
Abstract
Purpose
To evaluate the influence of radiation dose on tumor regression grade (TRG) and sphincter preservation rate in a series of cT3N0-1 rectal cancer patients treated with neoadjuvant chemoradiotherapy (CT-RT) with or without a sequential radiation boost.
Materials and methods
Between May 2002 and September 2013, 116 cases were eligible for retrospective evaluation. Radiotherapy was delivered for a total dose of 45 Gy (no boost arm) or 50.4 Gy (boost arm). TRG was evaluated with the Dworak scale.
Results
Median follow-up was 62 months (range, 12-138 months). The 5-year overall survival and local control rates were 72% and 93%, respectively. Fifty-five patients (47%) were treated with a sequential radiation boost and 61 (53%) without a boost. Eighty patients (72%) presented T3N0 disease and 32 (28%) T3N1 disease. Concomitant capecitabine was administered in 92 cases (79%) and intravenous 5-fluorouracil in 24 cases (21%). Sphincter preservation was performed in 82% of patients in the boost arm and 66% in the no-boost arm. A higher TRG was related to a longer interval between neoadjuvant treatment and surgery (p<0.001). The probability of a TRG ≥2 was 2.5 times higher in the boost arm. A gain in local control, estimated at 4% during the first 3 years after CT-RT, favored the boost arm.
Conclusions
The long-term results from our single-center experience confirm literature data on the role of a sequential boost in tumor response after neoadjuvant CT-RT in a series of cT3N0-1 rectal cancer patients.
Introduction
In resectable locally advanced distal rectal cancer, preoperative chemoradiotherapy (CT-RT) and total mesorectal excision are associated with better local control (LC) and a higher rate of sphincter preservation compared to the postoperative approach (1-2-3-4-5-6). In cT3-4 any N, M0 disease, several advantages have been reported with the use of long-course radiation therapy (RT) in tumor downsizing and pathological complete response (pCR) (pCR rates of 13%-36%) (7-8-9). As shown in the EORTC 22921 (10) and FFCD 9203 trials (11), concomitant chemotherapy (fluoropyrimidine-based) was found to provide better outcomes in terms of LC and pCR than RT alone, without any differences in disease-free survival (DFS) and overall survival (OS). Improving the response to preoperative therapy may increase the likelihood of successful resection of locally advanced rectal cancers. A strategy to achieve this result could be to increase the dose to the tumor. This can be performed with an external-beam RT boost (concomitant or sequential) or with a sequential brachytherapy boost (12, 13). According to Wiltshire and colleagues (14), there was a trend toward increased pCR with higher doses. In their experience, a statistically significant increase in local recurrence-free survival, DFS and OS was seen with radiation doses ≥46 Gy.
The aim of the present analysis was to evaluate the influence of RT dose on tumor regression grade (TRG) and sphincter preservation rate in a series of cT3N0-1 rectal cancer patients treated with neoadjuvant CT-RT with or without a sequential radiation boost.
Material and methods
Patient selection
The eligibility criteria of the present retrospective study were age >18 years, a World Health Organization (WHO) performance status of 0-1, cT3N0-1 resectable adenocarcinoma of the rectum (15), located within 10 cm of the anal verge.
Radiation therapy
Prior to neoadjuvant treatment, the stage of disease was assessed by clinical examination, rigid proctoscopy, chest radiography, computed tomography of the abdomen and pelvis, and endorectal ultrasonography. Pelvic magnetic resonance imaging (MRI) was routinely included in the flowchart of disease staging after the results of the MERCURY trial in 2007 (16). All patients underwent computed tomography-based simulation without contrast in the prone position and with a full bladder using a belly board immobilization system. The scan extended from the L2 vertebral body to below the perineum, with 5-mm slices.
Daily patient positioning was performed using skin marks and weekly portal films. The gross tumor volumes (GTV) and clinical target volumes (CTV) were contoured on axial computed tomography scan slices. GTV was defined as the primary tumor (including the mesorectal space around it) and involved lymph nodes. CTV was defined as the primary tumor with the mesorectal and presacral regions, mesorectal lymph nodes, internal iliac lymph nodes, and obturator lymph nodes (17).
The radiation dose was prescribed to the planning target volume (PTV). PTV was created by CTV adding an isotropic 6-mm margin. No study of the small intestine was performed.
Treatment was delivered 5 times a week with a daily fraction of 1.8 Gy for a total dose of 45 Gy. From November 2006, a boost of 5.4 Gy, with a daily fraction of 1.8 Gy, was added to the primary tumor for a total dose of 50.4 Gy, according to an internal protocol and following literature data (5). RT was delivered by photon radiation generated by a 6-MV or greater linear accelerator using 3D conformal RT.
Chemotherapy
Chemotherapy was administered concurrently with RT. Neoadjuvant CT-RT started as soon as possible after diagnosis. In our study population, either of 2 chemotherapy schedules were administered: capecitabine at a dose of 825 mg/m2 twice daily for 5 days/every week during RT, or intravenous bolus injection of 5-fluorouracil at a dose of 1,000 mg/m2/day for 5 days in the first and fifth weeks of RT. No adjuvant systemic therapy was administered.
Surgery and pathology
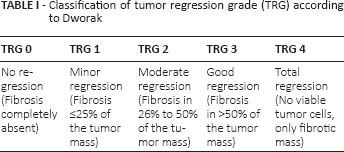
Surgery was scheduled 3 to 10 weeks after the conclusion of CT-RT. Before surgery, all patients underwent reassessment of clinical staging and resectability. The choice between abdominoperineal resection and anterior resection was left to the discretion of the surgeon, although the intent at diagnosis was sphincter preservation. Expert colorectal surgeons performed total mesorectal excision with pelvic autonomic nerve preservation when technically possible. Patients with low rectal cancer (defined as ≤5 cm from the anal verge) undergoing sphincter-preserving surgery also received prophylactic ileostomy to prevent postoperative complications. These patients underwent colonoscopy before ileostomy closure 1 year after surgery. All specimens were grossly assessed for quality by expert pathologists. TRG was evaluated with the Dworak scale (Tab. I).
Classification of tumor regression grade (TRG) according to Dworak
Follow-up and toxicity evaluation
During RT, all patients were examined weekly to evaluate toxicity. Postoperative follow-up was conducted every 3-4 months for the first 2 years after completion of treatment, then every 6 months until the fifth year from diagnosis. Clinical examination, measurement of serum CEA levels, and chest x-ray were performed during each follow-up visit. Abdominal-pelvic computed tomography scan was first done at the sixth postoperative month and yearly thereafter. Patients were assessed for toxicities by the European Organization for Research and Treatment of Cancer (EORTC/RTOG) radiation morbidity scoring criteria. Events occurring within 90 days of the start of RT were defined as acute and those occurring after 90 days as late. Clinical and pathological data were collected and evaluated for statistical analysis.
Statistical analysis
The primary endpoint of the study was the measure of the correlation between RT dose and pathological tumor response. LC, OS and treatment-related toxicity were chosen as secondary endpoints. In order to summarize the most relevant features of the clinical variables, descriptive statistics were performed. Contingency tables with Fisher's exact test, Pearson's chi square test and univariate logistic regression were performed to verify if the following independent factors could influence tumor response in the boost and no-boost groups: interval between CT-RT and surgery (≤4 weeks, 5-6 weeks, 7-8 weeks, 9-10 weeks) and distance from the anal verge (≤5 cm versus >5 cm). Multiple logistic regression analysis was conducted to verify if the RT dose remained a dependent factor in predicting tumor response (i.e., TRG and sphincter preservation). Additionally, statistical analysis was performed in patients with rectal adenocarcinoma ≤5 cm from the anal verge to ascertain whether the boost had a positive effect on sphincter preservation.
Evaluation of the preoperative circumferential resection margin (CRM) was excluded from the analysis because preoperative pelvic MRI was included in disease staging since 2007.
LC and OS were estimated using the Nelson-Aalen cumulative hazard rate function and Kaplan-Meier methods with the log-rank test. LC was defined from the time of diagnosis to the date of locoregional relapse. Any relapse in the pelvis was considered as local recurrence. OS was calculated from the date of diagnosis to the date of death or last follow-up. Time to progression (TTP) was calculated from the date of surgery to the time of recurrence or distant metastasis. A p value <0.05 was considered significant. All statistical analyses were performed using the R-3.1.2 software.
Results
Patients
Between May 2002 and September 2013, 155 consecutive patients with histologically proven cT3N0-1 rectal adenocarcinoma underwent preoperative concomitant CT-RT at our institution. The data of 116 of these 155 patients were evaluated because they met the study's inclusion criteria. The baseline characteristics and demographics are shown in Table II.
Patients’ (n = 116) baseline characteristics and demographics
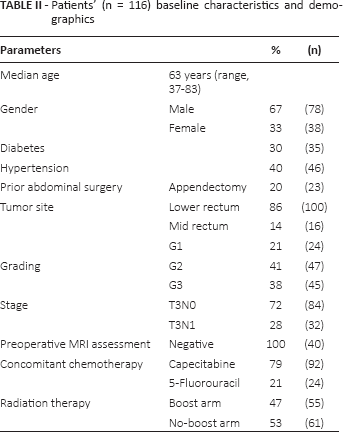
The remaining 39 patients were excluded for the following reasons: 14 because of poor performance status, 4 because of prior pelvic RT, 16 because of acute obstructive symptoms, and 5 because of a history of inflammatory bowel disease.
Correlation between RT dose and TRG
At the pathological examination, TRG was recorded as follows: grade 0 in 15 cases (13%), grade 1 in 25 (21%), grade 2 in 34 (30%), grade 3 in 33 (28%), and grade 4 in 9 (8%). No cases of positive margins were found. TRG ≥2 was reported in 78% of cases in the boost arm and in 60% in the no-boost arm. No significant difference was observed in the pCR (9% in boost arm versus 6% in no-boost arm). At univariate analysis, the probability to obtain a TRG ≥2 was 2.5 times higher in the boost arm than the no-boost arm (p = 0.04).
Type of surgery
Eighty-five patients (73%) underwent anterior resection and the remaining patients underwent abdominoperineal resection. With regard to the 2 groups (boost versus no boost), anterior resection was performed in 82% of cases in the boost arm and 66% of cases in the no-boost arm. Statistical analysis revealed that the possibility to perform an anterior resection was 32 times higher if TRG ≥2 was obtained after neoadjuvant treatment (p<0.001).
Sphincter preservation in patients with low rectal cancer
Before CT-RT, the median tumor distance from the anal verge was 6 cm (range, 4-10 cm). No evidence of anorectal ring infiltration was reported at rigid proctoscopy. At univariate analysis, no statistical significance was found between anal verge distance (≤5 cm versus >5 cm) and tumor response (p = 0.2). Instead, when we analyzed patients suffering from low rectal adenocarcinoma (<5 cm), we found a statistical correlation in favor of sphincter preservation in the boost arm compared with the no-boost arm (p = 0.04).
Correlation between the interval between RT and surgery and TRG
The interval from the end of CT-RT to surgery was ≤4 weeks in 18 patients (15%), 5-6 weeks in 37 (32%), 7-8 weeks in 32 (28%), and 9-10 weeks in 29 patients (25%).
At multivariate analysis, a greater TRG was related to a longer interval between neoadjuvant treatment and surgery (p<0.001). In detail, in 92% of cases a TRG 0-1 was recorded if time to surgery was ≤4 weeks, while in 89% of cases a TRG 2-3-4 (fibrosis >50%) was registered if time to surgery was 9-10 weeks. A higher pCR was found if the time to surgery was 9-10 weeks. As shown in Figure 1, the probability to obtain a greater TRG gradually increased until a plateau phase 7-10 weeks after CT-RT for both groups (boost and no boost).
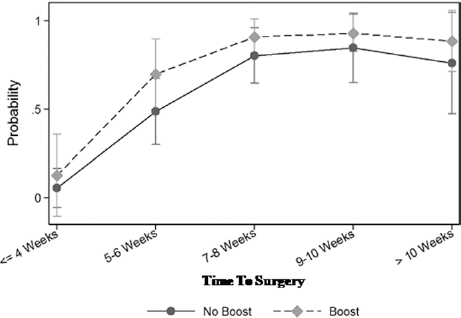
Adjusted predictions model: the probability to obtain a greater tumor regression grade gradually increased until a plateau was reached 7-10 weeks after chemoradiotherapy in both groups (boost and no boost).
Clinical outcomes
At the time of the analysis, median follow-up was 62 months (range, 12-138 months). The 5-year OS rate was 72%. Thirty-four (28%) cancer-related deaths were registered. A trend towards a gain in OS was observed for T3N0 versus T3N1 disease (p = 0.06). Instead, no difference in OS was reported between the 2 groups (boost versus no boost) considering 1) the whole study population; 2) the subanalysis for T3N0 and T3N1 disease (Fig. 2).
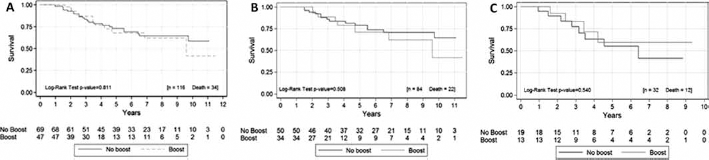
Kaplan-Meier overall survival curves in the boost and no-boost arms for the overall study population (
The 5-year LC rate was 93%. Eight patients (7%) experienced locoregional failure. Thirty-four patients (29%) had systemic progression of disease (14 lung, 12 liver, 4 lymph nodes, 3 brain, 1 bone). The median TTP was 51 months (range, 12-130 months).
Cumulative hazard estimate analysis showed a gain in LC of 4% in favor of the boost arm during the first 3 years after CT-RT, reaching a plateau in the third year. In case of T3N0, a 2-fold risk of local recurrence in the no-boost arm was observed (p = 0.04), with a similar time trend. No significant difference was reported for T3N1 disease.
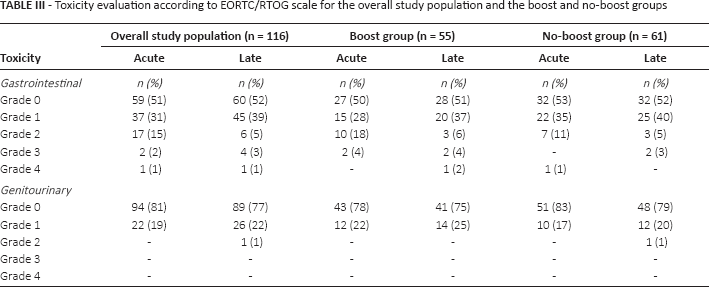
Toxicity was recorded in all patients. The late toxicity profiles were slightly different in the 2 groups. In particular, a higher rate of fecal incontinence was recorded in the boost arm (5 cases versus 2 cases in the no-boost arm). The gastrointestinal and genitourinary toxicities are detailed in Table III.
Toxicity evaluation according to EORTC/RTOG scale for the overall study population and the boost and no-boost groups
Discussion
In resectable locally advanced rectal cancer, the multidisciplinary treatment approach is considered the standard of care (18). The importance of preoperative RT to optimize clinical outcomes has been well reported by various randomized trials (4, 11, 12, 19). Although RT has made significant progress in terms of technology and therapeutic indications, the analysis reported here focused on the long-term findings in a historical series treated with standard 3D conformal RT. Compared with the postoperative approach, neoadjuvant treatment was associated with a higher LC rate, lower gastrointestinal toxicity, and increased sphincter preservation (5). In the present study we found a 5-year local recurrence rate of 7%, which is comparable to the EORTC 22921 findings, where the 5-year local recurrence rate was 8.5% (10). Although the pathological features influencing LC in rectal cancer, such as ypN stage and lymphatic invasion (20), are not listed in the present study, an interesting result was noted when we analyzed LC in the 2 arms (boost versus no boost). In fact, a 4% gain in LC was observed during the first 3 years in favor of the boost group, reaching a plateau in the third year. There was no difference in OS between the 2 groups. In addition, other data emerged in favor of the boost group. TRG, a surrogate marker to monitor the local effectiveness of neoadjuvant treatment (21-22-23), was higher in patients treated with a boost (TRG ≥2 was 78% in the boost arm versus 60% in the no-boost arm), even if pCR seemed to be not strictly dependent on the boost (9% boost versus 6% no boost). In a randomized trial where 2 radiation doses were compared (12), the higher tumor dose increased the rate of major response by 50% in cT3 rectal cancer. Additionally, it has been documented that TRG could be a time-dependent phenomenon (4, 24). A limitation of the present analysis was the heterogeneity of surgical timing, which ranged from 3 to 10 weeks after the conclusion of CT-RT. Moreover, the long-term findings of the current single-center experience confirm the importance of prolonging the interval between neoadjuvant treatment and surgery. In fact, the probability to obtain a greater TRG gradually increased until a plateau was reached 7-10 weeks after CT-RT in both groups (boost and no boost). Although some authors have recently suggested that prolonging the interval between neoadjuvant treatment and surgery could potentially increase TRG and the rate of sphincter preservation (4, 20), many surgeons hesitate to delay surgery beyond 6 weeks due to the expected radiation-induced pelvic fibrosis and consequent surgical complications (4). Other factors, including the surgeon's expertise as well as patient-related factors, may also influence the sphincter preservation rate (25). In a Polish trial (26), patients with locally advanced rectal cancer were submitted to preoperative combined-modality therapy (50.4 Gy plus bolus 5-FU/leucovorin) followed by surgery (median interval >10 weeks). Sphincter preservation was accomplished in 58% of the cases. In the boost arm of the present study, where a similar radiation dose was delivered, anterior resection was performed in 82% of cases. This difference could be attributable not only to surgeon expertise but probably also to the timing of surgery. In fact, in the current analysis the plateau of the tumor shrinkage effect was approximately 8 weeks after CT-RT. These findings might indicate that there may be a detrimental effect on tumor clearance and thus on surgical outcome if the time to surgery exceeds the tenth week after CT-RT.
Finally, in contrast to the M.D. Anderson Cancer Center experience (27) where significant tumor downsizing was obtained with preoperative CT-RT, allowing sphincter-sparing surgery in over 40% of patients when tumors were located <6 cm from the anal verge, in our series no statistical correlation was found between anal verge distance (≤5 cm versus ≥5 cm) and sphincter preservation.
The present analysis presents several limitations, including the retrospective nature of the analysis and the lack of homogeneous MRI assessment and preoperative definition of CRM. In fact, in the recent 5-year update of the MERCURY trial (28), preoperative MRI assessment of CRM status was defined superior to AJCC TNM-based criteria for assessing the risk of local recurrence, DFS and OS. However, as mentioned before, pelvic MRI was included routinely for rectal cancer staging in our institution since the publication of the MERCURY trial in 2007 (16).
A criticism regarding outcome interpretation, as a possible confounding factor, could be related to the 2 chemotherapy schedules administered. However, several randomized trials have established that capecitabine is comparable to intravenous 5-FU in the neoadjuvant setting (29, 30). Another concern regards the usefulness of adjuvant chemotherapy in case of a limited pathological response. No adjuvant systemic therapy was administered in our series. Nevertheless, no consensus has been reached for confirmed ypT3N0-1 rectal cancer following preoperative CT-RT (31). In fact, the 2 main randomized trials in this setting failed to find any improvement in OS (11, 32).
In conclusion, despite possible criticism at the present analysis for its retrospective nature, the long-term findings of our single-center experience seem to confirm the potential role of a sequential boost in LC, tumor shrinkage and sphincter preservation in a series of T3N0-1 rectal cancer patients.
Footnotes
Abbreviations
Financial support: None.
Conflict of interest: The authors have no conflict of interest to declare.