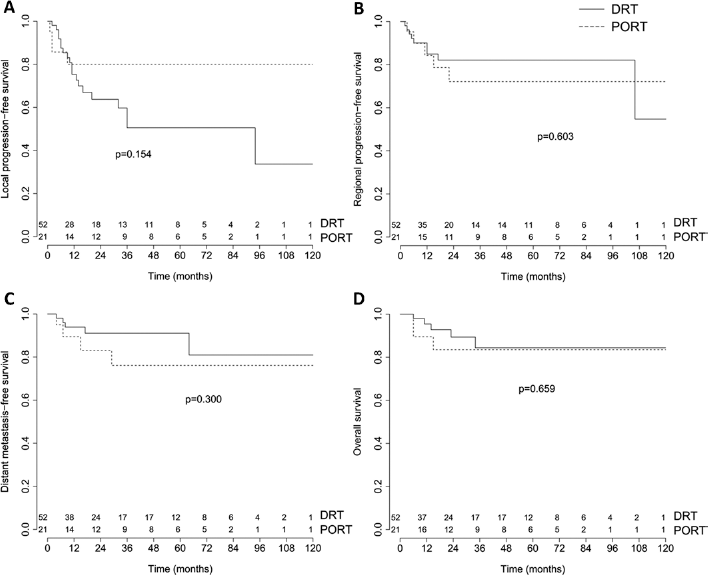
The 5-year local progression-free survival (LPFS), regional progression-free survival (RPFS), distant metastasis-free survival (DMFS), and overall survival (OS) in the DRT and PORT groups were 50.6%, 82.1%, 91.1%, and 84.4% and 85.7%, 72.1%, 76.1%, and 83.5%, respectively, without any statistically significant differences.
Conclusions
The LPFS, RPFS, DMFS, and OS were not significantly different between the DRT and PORT groups. Given the possibility of functional disability and cosmetic disfigurement with facial surgery, DRT might be considered as a surrogate to surgery followed by PORT for patients with locally advanced sinonasal SCC.
Introduction
Malignancies arising from the nasal cavity and paranasal sinuses are relatively uncommon. Age-standardized rates were between 5 and 9 per million for men and between 2 and 5 per million for women worldwide (1). Because these regions are air-filled cavities, symptoms usually do not develop unless the involved sinus is obstructed or the tumor extends beyond the sinus. Therefore, diagnosis of these malignancies is often delayed. In addition to the close proximity of the tumors to critical structures, a high degree of anatomic and histologic variability makes the surgical approach difficult.
Combined modalities consisting of surgery followed by postoperative radiotherapy (PORT) are the mainstay of treatment for sinonasal malignancies. However, there are considerable risks associated with surgical treatment involving these regions, including functional disability and aesthetic disfigurement. Therefore, we have performed definitive radiotherapy (DRT) at our institution for patients who selected radiotherapy (RT) rather than surgery, and for those who were medically inoperable.
The most common malignant histologic type in this region is squamous cell carcinoma (SCC), accounting for 57%-75% (1, 2). Other histologic types (adenoid cystic carcinoma, adenocarcinoma, sarcoma, lymphoma, melanoma) account for 10%-15% of the lesions that arise in this region, each of which is known to have a distinct spread pattern and prognosis. Thus, we aimed to evaluate the clinical outcome in patients with sinonasal SCC treated with DRT and PORT.
Methods
Patient and treatment characteristics
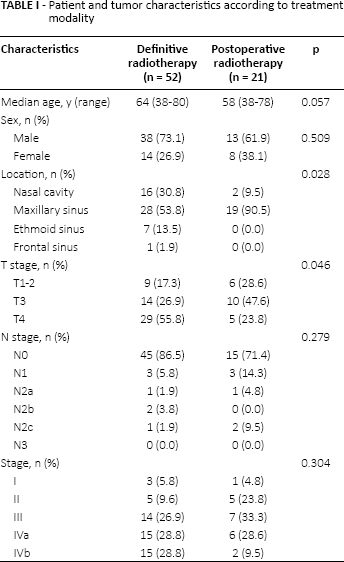
The medical records of patients with pathologically confirmed sinonasal malignancies who underwent RT with a curative intent at our institution between January 1990 and December 2013 were retrospectively reviewed. The institutional review board (IRB) approved this study and provided a waiver of consent (IRB no. 2015-04-042-001). Data for 144 consecutive patients with sinonasal cancer were evaluated, 71 of whom were excluded for the following reasons: palliative intent of treatment (n = 10), salvage intent of treatment (n = 13), or other histology (n = 48). The data for the remaining 73 patients were analyzed. The patient and tumor characteristics are summarized in Table I. There were 51 male and 22 female patients with a median age of 63 years (range 38-80 years). The median follow-up period was 23 months (range 3-196 months). Patients were divided into 2 groups according to the treatment modality. Fifty-two patients were treated with DRT and 21 patients with surgery followed by PORT. For the DRT and PORT groups, the median age of the patients was 64 years (range 38-80 years) and 58 years (range 38-78 years), respectively, which shows a trend toward younger patients being included in the PORT group compared to the DRT group (p = 0.057). T stage was T1, T2, T3, T4a, and T4b in 4, 11, 24, 17, and 17 patients, respectively. Only 13 patients (17.8%) presented with involved cervical lymph nodes, and 6, 2, 2, and 3 patients had stage N1, N2a, N2b, and N2c disease, respectively. DRT patients had more advanced T stage disease than did PORT patients (p = 0.046).
Patient and tumor characteristics according to treatment modality
The characteristics of the treatments are summarized in Table II. Radiotherapy was delivered at doses ranging from 54 to 75.6 Gy (median 72 Gy) in the DRT group. Positive neck nodes were irradiated at the same dose as the primary tumor. In the PORT group, 50 to 75 Gy (median 60 Gy) of RT was delivered to the postoperative tumor bed and involved region of the neck. Elective nodal irradiation (ENI) or elective neck dissection was not performed. All patients were treated with external RT using 6 MV photon beams. Patients treated from 1990-1997 were immobilized with a plaster strip while those treated from 1997-2013 were immobilized with a 5-point thermoplastic head and neck mask with shoulder fixation (Civco Medical Solutions, Kalona, IA, USA). Radiation was delivered once daily, 5 days per week, at 1.8-2.2 Gy per fraction. Patients who received conventional or 3D conformal radiation therapy (CRT) were treated with conventional fractionation of 1.8-2 Gy. A moderate hypofractionated regimen (2.2 Gy per fraction) was used in patients treated with intensity-modulated radiation therapy (IMRT).
Treatment characteristics
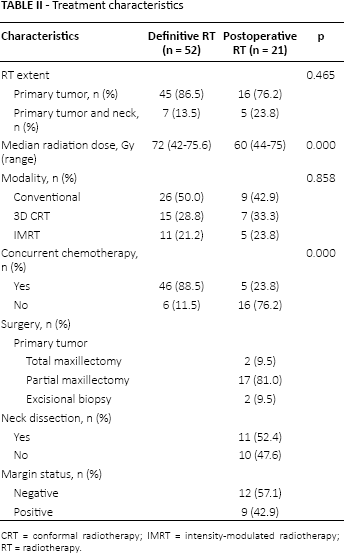
CRT = conformal radiotherapy; IMRT = intensity-modulated radiotherapy; RT = radiotherapy.
Concurrent chemotherapy with radiation was administered to 51 patients (Tab. II). Chemotherapy consisted of cisplatin/capecitabine for 32 patients, cisplatin/5-fluorouracil (5-FU) for 15, cisplatin/TS-1 for 1, cisplatin alone for 1, and capecitabine alone for 2 patients. Cisplatin (60-80 mg/m2) was administered via continuous infusion on the first day of each cycle followed by capecitabine (825 mg/m2 BID), with a rest period between days 15 and 21. The 5-FU was administered via continuous infusion at a dose of 750−1000 mg/m2 for 4-5 consecutive days once a month. Generally, 2 cycles of chemotherapy were repeated every 21 days during RT. Treatment-related toxicities were graded using National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0.
Statistical analysis
All events were measured from the date of surgery for patients treated with PORT or the first day of radiation for those treated with DRT. The actuarial survival rate was calculated using the Kaplan-Meier method, and the differences were compared using log-rank tests. p Values <0.05 were considered significant. Multivariate analysis using the Cox proportional hazard model was performed to identify independent predictors among the various potential prognostic factors. Differences between patient characteristics were analyzed using chi-square tests and independent t tests when appropriate. The R statistical language (version 3.1.3, The R Project) (http://www.R-project.org) was used for all statistical analysis.
Results
Local progression-free survival
Local progression during follow-up occurred in 23 patients (31.5%) (Supplementary Figure; available online at www.tumorijournal.com). The 2- and 5-year local progression-free survival (LPFS) for the entire group of patients was 69.0% and 60.4%, respectively (Fig. 1). In the DRT group, 19 patients (36.5%) had local progression, compared to 4 (19.0%) patients in the PORT group. A higher 5-year LPFS was seen with PORT compared to DRT, although this was not statistically significant (80.0% vs 50.6%, p = 0.154) (Tab. III, Fig. 2A). Positive neck nodes correlated with inferior LPFS relative to node-negative patients on univariate (p<0.001) and multivariate analyses (hazard ratio [HR] 5.77; 95% confidence interval [CI] 2.19-15.19; p<0.001) (Tab. III). Age, tumor location, T stage, RT technique, and the use of chemotherapy did not correlate with LPFS.
Prognostic factors in the univariate analysis
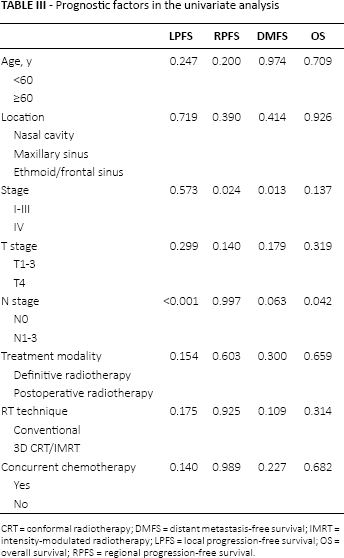
CRT = conformal radiotherapy; DMFS = distant metastasis-free survival; IMRT = intensity-modulated radiotherapy; LPFS = local progression-free survival; OS = overall survival; RPFS = regional progression-free survival.
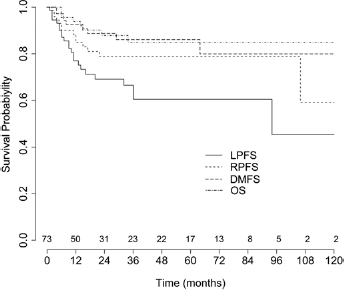
Local progression-free survival (LPFS), regional progression-free survival (RPFS), distant metastasis-free survival (DMFS), and overall survival (OS) for the entire group of patients.
(
Salvage surgery was performed for 6 out of 19 patients with local progression after DRT at a median of 10 months (range 2-93) after RT and 4 were alive at the last follow-up with locally controlled disease at a median of 52.5 months (range 24-106) after salvage surgery. Of the 4 patients who had a local recurrence after PORT, 2 underwent salvage surgery at 9 and 21 months after RT, respectively, and 1 patient was alive at the last follow-up with locally controlled disease 74 months after salvage surgery.
Regional progression-free survival
Regional lymph node failure occurred in 14 patients (19.2%) during follow-up (Fig. 1, supplementary Figure). The 2-and 5-year actuarial regional progression-free survival (RPFS) for the entire group of patients was 78.7% for both time points (Fig. 1). In the DRT group, 9 patients (17.3%) had regional failure compared to 5 patients (23.8%) in the PORT group. The 5-year actuarial RPFS in the DRT and PORT groups were 82.1% and 72.1%, respectively, which was not statistically different (p = 0.603) (Fig. 2). Isolated regional failure occurred in 4 patients in the DRT group and in 2 patients in the PORT group. The 2- and 5-year actuarial isolated RPFS for the entire group of patients was 89.6% at both time points. For the DRT and PORT groups, the 5-year actuarial isolated RPFS was 90.1% and 88.5%, respectively, which were not statistically different (p = 0.603). Of the 13 patients who were initially node-positive (7 in the DRT group and 6 in the PORT group), 11 patients achieved regional control at the time of the last follow-up and 2 (15.4%) developed regional failures, both of whom had in-field failure. Median prescribed doses to the involved neck were 72 Gy (range 69.4-72.6 Gy) and 50 Gy (range 44-75 Gy) in the DRT and PORT group, respectively. Of the 60 patients who were initially node-negative, nodal relapse occurred in 12 patients (20.0%) and isolated nodal relapse occurred in 6 patients (10.0%).
Disease stage was the only factor that significantly influenced RPFS based on the univariate (p = 0.024) and multivariate analyses (HR 4.63; 95% CI 1.23-17.49; p = 0.024) (Tab. III). Tumor location, T stage, N stage, RT technique, and the use of concurrent chemotherapy did not correlate with RPFS.
Salvage treatment was performed in 4 of 14 patients who experienced regional failure. Salvage treatment consisted of concurrent chemoradiotherapy for 2 patients, surgery followed by concurrent chemoradiotherapy for 1, and RT alone for 1 patient. One patient who underwent salvage surgery followed by concurrent chemoradiotherapy was alive without evidence of disease or severe late complications 38 months after salvage treatment. Among the 10 patients who did not receive salvage treatment, 4 patients received palliative chemotherapy because distant metastasis occurred at the same time (supplementary Figure). Two patients refused further salvage therapy and received conservative management only. The other 4 patients were lost to follow-up after the diagnosis of recurrence.
Distant metastasis-free survival
Distant metastasis occurred in 9 patients (12.3%) during follow-up. The 2-year and 5-year actuarial distant metastasis-free survival (DMFS) for the entire group of patients was 86.1% at both time points (Fig. 1, supplementary Figure). In the DRT group, 5 patients (9.6%) developed distant metastasis compared to 4 (19.0%) patients in the PORT group. The 5-year DMFS was 91.1% for the DRT group and 76.1% for the PORT group, but there was no statistically significant difference (p = 0.300) (Fig. 2). Distant metastasis was the first site of failure in 5 patients and a subsequent site in 4 patients. Metastasis to the bones occurred in 5 patients, to the lungs in 4, and to the liver in 2.
Stage IV was the only factor that was significantly associated with worse DMFS on univariate (p = 0.024) and multivariate analyses (HR 12.19; 95% CI 1.47-101.30; p = 0.021) (Tab. III). There was a trend toward a reduction in DMFS in N+ patients on the univariate analysis (p = 0.063). Tumor location, T stage, RT technique, and the use of concurrent chemotherapy with RT did not correlate with DMFS.
Overall survival
During follow-up, 9 patients (12.3%) died: 8 of sinonasal cancer and 1 of non-cancer-related causes (supplementary Figure). The 2-year and 5-year actuarial overall survival (OS) for the entire group of patients was 87.9% and 84.8%, respectively (Fig. 1). The 5-year OS for the DRT and PORT groups was 84.4% and 83.5%, respectively (p = 0.659) (Fig. 2). An inferior OS was observed for patients with N+ disease on univariate (p = 0.042) and multivariate analysis (HR 5.27; 95% CI 1.10-25.13; p = 0.037) (Tab. III). Age, tumor location, T stage, N stage, RT technique, and the use of chemotherapy were not associated with OS.
Treatment-related complications
Acute toxicities were recorded in 40 patients (54.8%). Grade 2 and 3 mucositis was recorded in 22 and 12 patients, respectively. Grade 2 dermatitis was recorded in 3 patients. No patients had grade 4 mucositis. Acute grade 2 conjunctivitis developed in 1 patient. Grade 2 alopecia developed in 1 patient in the treatment field. One treatment-related death was secondary to chemotherapy-induced neutropenia.
Table IV summarizes the incidences of treatment-related late toxicities according to treatment modality. Grade 3 optic neuropathy, retinopathy, and cataract occurred in 1 patient each in the DRT group, all of whom had been treated with conventional RT. Grade 2 nasolacrimal duct obstructions occurred in 6 patients who had undergone dacryocystorhinostomy to alleviate epiphora. One patient in the PORT group developed grade 3 nasolacrimal duct obstruction that required surgical management. Grade 1 dry eye symptoms, requiring treatment with artificial tears, occurred in 3 patients. Grade 3 serous otitis media occurred in 1 patient in the PORT group who was treated with the insertion of a ventilation tube. Grade 3 sensorineural hearing impairment occurred in 1 patient treated with DRT and concurrent cisplatin-based chemotherapy. Speech unintelligibility that required rehabilitation occurred in 1 patient in the PORT group. Three patients had grade 3 trismus. There were no deaths related to radiation side effects.
Late complications
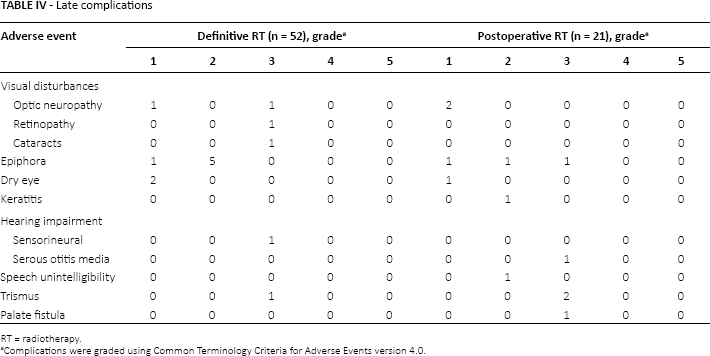
RT = radiotherapy.
Complications were graded using Common Terminology Criteria for Adverse Events version 4.0.
Discussion
The management of sinonasal SCC has been a therapeutic challenge. The current National Comprehensive Cancer Network guidelines for head and neck cancer recommend that patients with T1-T4a maxillary sinus carcinoma undergo complete resection, and when they have adverse features such as a positive margin or extracapsular nodal spread, they should receive PORT (3). For ethmoid sinus carcinoma, though DRT is also a recommended option, surgical resection is the preferred primary therapy. After surgery, PORT is recommended except in cases of low-risk T1 disease.
Several small retrospective trials have suggested that the clinical outcomes achieved with a combined modality treatment of surgery followed by PORT were better than those achieved with either surgery or RT alone. However, to our knowledge, no randomized trial for sinonasal carcinoma has been performed. Furthermore, most previous studies concerning the outcomes of patients treated with DRT were published more than a decade ago, before modern RT techniques were widely used (4–5–6–7–8). Complete resection with an adequate negative margin is often difficult due to advanced stage at diagnosis and the anatomical proximity to critical structures. Despite successful complete resections, most patients experience substantial functional disability or aesthetic disfigurement (9). Therefore, at our institution, DRT with or without chemotherapy has been performed instead of surgery for patients who were reluctant to undergo surgery.
Most previously published series have demonstrated the superior local control of treatment options incorporating surgery. For example, Le et al (5) reported a 5-year local control rate of 20% among patients treated with RT alone and 59% among patients who underwent RT and surgery. Paulino et al (6) also noted improved local control rates with surgery and RT compared to treatment with RT alone. In their study, the 5-year local control rates were 59% for the surgery and RT group and 23% for the RT alone group. Gabriele et al (10) reported a 5-year local control rate of 74% for those treated with surgery and RT versus 20% for those treated with RT alone. Dulguerov et al (7) reported a 40 ± 7% 5-year locoregional control rate in patients treated with RT alone and a 63 ± 4% rate in patients treated with both surgery and RT. Additionally, Katz et al (8) reported a 49% 5-year local control rate for the RT alone group and a 79% rate for the PORT group, which was statistically significant in a univariate analysis (p = 0.05). However, the authors suggested the possibility that the improved results were due to selection bias because the results were not statistically significant in a multivariate analysis. Our results are consistent with those of Katz et al (8). In our study, no statistical difference was found between the DRT and PORT groups for LPFS, although the DRT group had more T4 patients than the PORT group (55.8% vs 23.8%). Of note, the 5-year LPFS of 50.6% in the DRT group suggests that around half of all patients could avoid surgery without local progression.
The lymphatic spread of nasal cavity malignancies is uncommon, although spread to retropharyngeal and cervical chain nodes does occasionally occur. The paranasal sinuses are believed to have little lymphatic supply. Therefore, the rate of lymph node metastasis is relatively low, even in cases of advanced stage disease. Katz et al (8) reported a similar rate of regional failure between patients who received ENI and those who did not. Similarly, Dirix et al (11) reported that only 4 of 127 patients with N0 sinonasal cancers who were treated with RT without ENI developed nodal relapse. Of 4 patients who showed a relapse in regional nodes, successful salvage treatment was possible for 3 patients.
Sakashita et al (12) reported the late neck recurrence rate after DRT in patients with maxillary sinus cancer. According to their data, late neck recurrence was observed in 8.3% of the patients. They concluded that ENI was not required for N0 maxillary sinus carcinomas given that salvage neck dissection surgery was considered feasible for patients with nodal relapse. In our study, the 5-year actuarial isolated RPFS was 89.6%, though ENI had not been performed. Inasmuch as local failure is a major concern, rather than regional failure, the data supporting the performance of ENI appear weak.
Although Amendola et al (4) reported superior OS of patients treated with DRT compared to patients who underwent surgery, most studies thereafter demonstrated improved outcomes after treatments that incorporated surgery (6, 8, 13). The OS rates for patients with sinonasal carcinoma reported in previous series were poor (range 19%-67%) (6–7–8, 11, 14–15–16–17–18–19–20–21). Given that the study by Hoppe et al (20) that showed a 5-year OS of 67% included only patients treated with surgery followed by PORT, the 5-year OS of 80.8% in our study is promising. The salvage treatment protocol at our institution may have contributed to the improvement in survival. Although there is limited literature regarding salvage treatment for patients with progression or recurrence (22), 5 of the 25 patients who had locoregional recurrence achieved locoregional control with salvage treatment in our study.
In recent years, evidence has emerged that the theoretical benefits of IMRT have translated into clinical benefits. Intensity-modulated radiation therapy may result in better sparing of the optic apparatus, especially in cases of tumors that are in close proximity to the orbit. Several dosimetric studies have demonstrated improved dose distributions with the use of IMRT compared to conventional and 3D CRT (23–24–25). In an analysis by the University of California, the incidences of grade ≥3 late ocular toxicity were 20%/9%/0% in patients treated with conventional/3D CRT/IMRT, respectively. In our study, the 2 patients who developed grade 3 optic neuropathy and retinopathy were both treated with conventional RT.
There is no established role for chemotherapy as a part of the combined modality for the management of sinonasal SCC and it has yet to be studied in a large clinical trial. The most common regimen is cisplatin-based. Lee et al (26) suggested that the incorporation of chemotherapy into the management of sinonasal carcinoma resulted in improved outcomes. Several investigators reported a promising response rate with the use of intra-arterial 5-FU chemotherapy in a neoadjuvant setting (27). In our study, concurrent radiosensitizing chemotherapy was administered to most patients (88.5%) in the DRT group and to some patients (23.8%) in the PORT group. A relatively higher 5-year DMFS (91.1%) was observed in the DRT group compared to 76.1% in the PORT group, but these results lacked statistical significance (p = 0.314) (Fig. 2). Although our results, taken together with previous studies, suggest a potential benefit from the addition of chemotherapy, further studies are needed to investigate the role of chemotherapy.
The results presented in our study are limited because of the bias that is inherent to retrospectively designed studies. In addition, the number of patients in the PORT group was too small for a meaningful comparison. Nevertheless, we think our results are valid. While most studies regarding DRT were published before the IMRT era, we included a considerable number of patients in the DRT group who were treated with sophisticated, modern RT techniques such as IMRT. In our study, encouraging 2-year and 5-year OS (87.9% and 84.8%, respectively) rates were observed, even though approximately 50% of the patients had T4 tumors.
In conclusion, although patients treated with DRT had more advanced stage disease, no statistical significance was found between the DRT and PORT groups for LPFS, RPFS, DMFS, and OS. Furthermore, the 5-year actuarial OS rate in our study is promising in comparison to previously published studies. Therefore, in our experience, DRT for sinonasal SCC could be a feasible substitute for surgery followed by PORT if careful patient follow-up and adequate salvage management can be ensured.
Footnotes
Financial support: Kyungpook National University Research Fund, 2012.
Conflict of interest: None.