
Abstract
Purpose
To explore the efficacy and toxicity of an extended schedule of temozolomide (50 mg/mq 1 week on/1 week off) in a population of newly diagnosed low-grade gliomas (LGG).
Methods
Primary endpoints were progression-free survival (PFS) at 12 and 24 months and response rate evaluated with Response Assessment in Neuro-Oncology Criteria. Secondary endpoints were clinical benefit (reduction of seizures frequency), reduction of steroid, and modifications of Karnofsky Performance Status.
Results
From 2006 to 2009, we enrolled 14 consecutive patients with newly diagnosed LGG: 8 grade II astrocytomas, 2 oligodendroglioma, and 4 oligo-astrocytoma. Temozolomide was administered for 18 cycles (mean) per patient (range 3-24 cycles). In 57.5% (n = 8), we observed stable disease, 28.5% (n = 4) presented a minor response, and 14% (n = 2) showed progression. Five patients presented early progression during the first year of treatment and the study was stopped. A relevant clinical benefit was observed in 85% of patients (seizure control). After 6 years of follow-up, only 4 patients died. Prolonged PFS was associated with 1p-19q codeletion over 1p-19q intact (35 vs 4 months; p<0.04) and IDH1 mutation over IDH1 wild-type (36 vs 6 months; p<0.009).
Conclusions
The study was interrupted for the high rate of progression observed in the first 14 patients enrolled. However, our results show that an extended low dose of temozolomide presents interesting activity with objective response and clinical benefit, but does not seem to prevent progression in patients presenting unfavorable molecular prognostic factors.
Introduction
Diffuse low-grade gliomas (LGG) represent a heterogeneous group of slow-growing tumors with different clinical, histologic, and molecular characteristics. In adults, the majority of LGGs are WHO Grade II astrocytomas and oligodendrogliomas, which differ in molecular fingerprints and median survival, but share a propensity to malignant transformation after a number of years (1).
Surgical resection is considered the first treatment option, whenever possible (2, 3), although the optimal treatment of patients with LGG is controversial (4).
The role of extent of resection has never been proven to improve the outcome. Patients older than age 40 with unresectable large tumors and/or with neurologic deficits are considered to be at high risk of recurrence or progression and are usually treated with radiation therapy (5). A substantial incidence of radiation-induced cognitive deficits has been described in LGG patients who received whole-brain or focal radiotherapy (RT) and emerging data in the literature suggest that potential late neurotoxic effects should be considered in the timing of RT (6-7-8-9-10-11). Treatment selection in young patients with small asymptomatic, unresectable, or partially resected LGG is not easy (11).
Recently, several studies have reported the efficacy of chemotherapy in children and adults with newly diagnosed or recurrent LGG treated with different chemotherapeutic agents (12-13-14-15), showing high percentage of radiologic objective response or prolonged disease stabilization. The role of chemotherapy also is being evaluated in a multicentric European trial (European Organization for Research and Treatment of Cancer 22033) that compares 50.4 Gy RT with up-front temozolomide (TMZ) in previously untreated LGG. Preliminary results suggest that TMZ is well-tolerated and probably as effective as RT in a subgroup of LGG patients with chromosomal 1p deletion (16).
The role of chemotherapy in the treatment of LGG needs to be better defined, but some authors have suggested that TMZ may represent an interesting alternative to early RT after brain surgery, particularly in patients with favorable prognostic factors (16-17-18-19-20-21-22-23-24-25-26).
Also, various authors reported that chemotherapy in LGG may induce an important clinical benefit with control of symptoms, including epilepsy, and a good influence on quality of life (22, 26).
Previous studies have shown chemotherapy activity particularly in pure oligodendrogliomas and mixed oligo-astrocytomas (15, 17), even if better results have been observed in anaplastic oligodendrogliomas (18).
Available literature data (19, 27) show that adult LGG seems to be less chemosensitive than anaplastic forms, but even that chemotherapy activity may induce important clinical benefits.
The long-term results of a phase 3 Radiation Therapy Oncology Group (RTOG) trial evaluating patients with grade 2 glioma treated with radiation therapy plus PCV chemotherapy versus patients who received radiation therapy alone show a substantial survival advantage with PCV adjuvant chemotherapy (28).
Several phase II studies show a significant activity of TMZ chemotherapy with standard schedule in LGG (15, 16). Different schedules of TMZ administration, including extended and continuous schedules, have been investigated in various studies (20-21-22). Kesari et al (25) suggest that a protracted administration of daily TMZ is a well-tolerated regimen and seems to produce effective tumor control.
The LGG growth process is characterized by a slow expansion with a growth rate less than 1%-3% (22, 23) and this is considered as a resistance factor for cytotoxic radiotherapeutic and chemotherapeutic treatments. More recently, the hypothesis has been proposed that LGG biological features could make these tumors more sensitive to a chronic chemotherapeutic drugs exposition rather than fractioned elevated doses, which are most useful in the treatment of tumors that exhibit elevated mitotic index (24). Preliminary experiences with TMZ utilized with continuing schedule in anaplastic gliomas have demonstrated good tolerability with lower hematologic toxicity than that observed in standard schedule TMZ treatment (200 mg/mq for 5 consecutive days every 28 days) (22). Recent advances in gene expression profiling are fundamentally changing the management of LGG. Both prognosis and response to treatment, particularly to TMZ chemotherapy, have been reported to be significantly related on genetic or molecular characteristics such as 1p/19q chromosomal codeletion, p53 mutation, and IDH mutations (29-30-31).
The combination of IDH1 mutation and 1p/19q codeletion may be particularly effective in discriminating good prognosis and response to chemotherapy in adult LGG (32-33-34).
The role of IDH1 mutation as a strong predictor of survival in LGG has been reported in several studies (35, 36).
The aim of our study was to explore the efficacy and toxicity of low-dose extended-schedule administration of TMZ (50 mg/mq 1 week on/1 week off) in a population of newly diagnosed LGGs.
Methods
This is a prospective, phase II, open-label study.
From 2006 to 2009, we prospectively enrolled patients with newly diagnosed LGG (astrocytoma WHO grade II gemistocytic, fibrillary, and protoplasmatic; oligoastrocytoma WHO grade II; or oligodendroglioma WHO II) requiring treatment for the presence of at least one of the following negative prognostic factors: residual tumor after surgery or biopsy, age older than 40 years, neurologic deficits, or uncontrolled epilepsy.
We enrolled patients with age ≥18 years. Prior RT was admitted if it was completed at least 8 weeks before the enrollment.
Measurable disease on pretreatment contrast-enhanced magnetic resonance imaging (MRI), adequate hematologic, renal, and hepatic function, and a Karnofsky Performance Status (KPS) ≥60 were also required. Exclusion criteria were recurrent/progressive LGG with histologic or radiologic signs of anaplastic progression with enhancing areas at MRI brain scan. No previous chemotherapy was admitted.
The primary endpoints were progression-free survival (PFS) at 12 and 24 months and response rate (complete response [CR], partial response [PR], stable disease [SD]) evaluated with Response Assessment in Neuro-Oncology (RANO) criteria (37).
The secondary endpoints were clinical benefit evaluated by measuring reduction in frequency of seizures per month, reduction in steroid dose, and modifications of KPS.
Clinical and radiologic evaluation with MRI was performed at baseline and every 3 treatment cycles.
This study was approved by our institutional ethical committee and all patients were required to sign informed consent. Registration: EUDRACT 2006-001545-34.
Tumor response criteria
Progression-free survival at 12 and 24 months was defined as the time from the start of therapy to disease progression.
For response assessment (CR, PR, SD, minor response [MR]) we utilized the RANO criteria (37).
Clinical benefit was evaluated assessing neurologic function, seizure control, and steroid dosage. Seizure control was defined as partial seizure control (PSC), reduction of >50% in the number of seizures, with the steroid dose stable or reduced, and no modification of anticonvulsant treatment; or complete seizure control (CSC), absence of seizures in patients presenting uncontrolled epilepsy before the treatment (38).
Molecular profile
In all patients, we considered deletion status 1p/19q (yes/no/unknown), IDH1 mutation status (yes/no/unknown), and MGMT status (methylated/unmethylated/unknown). The molecular status was correlated with PFS and response rate.
Treatment plan
We utilized a low dose of TMZ (50 mg/mq/day) given 1 week on/1 week off until progression or for a maximum of 24 months.
Statistical analysis
Sample size justification
This phase II trial was planned as a single-stage design as described by A'Hern (39). A sample size of 45 patients was considered sufficient to give a 90% probability of rejecting a response rate of 60% with an exact 5% significance test when the true response rate is 80%. The drug regimen will be rejected if fewer than 33 responses (as previously defined) are observed.
Statistics
Standard summary statistics were used for both continuous and discrete variables. The objective response rate was reported with its 95% confidence interval. The time to event analysis was performed according to the Kaplan-Meier method and curves were compared using the log-rank test.
Results
Patients
From 2006 to 2009, we enrolled 14 consecutive patients with newly diagnosed LGG with different histology: 8 grade II astrocytomas, 2 oligodendroglioma, and 4 oligo-astrocytoma. Patient characteristics are described in Table I. The age of patients ranged from 18 to 75 years, with a median of 44 years.
Demographic and clinical features of patients
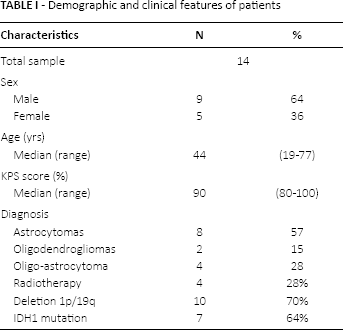
The median KPS was between 80 and 100. Four patients underwent RT before enrollment. Temozolomide was administered for a mean of 18 cycles per patient (range 3-24 cycles). A total of 251 cycles of chemotherapy were administered.
The FISH analysis for detection of 1p-19q deletion status was obtained in 12 patients: 10 (71%) patients presented a 1p-19q codeletion; 2 patients presented no deletion.
IDH1 mutation was assessed in 11 patients: in 7 patients, IDH1 was mutated, while IDH1 was wild-type in 4.
MGMT methylation status analysis was performed in 6 patients, resulting methylated in 4 and unmethylated in 2.
Response rate and follow-up data
In 57.5% (n = 8), we observed SD at MRI scan, 28.5% (n = 4) presented MR, and 14% (n = 2) showed PD. In patients receiving radiation treatment before the start of chemotherapy, a possible influence on radiologic response cannot be ruled out. However, among the 4 patients receiving RT before TMZ, 2 showed early progression and 2 were stable.
A disease control rate (SD plus MR) was obtained in 86% of patients. The PFS at 12 months was 71%, with a mean follow-up of 54 months; median PFS is 36 months. We observed an early progression during treatment in 5 patients with PFS of 7.8 months (interval 3-12 months). Considering the high rate of early progression, the enrollment was stopped.
Out of the 5 patients presenting early progression, 2 showed no 1p-19q deletion and no IDH1 mutation, 1 presented 1p deletion, and in the other 2, the molecular analysis was not obtained.
Long-term follow-up
After 6 years of follow-up, only 4 patients died. Out of 11 patients surviving, 4 are free of progression and all of them presented 1p-19q codeletion and IDH1 mutation. Among the 4 patients who died, 2 presented 1p-19q intact and IDH1 wild-type.
In the subgroup analysis of PFS according to IDH1mutation status, patients with tumoral IDH1mutations and 1p-19q deletion showed significantly longer PFS than did those without the mutation, regardless of histology.
Figure 1 reports the median PFS for 1p-19q deletion status (1p-19q codeleted = 35 months; 1p-19q intact = 5 months; p<0.04). Figure 2 reports the median of PFS for IDH1 mutation status (IDH1 mutated = 36 months; IDH1 wild-type = 6 months; p<0.009).

Median progression-free survival for 1p-19q deletion status.
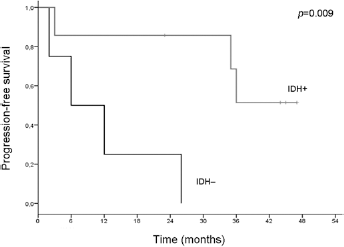
Median progression-free survival for IDH1 mutation status.
Clinical benefit and toxicity
The influence of TMZ treatment on seizure frequency was relevant. In almost all patients presenting epilepsy before treatment (n = 7), we observed a reduction in or complete control of seizures: 2 patients were epilepsy-free (CSC), 4 patients presented a reduction of epileptic seizures (PSC), and 1 patient presented stable frequency of seizures. In all patients, the steroid dose was stable or reduced and no modification in anticonvulsant treatment medication was necessary.
We did not observe significant modification of KPS during TMZ treatment with respect to baseline values. In this study, no gastrointestinal or hematologic toxicity more than grade 3 was observed. A grade 2 lymphopenia was noted in 5 patients (35%).
Discussion
Considering the high early progression rate and the statistical design of the study, this trial did not reach the primary endpoint and was interrupted after the enrollment of 14 patients.
However, our results show that continuous administration of a low dose of TMZ presents interesting activity with objective response and clinical benefit, but does not seem to prevent early progression in the treatment of newly diagnosed LGG requiring treatment, particularly in patients presenting unfavorable molecular prognostic factors.
It has been suggested that indolent gliomas with low mitotic index may be treated with extended schedules of administration of TMZ with chronic low-dose exposure (25). Several studies have investigated different types of continuous dosing schedules (23-24-25) in malignant gliomas with the aim to increase the dose intensity. As low-grade tumors have a limited number of cells in the proliferation phase, the investigation of a drug in a more continuous administration is theoretically attractive. At present, there are no data in the literature exploring the activity of continual low-dose chemotherapy in newly diagnosed low-grade astrocytomas.
In our study, a low-dose schedule of TMZ every other week showed interesting activity, producing an objective response in 4 patients (28.5%) with MR at MRI scan, SD in 8 patients (57.5%), and relevant control of seizures in 6 (43%).
In patients receiving radiation treatment before the start of chemotherapy, a possible influence on radiologic response cannot be ruled out. However, among the 4 patients receiving RT before TMZ, 2 showed early progression and 2 were stable.
Recent data show significant activity of TMZ chemotherapy with standard schedule in LGG (20-21-22). However, most published series exploring the activity of TMZ in LGG include both newly diagnosed and progressive LGG, often presenting enhancing areas on MRI. In our study, we have included only newly diagnosed LGG with no signs of radiologic progression at MRI scan. Several studies showed that chemotherapy may induce long-term stabilization of the disease and important clinical benefit, including control of epilepsy (15, 26).
The occurrence of seizures negatively influences quality of life and contributes to cognitive impairment in patients with LGG (40-41-42). Also, more than 30% of patients with LGG will not become seizure-free despite treatment with often multiple antiepileptic drugs (AEDs) (43).
Koekkoek et al (26) recently observed that 44% of patients with LGG with uncontrolled epilepsy show a ≥50% seizure reduction after treatment with TMZ. In addition, we found that a reduction in seizure frequency after the start of TMZ appears to be a favorable independent prognostic factor of PFS and overall survival in patients with LGG with epilepsy. In a previous study by our group (22), we observed a ≥50% seizure reduction in 49% of patients with uncontrolled epilepsy treated with TMZ, and Kaloshi et al (34) demonstrated a ≥50% seizure reduction in 58% of patients with LGG. The effect of TMZ on seizure reduction is unclear. A direct pharmacologic effect of TMZ on seizures could be one of the mechanisms of action. de Groot et al (43) observed that TMZ reduces the intrinsic epileptogenicity of the tumor through a decrease in glutamate levels released from glioma cells. Furthermore, a downregulation of glutamate receptors is associated with a reduction in the risk of seizures as well as with increased survival in glioma patients treated with adjuvant TMZ (44). Changes in the peritumoral microenvironment might also be induced, for example, through an inhibition of the immune response or restoring the neurotransmitter synthesis (45, 46).
In the present study, we observed an improvement in seizure frequency during TMZ treatment with no change in AED in all patients. A total of 64% (9/14) of patients became seizure-free during the treatment and 36% (5/14) of patients showed a reduction of epileptic attacks. This can suggest that seizure control could be better managed in LGG patients with an association between AED and TMZ.
In the small population of patients included in our study, the presence of IDH1 mutation and 1p/19q codeletion seems to confirm a significant predictive and prognostic factor. Among the 5 patients with early progression, 4 showed unfavorable molecular prognostic factors while, on the contrary, all patients surviving after 6 years of follow-up presented IDH1 mutation and 1p/19q codeletion. The results of our study need to be evaluated in the context of the controversial debate on the best treatment of LGG.
At present, on the basis of the results of the RTOG trial 9802 showing a major increase in survival after adjuvant PCV chemotherapy, this regimen should be considered the treatment of choice in high-risk LGGs requiring treatment (28, 47). However, several aspects remain to be clarified. First, the concept of high-risk LGG and the criteria for selecting patients requiring adjuvant treatment need to be better defined. Previous studies evaluating the role of chemotherapy in LGG utilized different criteria to define patients requiring treatment and often included patients with proven progressive tumors. Few trials included truly newly diagnosed nonprogressive tumors. Another important aspect concerns the choice of the best chemotherapy regimen. Considering the data showing the positive impact of PCV regimen on survival in grade III and II gliomas, the question is whether TMZ may be considered equally effective.
Temozolomide is an easier schedule of treatment and less toxic than PCV, and may allow prolonged period of treatment in slow-growing tumors. In clinical practice, many neuro-oncologists consider the PCV regimen too toxic, and use TMZ instead of PCV.
The results of our study indicate that an extended schedule of low dose of TMZ shows interesting activity with objective response and clinical benefit in patients with newly diagnosed LGG with favorable molecular factors. The role of continuous low-dose treatment with TMZ needs to be confirmed in this subgroup of LGG patients harboring positive prognostic factors. Also, new trials are needed to evaluate the most effective chemotherapy regimen in LGG.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.