
Abstract
In metastatic colorectal cancer, the optimization of upfront treatment and the continuum of care based on patients’ exposure to multiple treatment lines have reached a plateau of efficacy. Therefore, a paradigm shift is ongoing towards precision medicine and personalized treatments based on the specific molecular features of the disease. In this perspective, the improved knowledge of disease biology coming from the lab has prompted a rapid translation from bench to bedside of newer targeted strategies. Here, we focus on the most promising biomarkers already included or close to adoption in daily clinical practice. In particular, evidence about the potential roles of BRAF mutation, HER2 amplification, MGMT methylation, microsatellite instability, and ALK, ROS and NTRK1–3 rearrangements as positive predictors of benefit from biological agents is reviewed and discussed.
Introduction
Over the last years, the availability of targeted agents and the identification of molecular markers able to drive therapeutic decisions have led to the “fragmentation” of solid malignancies into different entities with distinctive biological characteristics, prognostic features, and especially treatment options. In fact, the early recognition of positive predictors of benefit from new drugs has made the assessment of those markers an urgent need for medical oncologists, in order to choose the best option for each patient from the very first steps of his or her therapeutic route.
The recent history of colorectal cancer (CRC) was marked by the same process. However, the fragmentation into different molecularly defined entities was not based on positive predictors of benefit from targeted drugs but rather on the identification of predictors of resistance to a class of drugs, i.e., the anti-EGFR monoclonal antibodies cetuximab and panitumumab.
In 2008, panitumumab was the first agent in metastatic CRC (mCRC) to be approved only for a molecularly defined subgroup of patients: those not bearing KRAS codon 12 and 13 mutations. It took around 5 years and many retrospective analyses to acknowledge the negative predictive impact of rare KRAS mutations occurring in exon 3 (codon 59 and 61) and 4 (codon 117 and 146) and NRAS mutations in exon 2 (codon 12 and 13), 3 (codon 59 and 61) and 4 (codon 117 and 146), with the same functional meaning.
Mainly based on the post-hoc analysis of a phase III randomized study assessing the efficacy of the addition of panitumumab to first-line FOLFOX4 (1), the labels of both cetuximab and panitumumab were changed in 2013 to limit the use of anti-EGFR monoclonal antibodies to RAS wild-type patients, i.e., those not bearing the above-mentioned mutations. A substantial role in that decision was played by the potential detrimental effect of treating RAS-mutant patients with an anti-EGFR monoclonal antibody, especially when combined with an oxaliplatin-based chemotherapy backbone.
Although RAS status is today the only molecular marker taken into account by regulatory restrictions, the clinical impact of other markers is well established, so that some of them are already routinely tested in many institutions while others will probably be implemented in the near future.
The aim of the present review is to briefly summarize the available evidence on molecular markers, other than RAS status, with immediate impact on the management of mCRC patients (Tab. I and Fig. 1) and to outline some future prospects in the field of clinical and translational research.
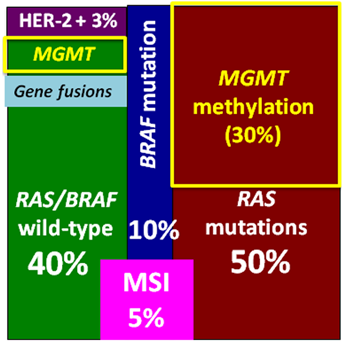
Summary of molecular alterations clinically relevant for the management of mCRC.
Molecular markers currently used or potentially useful in daily practice
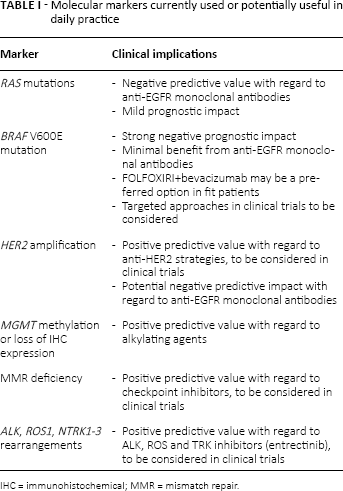
IHC = immunohistochemical; MMR = mismatch repair.
BRAF Status: The Never-Ending Story
BRAF mutations affecting codon 600 arise in 8%–10% of patients with mCRC and are thought to be mutually exclusive with RAS mutations, based on results from patients included in clinical trials (2, 3). However, it should be noted that the prevalence of BRAF V600E mutation may be higher in the real-life setting (4) due to the fact that these patients are often ineligible for enrolment in controlled trials because of their poor performance status or for having non-evaluable disease according to RECIST. In fact, the spread of BRAF V600E-mutant tumors often includes the lymph nodes and peritoneum as metastatic sites (2). Moreover, BRAF mutation is much more frequent in right-sided than left-sided tumors (2).
While the negative prognosis of BRAF V600E-mutant mCRC is well known (with the median duration of survival for these patients across different trials and series worldwide being around 12 months), the impact of the BRAF mutation as a negative predictor of benefit from anti-EGFR monoclonal antibodies has been a matter of debate for a long time.
The biological rationale underlying the potential role of BRAF V600E mutation in driving the resistance to EGFR inhibitors is supported by strong preclinical evidence (5) and was first confirmed in an extensive body of data from a number of large series reporting no response to anti-EGFRs alone in the chemorefractory setting (6, 7).
More recently, 2 meta-analyses addressed this question. Rowland et al (8) assessed the predictive value of BRAF V600E mutation evaluating the relative impact of adding cetuximab or panitumumab to standard chemotherapy options or best supportive care (BSC) in BRAF wild-type (wt) and BRAF V600E-mutated mCRC, respectively. While the addition of an anti-EGFR in RAS-wt/BRAF-wt patients provided a clear benefit, maximizing the effect of the targeted agent, the impact in RAS-wt/BRAF-mutant patients was less convincing, with a borderline significant p value (p = 0.07) for the interaction in terms of progression-free survival (PFS). Eight randomized trials including a total of 351 RAS-wt/BRAF-mutant patients were included in that study.
Similarly, an Italian meta-analysis (9) included 10 clinical trials and a total of 463 patients with RAS-wt/BRAF-mutant mCRC, and reported that adding cetuximab or panitumumab to standard therapy or BSC did not significantly improve the overall response rate (ORR) (relative risk [95% confidence interval (CI)] = 1.31 [0.83–2.08]; p = 0.25), PFS [hazard ratio (HR)] [95% CI] = 0.88 [0.67–1.14]; p = 0.33), or overall survival (OS) (HR [95% CI] = 0.91 [0.62–1.34]; p = 0.63).
Overall, based on these results, while the negative predictive role of BRAF V600E mutation cannot be definitely and formally demonstrated, the minimal magnitude of the effect of adding anti-EGFR monoclonal antibodies is clear.
Recent data from the phase III CALGB 80405 trial of first-line doublet chemotherapy plus bevacizumab versus doublet chemotherapy plus cetuximab in KRAS-wt mCRC patients evidenced a significant interaction between primary tumor site and treatment effect (10). In particular, while a clear benefit from doublet chemotherapy plus cetuximab was observed in tumors distal to the splenic flexure, the combination with bevacizumab seemed more effective in those proximal to the right flexure. Consistent results were reported in the subgroup analysis of the phase III FIRE-3 study of first-line FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab in RAS-wt mCRC (11). Nevertheless, the higher prevalence of BRAF V600E mutations in right- than left-sided tumors cannot be neglected. In fact, a retrospective analysis of extensively characterized RAS-wt patients treated with anti-EGFR monoclonal antibodies showed that in a multivariable model including BRAF mutational status as a covariate, the association of primary tumor site with clinical outcome was no longer significant (12).
Moreover, the potential efficacy of a more intensive first-line regimen in BRAF V600E-mutant mCRC, the triplet FOLFOXIRI combined with the antiangiogenic bevacizumab, has been suggested by 3 subsequent experiences: the retrospective analysis of the phase II FOIB study (13), a prospective phase II single-arm trial (14), and the subgroup analysis of the phase III TRIBE study (3). Taken together, notable results in terms of reponse rate, PFS and OS were reported with FOLFOXIRI plus bevacizumab also in BRAF-mutant mCRC patients, thus confirming that intensified first-line chemotherapy may be efficacious to counteract the intrinsic biological aggressiveness of this disease. Drawing from these data, though in the absence of high-level evidence, FOLFOXIRI plus bevacizumab is regarded by international guidelines (15) as the preferred first-line option for fit patients with BRAF V600E-mutant tumors, and the assessment of BRAF status is recommended both for its prognostic and therapeutic implications.
The relevance of BRAF V600E mutation as a crucial driver of tumor growth and progression has been challenged by trials assessing the activity of BRAF inhibitors in this setting, and reporting disappointing results (16, 17) especially in comparison with observations in metastatic melanoma. Different explanations for these negative results have been hypothesized: the evidence of a small pre-existing clone of RAS-mutant cells also in BRAF-mutant tumors, leading to the hyperactivation of intracellular pathways downstream of RAS and other than BRAF (16); the high level of intratumoral heterogeneity with regard to BRAF status (18); and the hyperactivation of EGFR through a feedback loop induced by BRAF inhibition (19). As a consequence of the last hypothesis, new strategies combining EGFR and BRAF inhibitors have been developed with better results at least in terms of objective response rates (17, 20). More interesting results were achieved with a triplet of targeted agents including a MEK or PIK3CA inhibitor in addition to an EGFR and BRAF inhibitor (21, 22). All these regimens have been evaluated in early-phase trials in advanced treatment lines, and the small numbers of treated patients prevent us from drawing definitive conclusions about their impact on the prognosis of BRAF V600E-mutant patients. However, while objective responses have been reported in about 1 in 3 patients, their duration seems quite short, thus making more mature data indispensable to move toward new phases of development. The assessment of BRAF codon 600 status is therefore recommended also to make sure these patients will have the opportunity to be included in dedicated clinical trials.
Finally, the application of new sequencing technologies able to look at many different hotspots at a glance and to provide a comprehensive overview of thousands of genomic alterations make the clarification of mutations occurring in other hotspots of BRAF an urgent need. Interestingly, rare BRAF mutations in codons 594 and 596 do not predict poor prognosis or resistance to anti-EGFR monoclonal antibodies but seem to identify a good-prognosis subtype of mCRC (23).
HER2: The First Example of Precision Medicine in mCRC
In the attempt to disclose the mechanisms of intrinsic resistance to EGFR inhibitors other than RAS and BRAF mutations, amplification of HER2 was detected in some patient-derived xenografts resistant to cetuximab or panitumumab and propagated in nude mice (24).
In order to identify new therapeutic options for this molecularly defined subtype of mCRC, mice bearing HER2-amplified, cetuximab-resistant xenografts were treated with various HER2-targeted therapies, alone or in combination. While monotherapy with either HER2 tyrosine kinase inhibitors or anti-HER2 antibodies was mostly ineffective, the combination of an antibody (pertuzumab or trastuzumab) and a tyrosine kinase inhibitor (lapatinib) led to sustained tumor shrinkage. For this reason, the combination of trastuzumab and lapatinib was chosen for a prospective phase II trial of precision medicine, the HERACLES study, in KRAS-wt patients refractory to all available treatments including fluoropyrimidines, oxaliplatin, irinotecan, cetuximab and panitumumab. Previous exposure to bevacizumab was allowed but not mandatory. In order to standardize the assessment of HER2 status in colorectal cancer, diagnostic criteria were carefully established and HER2 amplification was found in around 5% of KRAS-wt tumors (25).
The HERACLES study met its primary endpoint, reporting 8 RECIST responses out of 27 heavily pretreated patients receiving trastuzumab and lapatinib. Not only was noticeable activity of the combination demonstrated, but there were tangible results in terms of duration of response. Interestingly, none of the patients whose outcome during previous anti-EGFR was known achieved a response (26).
The role of HER2 amplification as a new target in mCRC has been confirmed by the results of the HER2-amplified cohort of the MyPathway study, which investigated different targeted strategies based on the expression of the specific target (27). Five of 13 HER2-amplified or mutated patients treated with the combination of trastuzumab and pertuzumab responded and 10 achieved disease control.
The negative predictive impact of HER2 amplification with regard to anti-EGFR monoclonal antibodies was reaffirmed in a recent experience (28). Of 114 RAS-wt patients previously treated with an anti-EGFR agent and screened for phase I trials, 14 (12%) were found to be HER2 amplified. Since HER2 amplification and BRAF mutation were mutually exclusive, the prevalence of HER2 amplification in RAS/BRAF-wt tumors was 14%. The duration of PFS in HER2-amplified patients was significantly shorter than in patients in whom HER2 was not amplified. The same result was obtained in an independent cohort of 37 HER2-amplified patients compared with 62 non-amplified patients treated with anti-EGFR-based regimens. Notably, in both cohorts the PFS of HER2-amplified and non-amplified patients during first-line regimens not including an anti-EGFR agent did not differ, thus supporting the negative predictive value rather than prognostic weight of HER2 amplification.
Based on both its positive predictive role with respect to HER2-targeting strategies and its negative predictive impact with respect to anti-EGFR monoclonal antibodies, the implementation of HER2 assessment in daily practice may provide useful information for therapeutic choices.
Microsatellite Instability: The Niche of Immunotherapy in mCRC
The immune system plays a crucial role in CRC. In fact, the fraction of tumor-infiltrating CD8+ lymphocytes in primary resected tumors is associated with disease outcome (29–31). The presence of effector memory T cells is more important than that of naive T cells in impacting disease-free and overall survival. The recent widespread use of immune checkpoint inhibitors for the treatment of advanced melanoma and non-small cell lung cancer (32–34) has prompted further research for several tumors, including mCRC.
However, the anti-PD1 monoclonal antibody nivolumab failed to show marked activity in unselected, heavily pretreated patients with mCRC (35). Interestingly, 1 of 17 patients from the phase I study had a microsatellite instability-high (MSI-H), PD-L1-positive tumor and achieved long-lasting complete remission (36). Pembrolizumab was recently investigated in a phase II study carried out in 32 pretreated mCRC patients, of whom 11 had MSI-H and 21 microsatellite-stable (MSS) tumors. (37). The immune-related response rate and clinical benefit were very promising in patients with an MSI-H status (40% and 78%, respectively), whereas treatment activity was negligible in those with MSS tumors. Recently, the CheckMate-142 interim results confirmed the promising activity of nivolumab alone or in combination with the anti-CT-LA4 monoclonal antibody ipilimumab in patients with MSI-H mCRC independent of BRAF mutational status (38).
Since MSI-H status is associated with improved outcomes in stage II-III CRC, its frequency is considerably lower in mCRC (not superior to 5% of cases) (39, 40). Since somatic mutations may be recognized as neoantigens by the host immune system, it has been hypothesized that the extremely high mutational load associated with MSI-H cancers (including mCRC) may drive the efficacy of immune checkpoint inhibitors (41–43). Therefore, MSI-H has emerged as a positive biomarker for the selection of mCRC patients for immunotherapy. Not surprisingly, inflammatory infiltrates found in MSI-H CRC show higher PD-L1 expression, which is the treatment target of agents such as nivolumab and pembolizumab (44–45). Since immunotherapy lacks substantial efficacy in MSS tumors – which constitute about 95% of cases – several strategies are emerging to increase the sensitivity to immune checkpoint inhibition. In particular, in preclinical models, targeted inhibition of MEK leads to upregulation of MHC I on tumor cells, induces intratumoral T-cell infiltration, and enhances anti-PD-L1 activity. Recently, the results were presented of a phase I study of the MEK inhibitor cobimetinib in association with atezolizumab (atezo; MPDL3280A), an engineered antibody that inhibits binding of PD-L1 to its receptors. A promising response rate of 17% (4/23) was reported in chemotherapy-refractory patients with KRAS-mutated, MSS mCRC (46).
MGMT Promoter Methylation or Loss of MGMT Immunohistochemical Expression
MGMT is a repair protein that removes alkylating groups from the 06-guanine in DNA. It protects normal and tumor cells from this type of DNA damage by moving the alkylating group to a cysteine residual within its own protein (47). Approximately 40% of mCRCs show silencing of the MGMT gene, leading to absence of the corresponding protein. Due to this deficiency, the tumor cell is not able to effectively repair O6-methylguanine adducts, causing a higher frequency of G:C > A:T transitions and potentially enhancing the susceptibility to the cytotoxic effects of alkylating agents such as temozolomide and dacarbazine (48, 49). MGMT deficiency can be assessed in tumor samples either as promoter hypermethylation by methyl-specific PCR (MSP) and digital PCR quantification by methods such as Methyl-BEAMing (50) or lack of protein expression by immunohistochemistry (IHC) (51).
While the validation of MGMT as a predictive biomarker has been achieved for glioblastoma, where alkylating agents have been the backbone of systemic treatment for years, the same is not the case for mCRC, where these drugs have very limited activity. Indeed, only few data are available regarding treatment of CRC with these agents based on MGMT methylation. In particular, 5 phase II clinical trials have assessed the clinical efficacy of alkylating agents in mCRC based on MGMT deficiency as a biomarker (51–55). In all these studies, a selection was made by assessing promoter hypermethylation by MSP on formalin-fixed paraffin-embedded archival tumor tissue. Response rates ranged from 4% to 16% in heavily pretreated populations. Even though MSP is a well-standardized assay in melanoma and glioblastoma, selection according to this methodology in CRC appears to be a useful but not optimal condition for achieving clinical benefit. In fact, digital PCR quantification of MGMT methylation could further refine patient selection, with benefit restricted to patients with highly hypermethylated tumors (55). Moreover, low MGMT expression at IHC is found in about one-third of MSP-methylated samples and was associated with an increased response rate (54). A pooled cohort of 105 mCRC patients treated with alkylating agents indicated that assessment of MGMT promoter methylation coupled with reduced protein expression optimizes the prediction of response, and that MGMT promoter methylation with reduced protein expression is strongly associated with improved response rates, PFS and OS following treatment with alkylating agents, (unpublished data).
ALK, ROS and NTRK1–3 Fusions: Good News for a Limited Subgroup of mCRC Patients
Gene rearrangements determining constitutive activation of tyrosine kinase receptors have been identified as drivers of tumor progression and oncogenic events in a wide range of solid malignancies (56). While the role of ALK and ROS as therapeutic targets is well established in a subgroup of non-small cell lung cancers, recent evidence also underlines the existence of a small fraction of CRCs bearing these molecular alterations with a potential driving impact. Overall, the incidence of gene fusions in CRC is in the range of 0.5%–2% and their prognostic and predictive impact is far from being elucidated (57–68). Nevertheless, encouraging results have been obtained in patients treated with entrectinib in the phase I STARTRK-1 study, leading to the design of the STARTRK-2 basket study. Entrectinib is a small molecule that selectively inhibits ALK, ROS1 and TrkA-B-C, encoded by the ALK, ROS1 and NTRK1–2–3 genes, respectively. Entrectinib was able to induce impressive responses in 2 heavily pretreated mCRC patients harboring LMNA-NTRK1 (63) and CAD-ALK fusions (65). Similarly, an mCRC patient bearing the STRN-ALK fusion experienced clinical benefit when exposed to the ALK inhibitor ceritinib (67).
In spite of these promising findings, the evidence about the actual clinical impact of identifying these alterations is not clear-cut. A strong biological rationale supported by preclinical in vitro findings (69) seems to suggest a low EGFR dependency of these tumors, leading researchers to hypothesize a lack of benefit from anti-EGFR monoclonal antibodies in this subset of patients and encouraging clinicians to adopt targeted approaches as soon as possible in the disease course of these patients. Strong help from translational research is currently awaited to further deepen the relevance of gene fusions in the management of mCRC patients.
Future Prospects
Recent advances in the molecular characterization of mCRC have clearly changed our clinical practice and opened the way toward new challenges and new research. First of all, the identification of potentially relevant genetic alterations occurring in very small percentages of mCRC patients makes multicenter and hopefully multinational efforts mandatory in order to answer the most pressing questions about these rare entities. Second, the fragmentation of mCRC into different molecular entities implies a radical change in the paradigm of investigational drug development and a shift in the traditional methodology of clinical trial design.
Third, while some progress in refining the selection of patients who may benefit from anti-EGFR monoclonal antibodies has been made, in spite of many attempts no predictors of benefit from antiangiogenic agents have been identified. Although several antiangiogenic drugs with different mechanisms of action are currently indicated across different lines in the treatment of mCRC patients, no steps forward have been made in the last decade to optimize their use in clinical practice. While it is rather difficult that a “black or white” molecular marker might be able to account for such a complex biological process involving many different actors, also more comprehensive and sophisticated approaches failed to identify promising markers.
Finally, even if targeted approaches clearly have improved the prognosis of patients with mCRC, these drugs provide benefit for a limited (shorter or longer) duration. Then mechanisms of acquired resistance invariably occur and further enhance the intrinsic clonal heterogeneity of mCRC.
Liquid biopsies represent an intriguing tool to study the dynamism of tumor evolution across different lines of treatment, through a minimally invasive procedure. Nevertheless, the lack of cutoff values able to discriminate molecular events that are either clinically meaningful or not limits the applicability of these sensitive technologies in daily clinical practice, although they do highlight the need to include these prospective evaluations in properly designed clinical trials.
In conclusion, joint efforts of treating physicians and laboratory personnel are needed to quickly implement in the routine clinical activity news from the bench, and to interrogate the bench with questions coming from the bedside. Only a short, though significant, segment of the much longer way towards precision medicine in mCRC has been covered so far, but robust foundations to build further steps have been laid.
Footnotes
Abbreviations
Financial support: No financial support was received for this submission.
Conflict of interest: Chiara Cremolini declares advisory/consultant roles for Roche, Amgen, Eli-Lilly, Bayer and Merck-Serono. Filippo Pietrantonio declares advisory/consultant roles for Roche, Amgen, Eli-Lilly, Bayer and Sanofi-Aventis.