
Abstract
The therapeutic approach to thyroid carcinoma usually involves surgery as initial treatment. The use of external beam radiotherapy (EBRT) is limited to high-risk patients and depends on clinical stage and histologic type. Different behavior patterns and degrees of aggressiveness of thyroid carcinomas require different management for differentiated, medullary, and anaplastic carcinoma. However, the role of EBRT is an issue of debate. Most clinical studies are retrospective and based on single-institution experiences. In this article, we review the main literature and give recommendations for the use of EBRT in thyroid carcinoma on behalf of the “Radioterapia Metabolica” Group of the Italian Radiation Oncology Association.
Introduction
The therapeutic approach to thyroid carcinoma (TC) usually involves surgery as initial treatment. The use of external beam radiotherapy (EBRT) is limited to high-risk patients and depends on clinical stage and histologic type. Differentiated thyroid carcinoma (DTC) includes papillary, follicular, and Hürtle carcinomas, which account for about 80%, 11%, and 3% of all TC, and have 10-year survival rates of 93%, 85%, and 76%, respectively (1). Medullary thyroid carcinoma (MTC) accounts for 5% to 10% of all TC (2, 3). The overall survival of patients with MTC is 86% at 5 years and 65% at 10 years (4). Anaplastic thyroid carcinoma (ATC) is a rare and aggressive disease representing less than 2% of all TC, with a median survival of 5 months and a 1-year survival rate of 20% (5, 6). The different behavior patterns and degrees of aggressiveness of DTC, MTC, and ATC require different management strategies. The role of EBRT is an issue of debate. Most clinical studies are retrospective and based on single-institution experiences. In this article, we review the main literature and give recommendations on the use of EBRT.
Clinical studies
Differentiated thyroid carcinoma
A randomized clinical trial evaluating the clinical benefit of EBRT for locally advanced DTC failed to show any benefit of adjuvant EBRT (7). The difference in recurrence rates between the irradiated and the control arm was not statistically significant. However, this study had several limitations, most notably a poor accrual, and a set of selection criteria that included patients with extrathyroid extension. The control arm reported a low recurrence rate, which was probably due to the lack of high-risk patients. To date, there are no known randomized control studies on adjuvant EBRT in DTC; however, there are several retrospective single-institution experiences that suggest a better locoregional (LR) control rate with EBRT in high-risk patients. In a study from the Memorial Sloan Kettering Center (MSKCC) on high-risk DTC, the 4-year LR progression-free survival (PFS) was 72% with a mean radiation dose of 62 Gy. Significant toxicities were reported, with 5% feeding tube dependence (8). An MD Anderson Cancer Center (Houston, Texas) review reported a LR PFS of 79% at 4 years; 96% of patients had extrathyroid extension and the use of intensity-modulated radiation therapy (IMRT) was associated with less late toxicity (9). Romesser et al (10) observed in non-ATC patients treated with EBRT that poor DTC had significantly improved LR PFS at 3 years compared with well/moderate DTC (89.4% vs 66.1%). There was no difference in LR PFS between gross residual and unresectable disease. Kim et al (11) analyzed the effect of EBRT volume on LR PFS in LR advanced or recurrent non-ATC treated with EBRT. They found a significantly higher LR PFS at 5 years in patients irradiated on the primary or recurrent tumor bed and on the regional nodal areas in the cervical neck and upper mediastinum (89%) compared with patients irradiated on the primary or recurrent tumor bed and on the positive nodal area (40%). There were no significant differences in the incidence of toxicities. A recent retrospective study evaluated the outcome of metastatic follicular TC. Use of EBRT on metastasis did not impact cause-specific survival (12).
Medullary thyroid carcinoma
The role of EBRT in MTC is less clear than in DTC. The analysis of the Surveillance Epidemiology and End Results on patients who underwent total thyroidectomy and lymph node dissection for MTC showed no survival benefit of adjuvant EBRT in patients with positive nodes (13). Some retrospective studies have shown an improvement in LR PFS in high-risk patients, but no benefit in survival. Fife et al (14) reported in a cohort of 51 patients a 5-year LR PFS of 100% in patients with negative margins, 65% in patients with microscopically positive margins, and 24% in patients with gross residual disease. Call et al (15) reported a retrospective review of MTC treated with adjuvant or palliative EBRT. The authors observed that EBRT may provide sustained control of advanced or metastatic disease and that adjuvant EBRT may be effective for the prevention of LR recurrence. Brierley et al (16) reported that patients at high risk of LR recurrence (gross or microscopic residual disease, extraglandular spread, or nodal disease) had a higher LR PFS when treated with EBRT (86% vs 52% at 10 years). A study from the MD Anderson Cancer Center in 34 patients with stage IVA to IVC MTC showed a LR PFS of 87% at 5 years with a median EBRT dose of 60 Gy (17).
Anaplastic thyroid carcinoma
Out of 2,742 patients with locally advanced disease (stage IVB), an improvement in overall survival was observed in patients treated with adjuvant EBRT or concurrent radiochemotherapy vs surgery alone (6, 10, and 2 months, respectively); the difference was not significant (18). Levendag et al (19) reported in patients treated with EBRT a median survival of 3.3 months with doses >30 Gy, vs 0.6 months with doses <30 Gy. In a review by the MSKCC, the radiation dose (<60 Gy vs ≥60 Gy) was found to be a significant prognostic variable for overall survival in multivariate analysis (20). Wang et al (21) reported a significantly higher PFS in patients treated with radical vs palliative EBRT (11.1 months vs 3.2 months). They also observed a trend for increased median survival with twice daily EBRT (60 Gy in 40 fractions delivered in 1.5 Gy per fraction, with 2 fractions per day), which was not statistically significant.
Treatment recommendations
Differentiated thyroid carcinoma
Use of EBRT to the neck for TC is infrequent (22). In patients with locally advanced disease, there are reports of responses and of improved disease-free and cause-specific survival. However, the studies published so far are affected by the inherent bias of retrospective series, with mixed patient populations and histologic subtypes, treated over long periods of time during which there were variations in therapy and changes in staging systems (23). Only 1 phase II clinical trial was published, which involved 201 patients with locally advanced papillary TC (24). In this study, LR PFS at 4 years was significantly higher in the EBRT compared with the non-EBRT group (100% vs 84.6%, p = 0.002). Intensity-modulated radiation therapy was well-tolerated with no grade 3 or higher toxicities.
The principal international guidelines (22, 23, 25-26-27) agree that adjuvant EBRT should be considered in the following settings: 1) locally advanced disease with extrathyroid extension at the time of surgery; 2) gross residual disease; and 3) recurrent tumors that fail to concentrate radioactive iodine (RAI) and in which additional surgery would most likely be ineffective. In fact, in patients with gross residual or unresectable disease, EBRT is a safe and effective treatment modality with greater than 85% LR control in patients with nonmetastatic disease and 90% LR control in patients treated with concurrent radiochemotherapy (10). There are reports of improved relapse-free survival in patients over 60 years of age with extrathyroid extension and no gross residual disease (26, 28). We recommend EBRT also in patients, usually over age 50 years, with gross extrathyroid extension infiltrating the trachea or the esophagus, which is unlikely to be controlled by RAI, and in whom salvage surgery may require laryngectomy or esophagectomy (T4a or T4b) (29). External beam radiotherapy using modern techniques such as IMRT and stereotactic radiotherapy can be used for LR nonresectable recurrence or for extranodal extension or involvement of soft tissues (26). When surgical excision of recurrent disease is not feasible, EBRT may be useful. In such situations, molecular therapies, especially those targeting key tyrosine kinases and/or inhibiting angiogenesis, are the newly emerging treatment modalities (30). The lack of radioiodine uptake is associated with a worse prognosis. Fewer Hürthle cell carcinomas concentrate 131I in comparison with papillary and follicular carcinomas. In 101 patients with distant metastases, 131I uptake by pulmonary metastases was observed in 64% of follicular and 60% of papillary carcinoma but in only 36% of Hürthle cell carcinomas (31). The use of EBRT in such cases is controversial (1). Schwartz et al (9) suggest that tall cell, Hürthle, clear cell variants, and poor DTC should undergo irradiation; conversely, in the study by Kazaure et al (32), patients with these aggressive variants who received EBRT did not experience any improvement in survival. The indications for primary EBRT are rare and fall into the palliative intent. External beam radiotherapy can play a role in palliation of symptoms both in unresectable disease in the thyroid bed or in the neck and in distant metastasis (bone, lung, brain) (25, 26). As for the treatment of metastatic disease, the American Thyroid Association (ATA) recommends that EBRT should be used in the management of unresectable gross residual or recurrent cervical disease, painful bone metastases, or metastatic lesions in critical locations, not amenable to surgery, and that are likely to result in fractures, or neurologic and compressive symptoms (25, 26).
Medullary thyroid carcinoma
Unlike DTC, RAI is not a viable option in the treatment of MTC (23). In the past, in mixed medullary DTC, the possibility was considered that RAI uptake in follicular cells might damage adjacent MTC cells (33, 34). However, in a recent study on 293 patients treated by total thyroidectomy for MTC, there was no difference in disease-free survival between the treated and untreated group (35). In addition, according to the most recent ATA revised guidelines, postoperative RAI is not indicated following thyroidectomy for MTC (36). The first task of surgery in the neck is to preserve speech, swallowing, parathyroid function, and shoulder mobility and to prevent iatrogenic injuries. Therefore, EBRT and medical treatment appear to be the most suitable treatments in case of extensive local or metastatic disease. Generally, due to the lack of randomized trials, EBRT has been reserved for selected patients with a high likelihood of tumor recurrence following thyroidectomy, as determined by the operating surgeon and the radiation oncologist (36). It is important to note that the 5-year rate of local control without EBRT is 100% in patients without residual disease, 65% in those with microscopic residual disease, and 24% in those with gross residual disease (14). Therefore, patients with high-risk features (such as extensive metastatic lymph nodes or extrathyroid extension, gross residual disease, and microscopically positive surgical margins) should be considered for adjuvant EBRT (15). Schwartz et al (9) documented durable LR disease control with relatively limited morbidity in patients with advanced-stage disease treated with modern EBRT. Moreover, patients with locally advanced or metastatic MTC frequently enjoy durable overall survival, making optimal LR management an imperative. International guidelines agree to recommend EBRT in patients with high risk of recurrence (i.e., microscopic or macroscopic residual MTC, extrathyroid extension, extensive lymph node metastases, or lymph nodes with extranodal soft tissue extension) (27, 36), carefully considering the potential benefits against the acute and chronic toxicity associated with the therapy. Patients with metastatic disease causing symptoms should be considered for palliative EBRT (15). For the following indications of palliative EBRT, we refer to ATA revised guidelines of 2015 (36):
Brain metastases: stereotactic radiotherapy has a role in the management of isolated brain metastases. Whole-brain EBRT is indicated for multiple brain metastases.
Bone metastases: almost 70% of patients treated with EBRT had significant pain reduction lasting for months (37).
Lung and mediastinal metastases: EBRT has a role in the treatment of lung and mediastinal metastases even if lung metastases are generally multiple.
Hepatic metastases: EBRT is not indicated in the management of hepatic metastases, which occur in 45% of patients with advanced stage MTC.
Cutaneous metastases: Patients with MTC rarely develop cutaneous metastases. Skin metastases tend to respond to treatment with EBRT, but prognosis is very poor (38).
Palliation of advanced MTC: Palliative therapy, including surgery, EBRT, or systemic therapy, should be considered in patients with metastases causing pain, mechanical compression, or signs and symptoms of hormonal excess.
Anaplastic thyroid carcinoma
No prospective randomized controlled trials have been undertaken. There is no consensus on optimal management of small intrathyroidal ATC or incidentally found ATC following surgery. In such cases personalized decision-making is recommended (23). After complete or near-complete resections, the best results in terms of both local control and survival, according to several studies, appear to be achieved with the combination of surgery, EBRT, and chemotherapy. Kebebew et al (39) examined 516 patients retrospectively and identified age below 60 years, the extent of disease, and the association of surgery and EBRT as positive prognostic factors in multivariate analysis. Best results are reported after maximum surgical debulking and postoperative concurrent chemoradiotherapy, even if the results in terms of operability, according to Brignardello et al (40), are scarce. In contrast, Busnardo et al (41) reported that preoperative chemoradiation improves operability. Moreover, in the management of unresectable ATC, the EBRT maintains a key role (1). More prospective studies on this topic are needed. Therefore, the American (5) and British (23) Guidelines recommend that, following an R0 or R1 resection (excluding an incidental intrathyroidal microscopic lesion), patients with no evidence of metastatic disease should be offered definitive EBRT (with or without concurrent chemotherapy). In unresectable localized disease, EBRT can achieve long-term local control. A recent study (42) reported that a higher dose allowed to bring a neck mass under control in 10/13 patients. A good LR control (including complete and partial response and stable disease) avoids tracheostomy due to breathing difficulties. Several researchers report a better response with higher radiation doses; however, these data need to be evaluated carefully since all these studies are retrospective and patients with less extensive disease and better performance status are more likely to be given high-dose radiation therapy (6). Surgical resection may be reconsidered when radiation renders the tumor potentially resectable. IMRT is indicated for the delivery of a more conformal and hence higher dose with improved dose homogeneity across both gross disease and high-risk areas. For selected patients with pain and obstructive symptoms, a palliative EBRT could be considered. External beam radiotherapy may also be considered for palliation of symptomatic distant metastases. Key recommendations are summarized in Table I.
Treatment recommendations
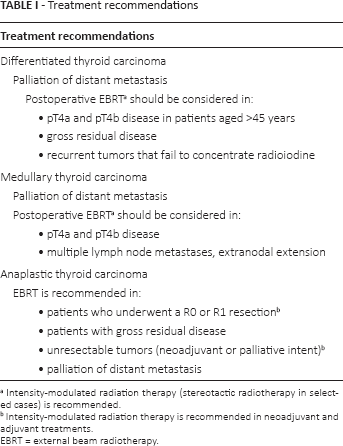
Intensity-modulated radiation therapy (stereotactic radiotherapy in selected cases) is recommended.
Intensity-modulated radiation therapy is recommended in neoadjuvant and adjuvant treatments.
EBRT = external beam radiotherapy.
Timing of EBRT
In DTC, there are no clinical studies aiming to define the optimal timing of EBRT and RAI. The ATA guidelines recommend planning the sequence of EBRT and RAI on the basis of the volume of gross residual disease and the likelihood of the tumor being RAI responsive (25). In MTC, there are no clear data about the role and timing of postoperative EBRT. Regarding ATC, a recent review including a total of 1,352 patients compared the outcome with preoperative vs postoperative EBRT. Patients receiving radiation prior to surgery were associated with a significantly lower cause-specific survival compared to patients receiving radiation postoperatively (median 9 months vs 51.0 months, respectively, p<0.0001) (43). The ATA guidelines recommend starting EBRT as soon as feasible, since ATC has very rapid growth. Radiation treatment should begin as soon as the postoperative swelling has subsided, approximately 2 to 3 weeks after surgery (6).
Clinical target volumes
Differentiated thyroid carcinoma
External beam radiotherapy of the neck is always critical: minimizing treatment volumes can reduce early and late toxicity but may compromise LR control of disease (44).
In a study published in 2008, Azrif et al (45) followed 49 patients treated for DTC and found that the majority of recurrences in TC are LR in the lateral neck and thyroid bed. Based on the data reported in the literature, guidelines, and our institutional practice, we recommend the following policy:
Clinical target volume (CTV) 1: high-risk areas: the operative or tumor bed, operative thyroid gland volume, and central nodal compartment, areas of microscopic disease, close or microscopically positive margins, and areas of gross disease, including nodal areas of extracapsular extension;
CTV 2: moderate-risk areas: clear surgical bed or positive nodal areas in absence of extracapsular extension;
CTV 3: low-risk areas: cervical lymph node levels II-VI, ipsilateral to the lesion, adjacent to CTV 2. In selected patients, level II can be excluded from the CTV, to minimize the risk of acute and late toxicity to the parotid gland;
CTV 4: volume of elective nodal station involvement other than CTV 3 (levels II-VII): in consideration of the presence of few cases of mediastinal recurrences confined to the superior mediastinum (45), we recommend to treat level VII. The volumes extend from the hyoid bone superiorly to the aortic arch inferiorly.
As EBRT techniques are constantly evolving and become more conformal with the increasing use of IMRT, whereby sharp dose gradients exist between the target and adjacent normal tissue, accurate contouring of tumor targets is very important in order to achieve cure and LR control; 18F-FDG- positron emission tomography (PET) can provide more accurate target identification (46). It is well-known that many malignancies have higher metabolism and consequently an increased uptake of FDG than surrounding normal tissues. This allows FDG-PET to image them (47). The FDG uptake correlates with outcome in head and neck cancer patients and the majority of LR recurrences occur within FDG-avid areas (48), which would represent a reasonable target for focal dose escalation (49). Even if there is no experience reported in the literature in the treatment of TC, we recommend that the gross tumor volume should be defined by fusion of images from computed tomography simulation and 18F-FDG-PET. All targets should be contoured with additional circumferential margins of at least 3-5 mm, to accommodate daily uncertainty, and they are defined as planning target volume (PTV). Except in case of extracapsular extension or gross residual tumor (R2), the skin should be spared at least 3-5 mm from all PTVs and the esophagus at least 3-5 mm from PTV1 and PTV2.
Medullary thyroid carcinoma
Regarding the individuation of CTV in the EBRT of MTC, we recommend following the same indications we reported for DTC.
Anaplastic thyroid carcinoma
As for the individuation of CTV in the EBRT of ATC, we recommend following the same indications we reported for DTC.
Radiation techniques, field design, dose prescription, and simulation
Historically, research articles on EBRT for TC have reported results with bidimensional irradiation. From the 1990s, tridimensional/conformal EBRT replaced bidimensional EBRT, and the latter has now been replaced by IMRT (ICRU 83) (44). Intensity-modulated radiation therapy allows for dose escalation with better tissue tolerance. Highly conformed dose distribution allows an individual dose adaptation even to extremely irregular thyroid tumor contours as well as to decrease the radiation dose delivered to organs at risk (9, 50, 51). Khalifa et al (52) compared dose distribution obtained with helical tomotherapy and volumetric modulated arc therapy; both techniques provided attractive treatment plans, with helical tomotherapy providing better medullary canal sparing. Due to the complex head and neck anatomic region with multiple organs at risk, which have to be spared, a modern treatment for TC has to be performed only with advanced techniques, namely IMRT or 3D CRT with multiple fields.
Differentiated thyroid carcinoma
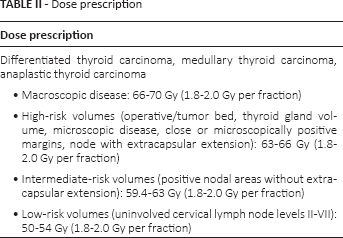
In the setting of postoperative treatment for well DTC, a significant dose-effect correlation has been suggested with an increase in local control for patients receiving >50-54 Gy (53). Little information can be found in the literature regarding the volumes that should be irradiated: comparing the effect of limited fields (62.5-67.7 Gy to the primary or recurrent tumor bed and positive nodal area) and elective fields (60-69 Gy to tumor bed and positive nodal area; 50 Gy to regional nodal area in the neck and upper mediastinum), significantly better LR control using elective fields was reported (11). According to the elective field strategy, a 50-54 Gy CTV should include a large volume comprising the former primary tumor and regional cervical lymph nodes (levels III-IV and VI, partial V, sometimes level II) and the lymph nodes of the superior mediastinum (level VII). Because of the different types of tumor cell spread, the upper cervical lymph drainage (level II) can be spared, especially in node-negative follicular cancer. Tumor bed, tracheoesophageal grooves, and central nodal compartment (level VI), may be irradiated to 59.4-63 Gy, thus reducing the risk of permanent xerostomia. Intermediate risk CTV, including the operative high-risk CTV, defined by close or microscopically positive margins (R1), should receive 63-66 Gy, while areas of residual macroscopic tumor (R2) or recurrent unresectable disease should be treated up to 70 Gy (1, 10, 54). The conventional fractionation schedule of 1.8-2.0 Gy/d/5 times a week is indicated in slow growing tumors and for patients with a high probability of cure.
Medullary thyroid carcinoma
The benefit of EBRT in MTC is more questionable than in DTC. No prospective randomized clinical trials have been conducted in order to assess a possible survival benefit of EBRT but results from retrospective series suggest an improvement in LR control with postoperative EBRT (15, 17). Because of the capacity of MTC to spread early to the cervical and mediastinal lymph nodes, large fields are commonly used in the adjuvant postoperative setting, with the 50-54 Gy CTV including the area of the former primary and the whole thyroidal bed as well as the regional cervical and upper mediastinal lymph nodes (levels III-IV, VI-VII, sometimes II), depending on the distribution of lymph node metastases and the extent of surgical resection. When cervical lymph nodes are extensively infiltrated, the target volumes may be treated up to 60 Gy. In areas of incomplete resection or for inoperable tumors, a dose escalation up to 70 Gy is indicated (36, 55).
Anaplastic thyroid carcinoma
For ATC, results of conventional fractionated EBRT are poor. Hyperfractionated and accelerated schedules have been used, sometimes within a sequence of resection and chemotherapy, in a concomitant or exclusive setting even within preoperative protocols (56-57-58-59). Although local control may be improved, reported results are inhomogeneous and long-lasting overall survival is rare. Extremely aggressive radiation protocols (2 Gy 2/d or 4 Gy/d) can impair improvement of local tumor control by extensive side effects with unacceptable toxicity and should be avoided. In patients with good performance status, in the absence of metastatic disease, either standard fractionation (1.8-2.0 Gy/d, 5 times a week) or accelerated hyperfractionated (1.5-1.6 Gy /2/d, 5 times a week) schedules should be used. Total doses of about 50-60 Gy are needed to treat the thyroid volume and all involved regional nodes in this setting of a rapidly infiltrating type of tumor. For palliation in patients with poor performance status, as an alternative to the classic fractionation scheme of 3 Gy/d, 5 times a week for 2 weeks, a more hypofractionated schedule can be used: 4 Gy/d, 5 times a week for 1 week with the option of a second course of irradiation 2-4 weeks after (21). Simulation has to be performed using a large plastic mask, in order to immobilize the head, neck, and shoulders of the patient. Computed tomography scans every 2 millimeters are preferred in order to obtain more detailed images. Accurate contouring of all organs at risk and the definition of appropriate tune volumes allow the request of relative constraints for IMRT planning. An example of dose distribution with static IMRT is shown in Figure 1. Key recommendations are summarized in Table II.
Dose prescription
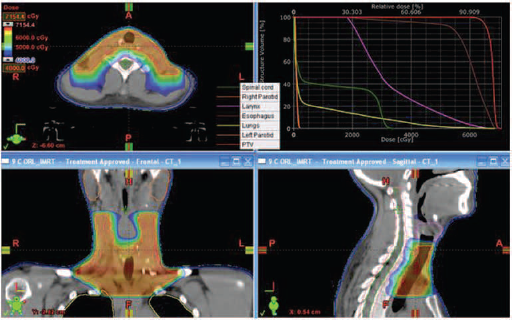
Example of dose distribution with static intensity-modulated radiation therapy.
Definition of at-risk organs and dose limitations
Due to the close proximity of the thyroid bed to critical organs, EBRT can cause several complications and it can be difficult to plan. In fact, cases of III and IV grade acute and chronic toxicity have been reported. The experience of the MSKCC reported acute grade 3 mucositis in 18% and dysphagia in 32% of patients. Moreover, in this experience 29% of patients had a short-term percutaneous endoscopic gastrostomy tube and 5% required enteral feeding for long-term support (8). In the randomized German trial, 1 patient had tracheostomy for chronic laryngeal edema (7). In another experience, the MD Anderson Cancer Center group reports that in patients treated prior to the advent of IMRT, 12% had late toxicity and 9% required dilation for esophageal stricture, while with IMRT only 2% of patients had late morbidity of equivalent severity (17). This means that with improvements in radiation techniques, an adequate dose can be effectively delivered to the region at risk while minimizing the dose to surrounding critical area (8, 25, 51, 60, 61). Intensity-modulated radiation therapy has replaced tridimensional/conformal EBRT, improving PTV coverage with less morbidity but with no impact on survival outcomes (52, 62-63-64).
The thyroid gland lies anteriorly in the low neck and has multiple bilateral lymphatic cervical and mediastinal drainages that constitute potential target volumes around the organs at risk such as medullary canal, mandible, salivary glands, larynx, oral cavity, esophagus, and brachial plexus. Dose constraints are shown in Table III (65).
Dose constraints in thyroid external beam radiotherapy (65)
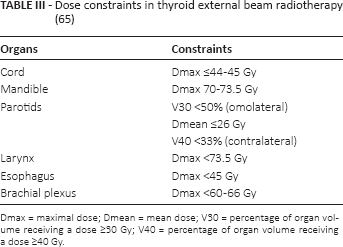
Dmax = maximal dose; Dmean = mean dose; V30 = percentage of organ volume receiving a dose ≥30 Gy; V40 = percentage of organ volume receiving a dose ≥40 Gy.
Chemotherapy association
Differentiated thyroid carcinoma
In the adjuvant setting, chemotherapy is not usually prescribed in DTC. In a cohort of 66 patients with advanced or recurrent DTC treated with EBRT, concurrent chemotherapy resulted in a nonsignificant improvement in LR PFS at 3 years (90% vs 73%). Administered schedules were doxorubicin (10 mg/m2), cisplatin (100 mg/m2), cisplatin (60 mg/m2) with etoposide (120 mg/m2), and doxorubicin (10 mg/m2) followed by paclitaxel (40 mg/m2) (10).
Medullary thyroid carcinoma
In MTC, chemotherapy has historically shown little efficacy and there is no evidence of advantages administering adjuvant chemotherapy (2).
Anaplastic thyroid carcinoma
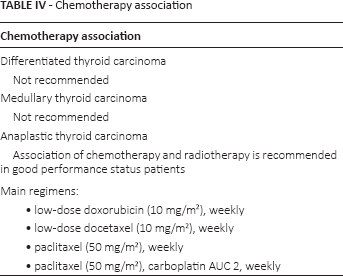
Anaplastic thyroid carcinoma is an aggressive disease and adjuvant treatments often involve cytotoxic chemotherapy. The ATA guidelines recommend the use of chemotherapy with EBRT in good performance status patients. Most administered schedules include taxanes, anthracyclines, and cisplatin alone or in some combinations (5). The MSKCC reported a local tumor control rate at 2 years of 68% and a 1-year survival rate of 50% with radiation with concurrent weekly low-dose doxorubicin (10 mg/m2) (66). Sherman et al (20) reported a median LR PFS of 10.1 months, increased to 35.9 months with EBRT doses >50 Gy. Superiority of chemotherapy with at least 5 cycles of doxorubicin was significant on univariate analysis but it was not significant on multivariate analysis (54).
Reports on patients treated with concurrent low-dose weekly docetaxel (10 mg/m2) showed high efficacy of concomitant treatment (67-68-69).
In a prospective trial, 24 patients with nonmetastatic ATC received 2 cycles of cisplatin plus doxorubicin chemotherapy after surgery, followed by hyperfractionated EBRT (40 Gy in 2 daily fractions of 1.25 Gy) and by 4 cycles of the same schedule of chemotherapy. The authors observed a complete response in 8 patients after a median follow-up of 35 months. Death was mainly related to distant metastases rather than to local progression (68% vs 5% of cases) (58). Receptor tyrosine kinase inhibitors have an increasing role as single agents or with cytotoxic chemotherapy (60). An ongoing phase II study is evaluating the addition of pazopanib to paclitaxel and IMRT (70).
Although adjuvant chemotherapy could improve disease control, an increased toxicity rate should be considered and its use should be evaluated on the basis of patient performance status. Key recommendations are summarized in Table IV.
Chemotherapy association
Complications
Exceeding the dose tolerance of the organs at risk can cause complications such as spinal cord dysfunction, xerostomia, dysphagia, osteonecrosis, and brachial plexopathy.
Cord dysfunction
Delayed injury to the spinal cord typically is manifested by a chronic, progressive myelopathy. Less commonly, such injury can be manifested as a lower motor neuron syndrome or as a hemorrhagic injury. Often the onset is insidious. Paresis, numbness, and sphincter dysfunction developing 6 to 12 months after irradiation are the typical manifestations of progressive radiation-induced myelitis (71). In general, neurologic symptoms do not remit (72, 73).
Xerostomia
Radiation-induced damage to the salivary glands changes the volume, consistency, and pH of secreted saliva from thin secretions with a neutral pH to thick and tenacious secretions with increased acidity. Patients may have oral discomfort or pain and these can lead to decreased nutritional intake and weight loss. Parotid dysfunction can be detectable at 10 to 15 Gy mean dose, and administration of approximately 40 to 50 Gy mean dose to a parotid gland typically causes >75% reduction in function. Although xerostomia often improves with time, it is a long-lasting and frequently permanent consequence (74, 75).
Dysphagia
Swallowing dysfunction is correlated with compromised quality of life and can lead to life-threatening complications, such as pneumonia. The best approach is to reduce as much as possible radiation doses to the pharyngeal constrictor muscles and to the larynx-hypopharynx (76).
Mandible osteoradionecrosis
The mandible is frequently exposed to radiation-related complications. It generally occurs with cumulative doses of 66 Gy and higher on the mandible (standard fractionation) delivered to a significant volume (77).
Brachial plexopathy
Brachial plexopathy is a peripheral nerve disorder in which nerve damage occurs at any point from the nerve roots to the terminal branches. Symptoms can vary from subtle to incapacitating shoulder, arm, and hand pain, numbness, paresthesias, weakness, muscle atrophy, and paralysis. Treatment is purely symptomatic and often ineffective. Recommended dose constraints range from 60 to 66 Gy in 2 Gy per fraction (78).
Conclusions
In patients with TC, EBRT has an unquestioned role for palliative treatments in metastatic disease. In locally advanced disease, a careful evaluation of the risk of recurrence and of acute and late toxicities is critical in determining the role of adjuvant treatments. Differentiated thyroid carcinoma, MTC, and ATC are 3 different diseases that require different management. In DTC, the role of EBRT is an issue of debate and should only be reserved to patients at high risk of LR disease in whom the potential benefit will outweigh the toxicity of the therapy and in whom no further surgery is possible. In MTC, the role of EBRT is controversial and should be considered in case of residual disease and extranodal spread. The role of EBRT in ATC is unquestioned. The body of evidence also indicates that a role of concurrent radiochemotherapy should be considered on the basis of the patient performance status. In all likelihood, new technologies will play an important role in helping to conform the dose accurately. It is hoped that either multicenter randomized trials will be started or a large international database will be created to clarify the role of this therapy.
Footnotes
Acknowledgment
The authors thank Dr. Paola Chiovati for help in preparing the figure and Dr. Daniela Michilin for editorial support during preparation of this manuscript.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.