
Abstract
Purpose
To study the immunohistochemical expression of CD74 in series of invasive breast carcinomas classified according to their estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) immunoprofile and explore its correlation to Nottingham Prognostic Index (NPI) and tumor pathologic stage to determine if it has a prognostic value.
Methods
A total of 160 cases of mammary carcinoma were classified broadly according to their ER, PR, and HER2 expression into luminal, HER2-positive, and triple-negative groups. The NPI was calculated and pathologic stage was recorded for each individual case and cases were classified into different prognostic groups. The CD74 expression was evaluated immunohistochemically and correlated to different prognostic variables.
Results
The CD74 immunohistochemical expression in invasive breast carcinoma was significantly higher in triple-negative tumors, higher tumor grades, presence of lymph nodal metastasis, higher tumor stages, and higher NPI scores.
Conclusions
The CD74 might be a useful prognostic indicator predicting poor outcome of patients with breast carcinoma. Its consistent expression in triple-negative breast carcinomas points to the need of further studies to test the possibility if it can be targeted in treatment of breast carcinoma, especially in such groups.
Introduction
Despite early detection, treatment options, and survival improvement, the morbidity and mortality of invasive breast carcinoma continue to increase and many patients develop metastatic diseases that lead to death. Thus, there is an urgent need to identify novel prognostic biomarkers (1).
Clinically, this heterogeneous disease is broadly categorized into 3 basic molecular groups. The estrogen receptor (ER)-positive group is the most numerous and diverse. The human epidermal growth factor receptor 2 (HER2)-amplified group has great clinical success because of effective therapeutic targeting of HER2. Triple-negative breast cancers represent approximately 15% of the newly diagnosed cancers worldwide. The last group represents an important clinical challenge because these cancers do not respond to endocrine therapy or other available targeted agents, thus it is urgent to find active agents in this field of non-hormone-responsive lesions (2, 3).
Major histocompatibility complex (MHC) class II-associated invariant chain (Ii; CD74) is a type II transmembrane glycoprotein. It connects with the MHC II a and b chains and guides the convey of the abII complexes to intracellular endosomes and lysosomes, thus launching antigen presentation for immune response (4). With respect to these biological functions, it is possibly pertinent that CD74 is also expressed on a diversity of malignant cells.
CD74 expression has been described in hematologic (5, 6) and nonhematologic cancers, including gastrointestinal (7-8-9), renal (10), non-small-cell lung (11), and recently, glioblastoma cell lines (12). In many of these cancers, expression of CD74 has been proposed to be a prognostic factor, with its higher relative expression of CD74 correlating with tumor progression or poor clinical outcome (13, 14). The biological functions of CD74 together with its expression on malignant cells and limited expression on normal tissues suggest CD74 as a probable therapeutic target worthy to be studied further in other types of cancers (15).
Few studies explored CD74 expression in breast carcinoma (1, 16), so this work aims to study the immunohistochemical expression of CD74 in series of invasive breast carcinomas classified according to their ER, progesterone receptor (PR), or HER2 immunoprofile and explore its correlation to Nottingham Prognostic Index (NPI) and tumor pathologic stage to determine if it has prognostic value.
This retrospective study followed the ethical standards of and was approved by the Ethical Committee at Tanta Faculty of Medicine, Egypt.
Materials
The present study was carried out on 160 specimens of invasive breast carcinoma. Cases with hormonal profile and HER2 status were those to be included in this study provided that the blocks were of primary tumor from patients who underwent radical mastectomy, modified radical mastectomy, or conserving surgery including sentinel and/or axillary lymph node dissection, while patients who received neoadjuvant chemotherapy or who underwent preceding treatment at another institution or patients with second primary tumor were excluded. Data regarding primary tumor size, lymph node status, and pathologic stage (pTNM) according to Lakhani et al (17) were retrieved from pathology archives at Tanta University together with hormonal profile and HER2 status for each included case. Data about the real outcome of patients included in this study were missing as our cases were from archives as the regimen of treatment now differs in our institution and most patients receive neoadjuvant chemotherapy before surgery, which conflicts with our inclusion criteria.
Methods
Paraffin blocks from the primary tumor were serially sectioned into 5 µm thickness and stained with hematoxylin & eosin. Stained sections were reviewed to assess the histologic grade according to the Elston and Ellis grading system (18).
Nottingham Prognostic Index was calculated for each individual case taking into consideration the tumor size, lymph node status, and histologic grade. Nottingham Prognostic Index was calculated as follows: NPI = tumor size in cm × 0.2 + histologic grade (1-3) + lymph node status (1-3) (1 = 0 lymph nodes, 2 = 1-3 lymph nodes, 3 = ≥4 lymph nodes).
According to the score value, the cases were stratified into one of 4 prognostic groups where the higher the value, the worse the prognosis: excellent, NPI score <2.41; good, NPI score <3.41; moderate, NPI score 3.41-5.4; poor, NPI score >5.4 (19).
Immunohistochemistry
Estrogen receptor, PR, and HER2 immunohistochemical stained slides (immunohistochemical assay for all was from Dako Denmark A/S, Glostrup) of the studied cases were retrieved from Pathology Department archives for reevaluation and confirmation of scoring recorded. Then, cases were broadly classified according to these markers’ scores into 3 groups: luminal group (ER-positive, PR-positive or negative, HER2-positive or negative), HER2-positive group (ER-negative, PR-negative, HER2-positive), and triple-negative group (ER-negative, PR-negative, HER2-negative) according to Prat et al (20).
For CD74 immunohistochemical staining, 3-mm sections from primary tumors were deparaffinized in xylene for 30 minutes and rehydrated with a graded alcohol series. Sections were then subjected to antigen retrieval in 10 mM citrate buffer, pH 6.0 (Lab Vision Catalogue #AP-9003, Fremont, CA, USA) in a pressure cooker for 10 minutes followed by cooling at room temperature for 20 minutes and rinsing with phosphate-buffered saline (PBS) for 1 minute. Endogenous peroxidase was blocked by immersion of the sections in 3% hydrogen peroxide solution for 10 minutes, then washing them in PBS. Immunohistochemical staining was performed using the Lab Vision's UltraVision Detection Kit (TP-015-HD) according to the manufacturer's protocol. Sections were incubated for 10 minutes with Ultra V block to prevent nonspecific background staining. Then, sections were rinsed is PBS followed by an overnight incubation in a humidity chamber with mouse monoclonal antibody against CD74 (Lab Vision Catalogue #MS-131-R7 ready to use), then washing in PBS. Sections were then covered with 4-5 drops of UltraVision biotinylated goat anti-polyvalent secondary antibody, incubated at room temperature for 10 minutes, then washed in PBS, followed by incubation with streptavidin peroxidase solution for 10 minutes at room temperature, then rinsing with PBS. Sections were then covered for 15 minutes by adding 1 drop of 3-30-diamino-benzidine-tetrahydrochloride (DAB) chromogen mixed with 2 mL of DAB substrate. Finally, sections were counterstained with Mayer's hematoxylin, dehydrated in alcohol, and mounted in distyrene, plasticizer, and xylene. Sections of lymph node were used as positive control for CD74. Negative controls had primary antibody replaced by buffer.
Immunohistochemical evaluation
CD74 expression was scored for pattern of distribution: negative, <1% of tumor cells were labeled; focal, 1%-25% of tumor cells were labeled; diffuse, >25% of tumor cells were labeled and intensity (scale of +1 to +4). Only the carcinoma cells were considered for assessment of CD74 expression (4). Conventional H scoring was obtained by multiplying percentage of positive cells by the factor representing the intensity of staining (21).
Statistical analysis
The difference in studied marker expression among different studied tumor groups was statistically analyzed using SPSS (Chicago, IL) software statistical computer package version 15. Scores are expressed as mean ± SD. The difference in frequency was statistically analyzed using chi-square testing; comparing means of CD74 H-score and NPI among more than 2 different groups was carried out using analysis of variance (ANOVA); post hoc Tukey test was used for comparing 2 groups; and Spearman rank correlation coefficient was used to assess if there was a correlation between CD74 expression scores and NPI score in studied cases. A probability value of less than 0.05 was considered statistically significant.
Results
The present study included 160 specimens of invasive breast carcinoma. Forty cases (25%) were classified as luminal group (Fig. 1), 72 cases (45%) were classified as HER2-positive group (Fig. 2), and the remaining 48 cases (30%) were classified as triple-negative group (Fig. 3).
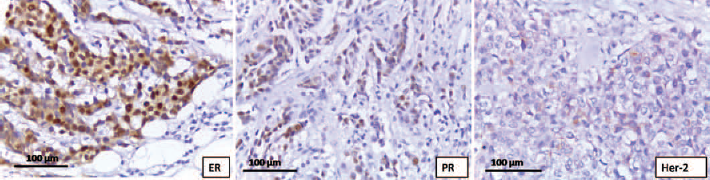
A case from the luminal group shows positivity to estrogen receptor (ER) and progesterone receptor (PR) receptors and negativity to human epidermal growth factor receptor 2 (HER2) (immunoperoxidase ×400).
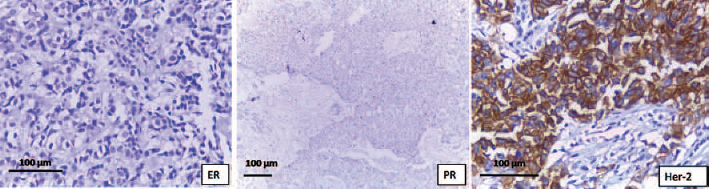
A case from the human epidermal growth factor receptor 2 (HER2)-positive group shows negativity to estrogen receptor (ER) and progesterone receptor (PR) receptors and positivity to HER2 (immunoperoxidase (400 [ER, HER2] and 4100 [PR]).
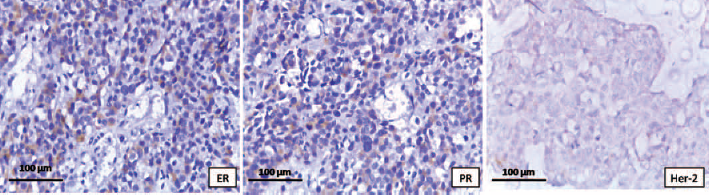
A case from the triple-negative group shows negativity to estrogen receptor (ER) and progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) (immunoperoxidase ×400).
Table I demonstrates distribution of cases in each studied tumor group as regards the different studied clinicopathologic parameters. Taking into consideration the clinicopathologic data, NPI for each individual case was calculated. Accordingly, studied cases were stratified into 3 prognostic groups: 5 cases (3.1%) had NPI ranging from 2.41-3.41 and these were categorized as good prognostic group, 72 cases (45%) had NPI ranging from 3.41-5.4 and these were categorized as moderate prognostic group, and 83 (51.9%) cases had NPI more than 5.4 and these were categorized as poor prognostic group.
Clinicopathologic variables in different studied groups
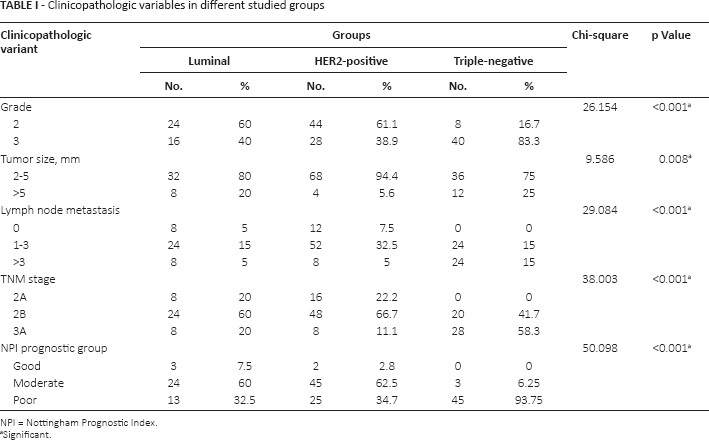
NPI = Nottingham Prognostic Index.
Significant.
CD74 immunohistochemical expression
CD74 was expressed mostly as brown granular cytoplasmic staining that was diffuse and/or perinuclear in tumor epithelial cells. Cell surface expression was observed in some cells as well (Fig. 4).
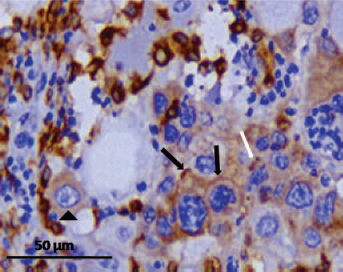
A case of invasive breast carcinoma from the triple-negative group shows moderate membranous (black arrows), diffuse cytoplasmic (arrowhead), and perinuclear (white arrows) CD74 staining in tumor cells (immunoperoxidase g1,000).
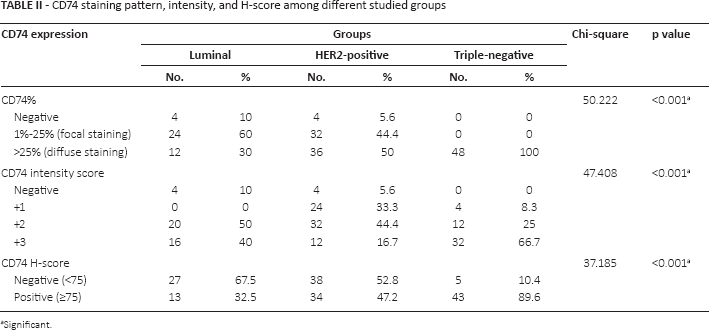
As regards CD74 pattern of staining, 8 cases (5%) were negative, 56 cases (35%) showed focal expression, and the remaining 96 (60%) cases showed diffuse expression (Fig. 5). CD74 pattern frequencies varied significantly among different studied groups (p<0.001). Of the 152 cases that expressed CD74, 28 (17.5%) showed mild (+1) intensity, 64 (40%) showed moderate (+2) intensity, and 60 (37.5%) cases showed intense (+3) staining (Fig. 6). The frequency of CD74 different intensities also varied significantly among different studied groups (p<0.001). On combining both intensity and percentage of stained cells into H-score, 70 cases (43.75%) had H-score less than 75 and considered as negative and 80 cases (56.25%) had H-scores equal to or more than 75 and were considered as positive. The frequency of CD74 H-score negativity and positivity was significantly different among different studied groups (p<0.001). Table II demonstrates the distribution of cases in different studied groups as regards CD74 pattern, intensity, and H-score.
CD74 staining pattern, intensity, and H-score among different studied groups
Significant.
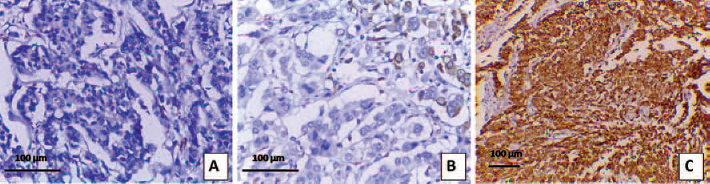
Different cases of invasive breast carcinoma show negative (
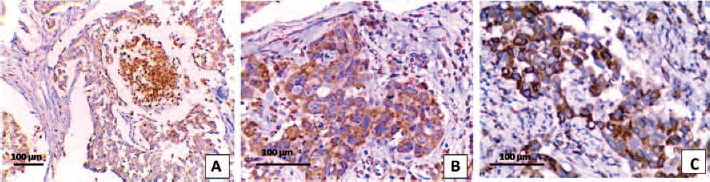
Different cases of invasive breast carcinoma show different intensities of CD74 expression: mild (
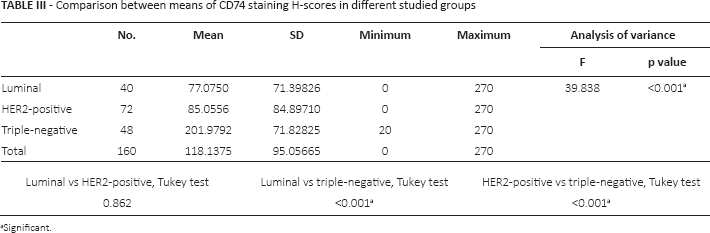
On performing ANOVA (Tab. III) to compare between means of CD74 H-scores in different studied groups, the difference was of high statistical significance (p<0.001) with significantly higher scores in the triple-negative group (201.98 ± 71.83) when compared to luminal (77.08 ± 71.39) and HER2-positive (85.06 ± 84.89) groups (p<0.001 for both) and the latter 2 groups did not differ significantly in their H-scores (p = 0.862) as evidenced by the post hoc test.
Comparison between means of CD74 staining H-scores in different studied groups
Significant.
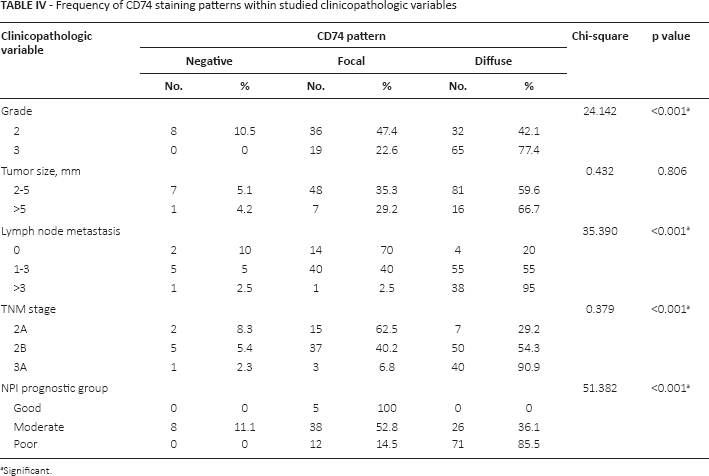
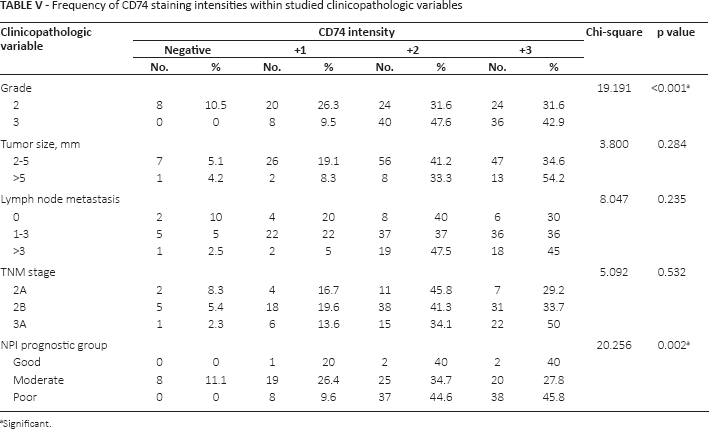
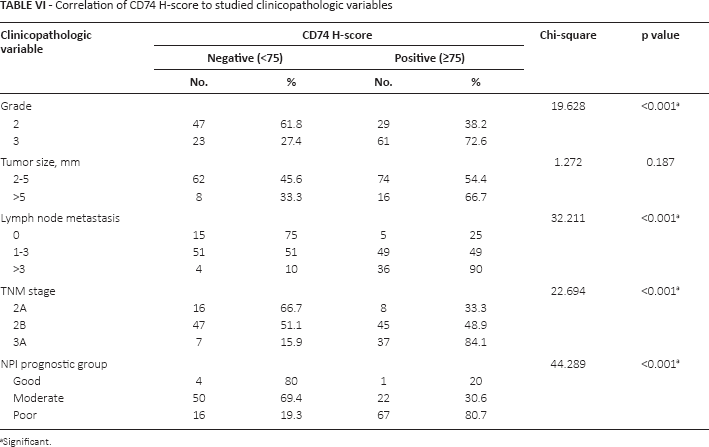
On studying frequency of CD74 expression patterns in different clinicopathologic parameters, a significant difference was present with tumor grade, lymph node metastasis status, TNM stage, and NPI grouping, but not with tumor size (Tab. IV). On the other hand, frequency of CD74 different intensities varied significantly with tumor grade and NPI grouping only but not with other clinicopathologic parameters, as demonstrated in Table V. CD74 H-score categories showed significantly different frequencies with all studied clinicopathologic parameters except for tumor size (Tab. VI).
Frequency of CD74 staining patterns within studied clinicopathologic variables
Significant.
Frequency of CD74 staining intensities within studied clinicopathologic variables
Significant.
Correlation of CD74 H-score to studied clinicopathologic variables
Significant.
On performing Spearman rank correlation coefficient to compare between CD74 expression and NPI scores, it was found that there is a significant positive correlation between CD74 intensity of staining, percentage of stained cells, H-scores, and NPI score (r = 0.253, 0.547, 0.501 and p = 0.01, <0.001, <0.001, respectively); thus the higher CD74 expression the higher the NPI score and consequently the worse the expected prognosis. The correlation between CD74 expression and NPI score is demonstrated in the graphs of Figure 7.
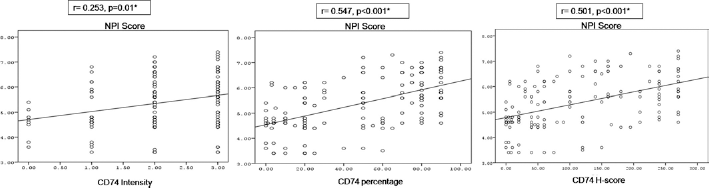
Scattergraph demonstrates the positive correlation among CD74 expression intensity, percentage of stained cells, H-scores, and Nottingham Prognostic Index (NPI) scores in studied cases.
Discussion
Prognostic factors can be used to distinguish patients likely to have recurrences after treatment of their primary tumor from those with low risk of recurrence, and those likely to benefit from adjuvant therapy from those whose disease is likely to be resistant to treatment. So, these factors influence the layout, direction, and analysis of clinical trials of breast cancer (22). The statuses of ER, PR, and HER2 are critical in the management of patients with invasive breast carcinoma (23). In patients whose tumors show no expression of ER and PR, any form of endocrine therapy is considered ineffective, and trastuzumab is not considered in those whose tumors exhibit less than 2+ staining of HER2 (24).
This study included 160 cases of invasive breast carcinoma that were classified according to their ER, PR, and HER2 immunohistochemical expression. Twenty-five percent of the studied cases were designated as luminal group, 45% designated as HER2-positive group, and the remaining 30% of cases designated as triple-negative group.
Tumor grade and size, which have a significant prognostic value in the luminal/ER-positive classes, show a limited prognostic power in HER2-positive and basal-like tumors. Thus, clinicopathologic prognostic factors behave differently in the different molecular subclasses (25, 26).
Accordingly, Rakha et al (27) reported that enhanced tailoring of treatment for breast carcinoma needs integration of clinical, pathologic, and cancer biological information to make sure that all known variables that could potentially control patient outcome and response to therapeutic treatments are considered. Subsequently, there has been increasing interest in the clinical utility of NPI, which is based on a combination of histopathologic examination of tumor size, lymph node stage, and tumor grading assembled in a prognostic index formula.
In this study, data about the real outcome of patients included in this study were missing as the blocks were from archives, in which the cases did not receive neoadjuvant chemotherapy before surgery. Thus we depended on the expected outcome of cases using NPI that classified cases into different prognostic groups. Most triple-negative group cases (93.75%) had high NPI and were considered of poor prognosis and the remaining cases of this group (6.25%) were of moderate prognosis. In the HER2-positive group, 34.7% of cases had high NPI and were considered of poor prognosis, 62.5% of cases had lower NPI and were considered of moderate prognosis, and the remaining 2.8% only had the lowest NPI and were considered of good prognosis. As regards the luminal group, 32.5% of cases had high NPI and considered of poor prognosis, 60% of cases had lower NPI and were of moderate prognosis, and 7.5% of cases had much lower NPI and were considered of good prognosis.
Dunkler et al (28) reported that the use of a formula like NPI not only overcomes problems associated with the variable prognostic power of each individual clinicopathologic factor in the different molecular classes but also provides a way of incorporating biological and clinical variables in a scientifically and clinically relevant way. Soria et al (29) added that the biological characteristics of breast carcinoma and incorporation into the NPI could significantly improve the delivery of personalized medicine in breast carcinoma patients. Baker et al (30) found a significant correlation between the expected outcome as determined by NPI and the real outcome. Meteoglu et al (31) also reported that high PR positivity had a meaningful correlation with low NPI values. These findings explain why we stratified cases of this study according to their NPI.
The tendency of having poor prognosis in this study was significantly more frequent in triple-negative (93.75% of cases) than HER2-positive (34.7% of cases) and luminal groups (32.5% of cases). This finding signifies the urgent requirement to search for and identify novel prognostic biomarkers for such group and this is consistent with what was reported by others (32).
CD74, the γ subunit of MHC class II, is frequently overexpressed in malignant tumors of epithelial and mesenchymal origin (33). The CD74 expression in this study was detected mostly as granular cytoplasmic staining that was diffuse and/or perinuclear in tumor epithelial cells, with cell-surface expression observed in some cases as well. Similar staining pattern of expression was reported in gastrointestinal cancers by Gold et al (4). This finding is in contrast to hematologic tumors that show CD74 cell-surface expression as reported by Burton et al (5) and Starlets et al (34).
Gold et al (4) explained the variable expression of CD74 by the fact that their study, like ours, “evaluated a static presentation of antigen rather than a dynamic, time-dependent, profile.” They added that CD74 is possibly present within the membrane of tumors with cytoplasmic expression at densities much less than the detection limits of the technologies employed or it is possible that this large intracellular aggregation of CD74 allows greater chance for maintenance of surface-expressed CD74 receptor at low amount.
In this study, CD74 immunohistochemical expression in tumor epithelial cells was evaluated as regards pattern, intensity of staining, and H-score. For pattern of staining, 34.4% and 60% of cases had focal and diffuse CD74 staining, respectively, while only 5% of cases were negative. All cases in the triple-negative group of this study showed diffuse staining. In the HER2-positive group, 5.6%, 44.4%, and 50% of cases showed negative, focal, and diffuse staining, respectively. The luminal group showed negative, focal, and diffuse staining in 10%, 60%, and 30%, respectively. The pattern of CD74 staining varied significantly among different studied groups with tendency of diffuse expression to be higher in the triple-negative group than the HER2-positive and luminal groups.
These findings are similar to that of Tian et al (1), who also reported that CD74 was located in the cytoplasm and membrane of breast cancer cases of their study. They studied the pattern of expression and found that it related significantly to triple negativity of breast cancer.
As regards CD74 intensity of staining in this study, 17.5% of cases showed mild staining, 40% of cases showed moderate staining, and 37.5% of cases showed intense staining. The triple-negative cases showed intense, moderate, and mild staining in 66.7%, 25%, and 8.3% of cases, respectively. The HER2-positive group cases showed intense, moderate, and mild staining in 16.7%, 44%, and 33.3% of cases, respectively. The luminal group cases showed intense and moderate staining in 40% and 50% of cases, respectively. The frequency of different CD74 expression intensities varied significantly between groups (p<0.001), with highest frequency of intense expression observed in the triple-negative group.
On calculating H-score of CD74 expression in studied cases by combining intensity of staining and percentage of stained cells, cases were finally categorized into negative cases (43.75%) with CD74 H-score less than 75 and into positive cases (56.25%) with CD74 H-score more than or equal to 75. The frequency of cases in these 2 categories varied significantly among different studied groups with highest frequency of positivity observed in the triple-negative group (89.6% of cases).
Greenwood et al (35) reported that CD74 was consistently expressed in the triple-negative subgroup of breast cancer in their study and correlated with clinicopathologic and immunohistochemical characteristics.
In this study, CD74 pattern of expression and H-score correlated significantly with the presence of lymph node metastasis (p<0.001 for both). This finding is similar to others who reported that CD74 overexpression is linked to increased invasion and metastasis of breast tumors, particularly tumors of the triple-negative phenotype (1, 33, 36).
In this study, neither CD74 pattern nor intensity of expression nor H-score showed significant correlation with tumor size (p = 0.806, 0.284, 0.187, respectively), similar to Tian et al (1).
Our study shows that CD74 pattern, intensity of staining, and H-score correlated significantly to NPI score as demonstrated by differences in frequency of expression in different prognostic groups and by Spearmen rank correlation coefficient, where the higher the CD74 expression, the higher the NPI and thus the poorer the expected prognosis. This finding is consistent with that reported by Tian et al (1); survival analysis in their study revealed that patients with CD74 expression experienced worse postoperative survival compared to those without CD74 expression.
Others have also suggested an association between CD74 expression and tumor behavior and added that this may correlate with prognosis (37-38-39). Gold et al (4) reported that the presentation of tumor antigens by MHC II may be impossible by increased CD74 expression with an eventual decrease of tumor immunogenicity. They added that more effective MHC II peptide-binding cleft blocking can be provided by high intracellular concentrations of CD74 that will prevent uptake of endogenous tumor-related peptides and presentation of immunogen to CD4+ T cells. Other studies have also suggested another important role for the CD74 molecule in catalyzing cell survival pathways including the ERK-1/2 MAP kinase signaling cascade and inducing cell proliferation by increasing cyclins and expression of other regulatory factors (40, 41).
In accordance with these findings, this study shows that CD74 expression pattern and H-score varied significantly (p<0.001 for both) among different studied tumor stages where tumors of higher stages show higher frequencies of increased CD47 expression. These findings are in contrast to Tian et al (1), who found that the correlation between CD74 and tumor stage was of no significance.
CD74 expression is also linked with several forms of cancer (15, 42-43-44-45-46-47-48). Zhang et al (42) found that CD74 overexpression in pancreatic ductal adenocarcinoma patients was associated with poor prognosis even if curative resection was done. They concluded that CD74 can be used as a prognostic indicator for resectable pancreatic ductal adenocarcinoma. Moreover, a study carried out by Otterstrom et al (49) revealed that high expression levels of CD74 have positive correlation to poor prognosis in mesothelioma.
Borghese and Clanchy (50) outlined the role of CD74 signaling in carcinogenic processes and its use as a therapeutic target in cancer. The upregulation of CD74 in gastric carcinoma was found to be associated with increasing clinical stage and provided an opportunity as novel gastric cancer chemoprevention and/or treatment strategy (51). Cheng et al (52) reported that CD74 overexpression in thyroid cancer is associated with advanced tumor stage and may serve as a therapeutic target. Some studies have demonstrated that CD74 suppression can transform tumor cells into potent vaccines. The MHC II molecules can bind and present endogenous peptides as immunogenic tumor antigens in the absence of the CD74 chaperone, and this can be used in cancer immunotherapy (53, 54).
In summary, this study shows that CD74 immunohistochemical expression in invasive breast carcinoma was significantly higher in triple-negative tumors, higher tumor grade, presence of lymph node metastasis, higher tumor stage, and higher NPI score. These findings indicate that CD74 might be considered as a useful prognostic indicator predicting poor outcome of patients with invasive breast carcinoma and its expression on malignant cells especially in the triple-negative group suggest CD74 as a potential therapeutic target worthy to be studied further in such cancers. Few studies have worked on evaluation of CD74 expression in breast carcinoma with its different molecular and prognostic subclasses. Consequently, effort should be focused on understanding the clinical significance of this marker aiming at optimal utilization of available therapies and development of novel therapies based on improved cancer models.
Footnotes
Acknowledgment
Authors greatly appreciate the support of Prof. Dr. Hussein Zaki Ghoraba and Dr. Mohamed Elrashidy during delivering this work.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.
Meeting presentation: This work has been accepted as poster presentation in the XXXI International Congress of the International Academy of Pathology and the 28th Congress of the European Society of Pathology that will be held, from 25 September to 29 September 2016, in the KölnMesse in Cologne, Germany.