
Abstract
Pazopanib is an oral multikinase inhibitor that has proved effective in adults treated for relapsing soft tissue sarcoma and synovial sarcoma in particular. Two cases are reported here of pediatric patients with pretreated relapsing synovial sarcoma whose tumors showed a prolonged response to pazopanib given on compassionate grounds. These results suggest that new agents found effective in adult patients might achieve similar results in adolescents with the same disease. Facilitating the availability of new drugs for children and adolescents is a major challenge for pediatric oncologists.
Introduction
Synovial sarcoma (SS) is a high-grade sarcoma that is locally invasive and tends to metastasize; it can occur at any age (1). The outcome of patients with SS depends mainly on the feasibility of surgical resection, tumor size and site, and the presence of metastases (2). In pediatric age, around 80% of patients with localized disease can be cured by means of a multimodal treatment approach, combining surgery with chemotherapy and radiotherapy according to the patients’ risk features (3). The chances of survival are still largely unsatisfactory, however, for patients with metastatic disease at diagnosis (5-year survival around 30%) (4), and for those with relapsing tumors (10-year survival around 20%) (5), for whom novel therapeutic strategies and new effective agents are therefore urgently needed.
Pazopanib is an oral multikinase angiogenesis inhibitor that has proved effective for the treatment of relapsing soft tissue sarcomas (STS) in adults (6, 7). Among the different histological subtypes of STS, pazopanib has been found particularly active against leiomyosarcoma and SS.
Here we report on 2 pediatric patients with pretreated relapsing SS whose tumors showed a prolonged response to pazopanib given on compassionate grounds.
Case Descriptions
The first case concerns a 14-year-old girl initially diagnosed with a retroperitoneal (SYT-SSX-positive) monophasic SS that was 11 cm in greatest diameter. She was treated at the Pediatric Oncology Unit of the Istituto Nazionale Tumori in Milan with neoadjuvant ifosfamide-doxorubicin chemotherapy, preoperative radiotherapy (50.4 Gy), then complete resection with histologically tumor-free margins, based on the European pediatric Soft tissue sarcoma Study Group (EpSSG) protocol (3). Sixteen months after completing her therapy, the girl experienced a metastatic relapse consisting of a single lesion 6 cm in size in the inferior lobe of the left lung. She was therefore administered 2 cycles of gemcitabine-vinorelbine chemotherapy (with no tumor response), then underwent lung metastasectomy followed by 6-month maintenance treatment with metronomic oral cyclophosphamide. Ten months after this lung surgery, a computed tomography (CT) scan showed bilateral multiple lung metastases. The patient was given 3 courses of trabectidin, with disease progression on CT scan, so trabectidin was stopped and oral pazopanib (800 mg once daily) was given on compassionate grounds. After 3 months of pazopanib therapy, CT scan showed a partial remission: a large tumor mass in the left lower lobe shrank from 8 cm to 5 cm, and a mass adhering to the left hemidiaphragm and chest wall from 8.5 cm to 6.5 cm (Fig. 1). Tumor response, with the volume of the lesions remaining stable, was maintained for 15 months. Pazopanib administration was well tolerated, with very good quality of life. The main side effects reported were hair depigmentation and grade 2 diarrhea. The diarrhea was poorly responsive to loperamide, and was responsible for the therapy being discontinued twice for 1 week, with a temporary improvement in symptoms. No other toxicity was reported. Pazopanib treatment was stopped after 15 months when a CT scan showed progression of the pulmonary lesions.
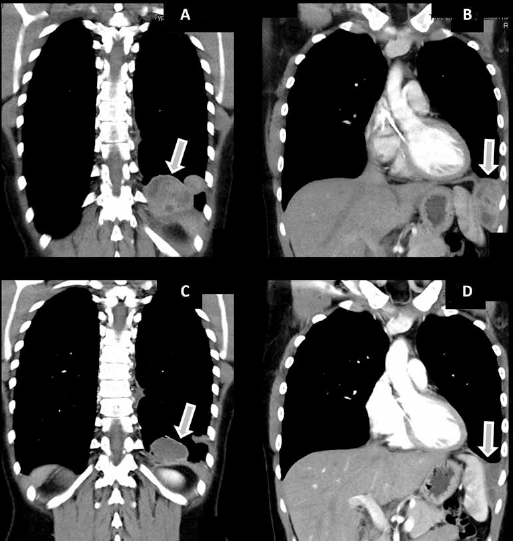
After 3 months’ therapy with pazopanib, a large mass in the left lower lobe shrank from 8 cm (
The second patient was a 13-year-old boy treated at the Pediatric Oncology Unit of the Regina Margherita Hospital, Turin, for a monophasic (SYT-SSX-positive) SS of the knee that was 10 cm in greatest diameter. He had a medical history of type 1 diabetes and insulin therapy. He was initially treated with marginal resection, ifosfamide-doxorubicin chemotherapy and radiotherapy (54 Gy) according to the EpSSG protocol (3). Nine months after completion of this treatment, a local relapse was detected and treated with complete surgical resection. Sixteen months later, CT scan revealed bilateral pulmonary metastases. The patient underwent metastasectomy followed by 6 cycles of high-dose ifosfamide in continuous infusions (14 g/m2 over 14 days) by means of an elastomeric pump. Eight months after his last course of treatment, the patient had local and lung recurrences (multiple metastases). He underwent further local resection followed by brachytherapy, and treatment with oral pazopanib was started at a dose of 400 mg twice daily. After 5 months of treatment, a lung CT scan showed some tumor response (33% volume reduction of the pulmonary metastases); subsequent CT scans showed stable disease. Response to pazopanib was maintained for 14 months, then lung progression was detected, associated with concomitant pneumothorax. Overall, the treatment was well tolerated, the main toxicities being hair depigmentation, grade 2 hyperbilirubinemia, grade 1 hypertension, and grade 2 diarrhea. No hematological or other clinical toxicities were recorded. The patient's hyperbilirubinemia and diarrhea prompted a 1-month 50% dose reduction on 2 occasions, and after 9 months of pazopanib therapy, the dose was definitively reduced to 50% (400 mg daily).
Discussion
Pazopanib is an oral multi-tyrosine kinase inhibitor that is active on various signaling pathways (VEGFR-1, -2 and -3, PDGFR-α and -β, FGFR-1 and -3, and KIT) and effective in preventing angiogenesis and metastasis in STS, and SS in particular (7). It is a promising treatment for delaying progression in pretreated adults with advanced STS, and it has been approved for this indication by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA).
Despite the encouraging results of pazopanib in adults with pretreated SS, there is still very little experience of its use in pediatric patients, for whom it has yet to be approved. A phase I trial in children with relapsing tumors showed that pazopanib was potentially of clinical benefit in pediatric patients (8), while a phase II trial is currently ongoing.
It is fundamentally important to investigate the clinical and biological differences in a given histological type occurring in pediatric and adult age. Previous studies have suggested that the outcome of SS differs in children and adults (1, 9) and recent biological research has shown differences in the related genome instability too (10). At the same time, given the poor prognosis of pediatric patients with relapsing SS and the current lack of standardized treatment for such cases (5), it is crucial to identify innovative approaches. The feasibility of trials on new agents in minors is limited and only a minority of children and adolescents with cancer have access to innovative therapies, so it seems important for pediatric oncologists to devise ways to draw on the experience gained by medical oncologists treating adults, with a view to applying any positive results achieved in adults to younger patients too.
The 2 cases described here of a clinical response in adolescent patients with pretreated relapsing SS go to show that a new agent found effective in adult cancer patients may achieve similar results in adolescents with the same disease – though this may be true of pazopanib, but not apply to other drugs. To increase the availability of new drugs for the treatment of children and adolescents, pediatric oncologists need to improve their networking with adult oncology groups, and also with pharmaceutical industries and regulatory authorities.
Footnotes
Financial support: None.
Conflict of interest: The authors have no potential conflicts of interest to disclose.