
Abstract
Purpose
Before the wait-and-see policy became the standard approach in abdominal wall desmoid tumors, surgery was performed on a systematic basis. Surgery remains indicated for progressing tumors but its extent is debatable. The abdominal wall is a common site of origin of sporadic desmoids, usually associated with a favorable prognosis. We analyzed the results of surgery at this specific site.
Methods
Data from 33 patients affected by sporadic desmoid tumors of the abdominal wall (31 primary, 2 recurrent) consecutively treated at our cancer center between January 2000 and September 2013 were retrospectively studied.
Results
Twenty-nine patients underwent surgery upfront and 1 after progression during the initial wait-and-see period. Prosthetic reconstruction of the abdominal wall was required in 28 patients. The average hospital stay was 5 days. Three patients developed surgical complications. Local recurrence-free survival was 90% at 5 and 10 years. Three patients had an uneventful childbirth during the follow-up after surgery.
Conclusions
Desmoid tumors of the abdominal wall have a favorable prognosis after surgical resection, which remains a safe and effective treatment. Wild-type tumors are common, whereas the incidence of S45F mutation in the beta-catenin gene is lower than in other anatomic sites. Upfront surgery may be considered in selected women who wish to bear a child.
Keywords
Introduction
The clinical behavior and mutational status of sporadic desmoid tumors (sDTs) differ from those of desmoids occurring in association with familial adenomatous polyposis (FAP) (1–3). While somatic APC mutations are rarely identifiable in sDTs, a high prevalence (∼85%) of mutations of CTNNB1 (the gene encoding for beta-catenin) characterizes sDT (4). sDT predominantly affects young adults, with a female predominance (5–7). The pattern of growth is infiltrative and surgical resection must be wide to obtain negative resection margins. About 20%–25% of patients experience 1 or multiple recurrences after resection (8–11). Medical treatments include antiestrogen therapy such as tamoxifen or toremifene, nonsteroidal antiinflammatory drugs such as indomethacin, sulindac or celecoxib, and chemotherapy (mainly methotrexate and vinblastine/vinorelbine or doxorubicin-based combinations) (12, 13). Radiotherapy has been used alone or in combination with surgery (14, 15), but its role is controversial because severe complications may occur, including secondary tumors.
Currently, many referral centers and scientific organizations advise against an upfront surgical approach (16–20). There are 3 ongoing prospective trials on a wait-and-see (W&S) approach for aggressive fibromatosis conducted by French, Italian and Dutch groups.
Recently, a position paper from the Italian (ISG) and French (FSG) sarcoma groups proposed a stepwise approach to desmoid tumors (DTs) based on a W&S approach upfront (19). The algorithm was developed on the basis of a large body of evidence showing a 50% progression-free survival rate at 5 years for patients managed with a conservative approach. It remains very difficult to choose the best subsequent treatments for patients who progress. The algorithm suggests different therapeutic strategies according to the site of the tumor, because different anatomic sites have different risks of local recurrence and morbidity.
Against this background we decided to analyze our series of patients treated for sDT of the abdominal wall, because this is a common site of origin of DT that in our opinion requires peculiar consideration.
Methods
We reviewed the records of all patients treated for sDT of the abdominal wall at the Humanitas Clinical and Research Center, Rozzano (Milan), Italy, between January 2000 and September 2013. Patients affected by FAP were excluded from the study. Diagnosis was always obtained through a percutaneous core-needle biopsy. Colonoscopy was performed to rule out FAP.
Patients were treated with upfront surgery until the end of 2010. From the beginning of 2011 we started to propose a conservative approach to patients. We then suggested surgery to patients with small tumors who progressed during the W&S period, while we suggested medical therapy to patients with large tumors who progressed during the W&S period. When the patient affected by DT was a young woman who wanted children, the possible alternatives were discussed with the patient and the final decision depended mainly on the attitude of the patient and the size and site of the tumor.
The Clavien-Dindo classification was used to classify surgical postoperative complications (21).
Pathological Evaluation of Cases
All DT cases were selected and diagnosed by an expert soft-tissue pathologist based on morphological and immunohistochemical features and according to the WHO classification of soft tissue tumors (2).
To perform molecular analysis, genomic DNA was extracted from the paraffin block using the QuickGene SP Kit (Fujifilm). Genetic analysis of CTNNB1 was performed by PCR amplification according to standard technique (4).
Statistical Analysis
Data are reported as numbers and percentages, or mean and standard deviation, as appropriate. The examined outcomes of this study were local recurrence-free survival (LRFS) and incidence of surgical complications. LRFS was the interval between the date of surgery and the date of detection of local recurrence, or the date of last follow-up for patients with no local recurrence. All potential prognostic factors were analyzed by univariate Cox regression analysis. P values <0.05 were considered significant. Statistical analysis was performed with Stata 13 (StataCorp LP).
Results
The patient and tumor characteristics of the 33 consecutively treated patients are shown in Table I. Thirty-one presented with primary lesions and 2 with recurrent tumors operated on elsewhere several years earlier. Surgical resection was performed in 30 cases. Twenty-nine patients had upfront surgery whereas 1 patient was operated on after an initial W&S period.
Tumor and patient characteristics
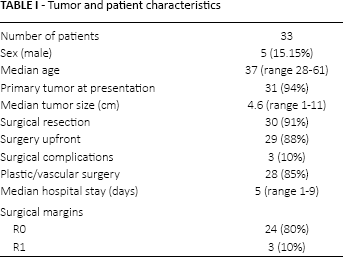
Twenty-eight patients required prosthetic reconstruction of the abdominal wall. We mainly used polypropylene or composite PROCEED (Ethicon) meshes. The surgical margins were classified as R0 in 24 cases (80%) and R1 in 3 cases (10%). In 3 cases the surgical margin status was not clear from the histological report.
Three patients (10%) developed postoperative complications including an abdominal hernia in 2 patients 3 and 5 years from tumor resection despite the use of a prosthetic mesh, and mild wound infection in 1 patient. The wound infection was treated successfully with antibiotics. One patient had surgery for hernia repair, while the other patient had a small, symptomless hernia that did not require any treatment. Surgical complications were classified as grade 1 in 1 case, grade 2 in 1 case, and grade 3b in 1 case.
Mutation analysis of the tumor was performed in 26 surigcally treated patients, while in the remaining 4 patients there was insufficient tissue for DNA extraction. The results are shown in Table II. A mutation in exon 3 of the CTNNB1 gene was identified in 13 cases (50%). Three different point mutations in 2 different codons were found in all mutated cases: T41A (n = 9; 69%), S45F (n = 3; 23%) and S45P (n = 1; 8%).
Mutation analysis of patients treated with surgical tumor resection
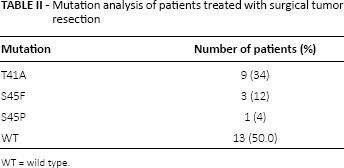
WT = wild type.
The average duration of follow-up for the entire series was 42 months (range 1–49). Three patients developed a local recurrence after surgery at our institution. Two underwent repeat surgery. The overall 5- and 10-year LRFS was 90% (95% confidence interval 71.05%–96.53%). Median time to relapse was 12 months (range 2–21 months). No patient had died of DT at the end of follow-up. Age was the only significant factor in univariate analysis for predicting local disease-free survival (LDFS) (Tab. III), with younger patients having a worse prognosis. The LDFS curves are shown in Figures 1 and 2.
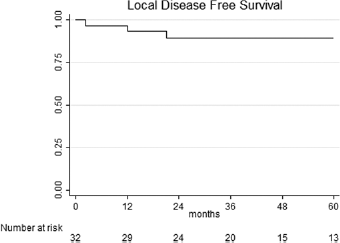
Local disease-free survival of patients treated with surgery.
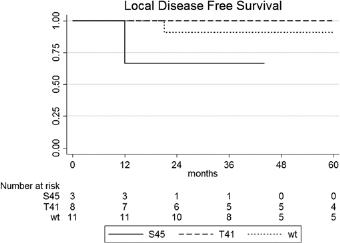
Local disease-free survival of patients treated with surgery according to tumor mutation (p = not significant).
Prognostic factors for tumor recurrence
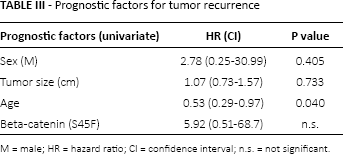
M = male; HR = hazard ratio; CI = confidence interval; n.s. = not significant.
During follow-up after surgery 3 patients became pregnant and gave birth, 1 by vaginal delivery and 2 by cesarean section. All 3 patients had prosthetic reconstruction of the abdominal wall with a mesh during the index operation. The vaginal delivery took place 5 years after surgical resection of the tumor; the cesarean sections were performed 6 and 7 years after tumor resection. No obstetric complications were reported. No recurrence of sDT was observed in these patients.
Four patients (1 man and 3 women) started a W&S period for 3 primary desmoids and 1 recurrent tumor. The median follow-up of this subgroup was 12 months (range 1–33). The male patient with the recurrent tumor was given an upfront W&S approach. The reason was that he did not have symptoms and data from the literature suggested a W&S approach to be best upfront. The tumor was located in the lower part of the abdomen, close to the left groin, and harbored a S45F mutation in the CTNNB1 gene. After 12 months of stable disease (SD) he had sudden major progression. At that point we performed en bloc resection of the tumor with resection of the iliac vein and abdominal hernia repair using a mesh. Vascular surgery would have not been necessary at the time of diagnosis of the recurrence. This patient had a further bifocal recurrence 1 year after our surgical treatment and started medical therapy with tamoxifen 40 mg plus celecoxib 200 mg daily. He currently has had SD for 7 months. One patient had complete tumor regression after 30 months of follow-up. One patient had slow progression and started tamoxifen 40 mg daily after 14 months of follow-up; she has had SD for 3 months. The last patient has SD after 5 months of follow-up.
Discussion
Sporadic DT has an unpredictable behavior. The tumor can grow, remain stable, spontaneously decrease in size or even disappear, but will never metastasize (2). We do not know the pathogenetic mechanisms that regulate its growth. Surgical trauma, estrogens and pregnancy seem to play a role in an enigmatic way (3, 22–25). The abdominal wall is a fairly common site of origin of sDT, especially in young women. Several studies have reported that sDTs originating at this anatomic site have a favorable outcome (26, 27). Nevertheless, there are few published series dedicated to the analysis of this specific site (10, 27).
Surgery was for a long time the mainstay of treatment for primary tumors. Now a large body of evidence suggests that a W&S approach is the best approach, because approximately one-third of patients remain stable and one-third show spontaneous regression after the initial W&S period (16–18, 27). For symptomatic patients and patients who progress during the W&S period the algorithm proposed by the ISG and FSG for abdominal DT suggests hormonal therapy followed by surgery for patients who further progress despite medical treatment (19), except for patients who progress rapidly during the W&S period: in this case surgery is suggested as the first choice instead of medical treatment. For patients who progress after observation and/or for resectable tumors that are symptomatic, the National Comprehensive Cancer Network (NCCN) guidelines recommend surgery and/or RT and/or systemic therapy. These guidelines state that the decision should be based on the location of the tumor and the potential morbidity of the treatment option.
W&s Approach
In our study, the few patients managed with an initial W&S approach had variable outcomes. The numbers of non-surgical patients are too small to draw any definitive conclusions; however, several previously published data on sDT suggest that this is an approach that benefits the majority of patients. A minority of patients could be disadvantaged by delayed treatment. In our series 1 patient experienced sudden progression of a recurrent tumor during the W&S period that prompted a more invasive surgical procedure compared with that planned at the outset. However, this patient had only temporary benefit from the surgical resection of the recurrence and had a bifocal relapse only 1 year following surgery. He likely would not have had any advantage in terms of local control from earlier surgical resection (i.e., when we detected the first recurrence), but he would have had a less extensive resection, without vascular surgery.
Medical Treatment
Medical treatment with tamoxifen is one of the best options after progression during the W&S period, whereas chemotherapy or radiotherapy should be reserved for symptomatic patients who further progress despite previous treatments. It can be hard to decide when to suggest tamoxifen and when to resect the progressing tumor. Several aspects should be balanced in the decision making. Tamoxifen is a chronic treatment and is associated with side effects. Although many of these side effects are mild and clinicians do not consider them important, menopausal symptoms make the treatment not always well tolerated by women. In a quality study performed by Harrow et al (28) in a group of women who had been prescribed tamoxifen or aromatase inhibitors for breast cancer, the researchers found that side effects were common and strongly affected the women's quality of life. Only rarely did patients seek advice about reducing the side effects they experienced; few were offered the opportunity to discuss the impact of side effects or the potential options available (28).
Tamoxifen can also, albeit rarely, induce hematological, hepatic and ocular toxicity (29). In addition, it increases the chances of endometrial cancer and thromboembolism (30). Therefore, treatment with tamoxifen might be the best first choice in case of slow disease progression during the W&S period for large tumors that would require a major surgical procedure, especially in men, and in women who do not wish to conceive.
Tamoxifen can also be considered for patients who rapidly progress during the W&S period. The ISG and FSG recommend surgery, but there is no clear evidence supporting surgery rather than medical treatment. In our series the only patient who had surgery for rapid progression of the tumor had a large, bifocal, symptomatic, early relapse. On the basis of this case and especially against the background of our experience of DTs at other anatomic sites, we currently prefer to start with medical treatment in patients who have rapid and major progression during the W&S observation, but prospective and consistent data are necessary to define the best approach in this subgroup of patients.
Surgical Resection
In our series the majority of patients were treated with an upfront surgical approach. The long-term results were very good in terms of local control with very low surgical morbidity. We performed extensive muscle resection to remove the tumor. Consequently a mesh to repair the abdominal defect was necessary in all cases but 1. With this aggressive surgical approach we obtained 80% of R0 margins and 90% of LDFS. No complications were observed during subsequent pregnancies and deliveries.
The good results of the surgical resection observed in our series suggest that at this specific anatomic site surgery remains among the best options for patients who progress after a W&S period, mostly when the patient has a small tumor, experiences side effects from tamoxifen, or has negative prognostic factors for thromboembolism and endometrial cancer. Upfront surgery can also be considered for women who wish to bear a child, especially when the tumor would impair an urgent cesarean section or in case of the need for hormonal stimulation. Surgical morbidity is low and pregnancy after abdominal mesh repair is possible.
Childbearing
For patients who wish to conceive, upfront surgery could be considered. Few data are available on desmoid behavior during pregnancy. Fiore and colleagues (31) reported a progression rate of about 50% during pregnancy for patients with a previously identified DT of the trunk or extremities and a progression rate of 80% for patients with a DT arising during pregnancy. They reported that disease progression during pregnancy was safely managed, also in patients with DT of the abdominal wall (28 patients). Nevertheless, in 2 cases, women required resection of the tumor during pregnancy. Since the sample in the mentioned multicenter series – the largest ever published – is too small to formulate any definitive recommendations about the obstetric risk, counseling a woman affected by a desmoid of the abdominal wall about pregnancy continues to be hard.
We think that the anatomic site of the tumor is a critical factor in the decision making. A desmoid growing in the hypogastrium and/or mesogastrium could generate problems in case of major progression or the necessity of an urgent cesarean section. Many desmoids grow in proximity to a previous cesarean section. Since in case of a pregnancy these patients have a high probability of needing another cesarean section, in our opinion they should undergo tumor resection before planning a pregnancy. The mesh repair does not impair subsequent pregnancy and delivery. In fact, both in our series and several other previously published ones, no complications were reported (32–34). In the multicenter series published by Fiore, an incisional hernia occurred in 3 of 5 patients after delivery in the context of a previous abdominal wall mesh reconstruction; surgical repair was required in 2 cases.
When the tumor is small and located far from the incision line of a cesarian section, the best option could be for the woman to go through pregnancy without DT treatment. Nevertheless, in such cases the assessment of tumor progression is problematic. In fact, the optimal radiological evaluation of tumor progression would require MRI with contrast enhancement, but MRI is considered safe only in the second and third trimesters (35, 36). Therefore, in the first trimester only ultrasound evaluation can be safely performed. In addition, contrast enhancement is not recommended during the whole pregnancy. This fact does not rule out the possibility to go through pregnancy with an untreated abdominal DT, but it requires that the clinicians, the patient and the radiologist share this challenging decision.
In case women need hormonal stimulation and medically assisted reproduction, we still suggest resection of the tumor before starting the procedure, because hormonal stimulation would increase the risk of DT progression. However, in the absence of certainty, all opportunities should be discussed with the patient in a referral center.
Molecular Analysis
The scientific literature suggests that the mutational status of the tumor may correlate with the risk of local recurrence. Several studies have reported that sDTs with the serine-to-phenylalanine substitution at codon 45 (the S45F mutation in CTNNB1) have a greater tendency towards local recurrence after surgical resection (4, 37–39).
In our study the incidence of the CTNNB1 S45F mutation was lower compared with other studies performed on sDTs of any anatomic site. We observed the S45F mutation in about 12% of cases compared with about 25% reported in the literature (37–39). There was a high rate of wild-type tumors compared with that reported in other studies, 50% in our work versus 15%–25% in the literature (37–39). A high percentage of wild-type tumors, which have a better prognosis, and the low incidence of S45F mutations, a recognized poor prognostic factor, could be the reason for the good prognosis of DTs located in the abdominal wall compared with other anatomic sites. In our work the S45F mutation did not appear to play a significant prognostic role. This could be related either to the limited number of events we observed or to a lesser impact of this mutation on the prognosis of tumors located in the abdominal wall.
Conclusions
Sporadic DTs of the abdominal wall have a good prognosis. Old age is a good prognostic factor. The incidence of the beta-catenin gene mutation S45F is lower than at other anatomic sites, while the incidence of wild-type tumors is higher.
Our study confirms that surgery of the abdominal wall for DTs is safe and effective. The series is too small to pinpoint the ideal candidate for surgery. Further studies are necessary to assess the best treatment for patients who rapidly progress during the W&S period and for women of child-bearing age.
To better characterize the ideal patient who benefits from either surgery or medical treatment, researchers should focus on seeking new prognostic factors.
Footnotes
Abbreviations
Financial support: None.
Conflict of interest: The authors declare they have no conflict of interest related to this article.