
Abstract
Background/aims
Endoscopically detected tumor recurrence after curative total gastrectomy is very rare. We reviewed the clinicopathological and endoscopic findings together with the clinical outcomes of these patients.
Methods
Seventeen patients with recurrent gastric cancer detected by upper gastrointestinal endoscopy who underwent curative total gastrectomy between January 1990 and May 2011 at the Asan Medical Center were analyzed retrospectively.
Results
Of the 17 patients, 5 were resectable at the time of diagnosis of recurrence and 12 were unresectable. The median interval between total gastrectomy and diagnosis of recurrence was 20.2 months (interquartile range 12.4-42.1 months). The tumors were located in the anastomotic area in 8 patients, in the proximal part of the afferent or efferent loop in 7, and in the stump of the afferent loop in 2 patients. With regard to the endoscopic findings, a mass was found in 8 cases, an ulcer in 2, stricture in 4, and nodularities in 3. Operations were performed in 3 patients, chemotherapy in 10 (including 2 receiving adjuvant chemotherapy), and conservative management in 6. Fourteen patients died from progression of the disease and the median survival period from recurrence for all 17 patients was 5.3 months (interquartile range 1.2-7.7 months).
Conclusions
Local recurrence of gastric cancer detected by upper gastrointestinal endoscopy after curative total gastrectomy has a poor prognosis.
Introduction
Gastric cancer is one of the most common cancers, with about a million new cases per year worldwide (1). Although there have been great advances in its diagnosis and treatment, the prognosis is still dismal, especially in the more advanced stages (2). This is because more than half of the gastric cancers are diagnosed at an advanced stage and many of them recur in spite of curative surgery.
Tumors can recur after total gastrectomy due to remaining intramural tumor cells (R1 resection) at the esophagojejunal anastomosis or implantation of intraluminal tumor cells into the anastomosis (3). Locoregional tumor recurrence after R0 resection is not unusual and its incidence is reported to be as high as 11.3%-34.7% (4-5-6). However, few studies have focused on recurrent cancer detected by upper gastrointestinal endoscopy after curative total gastrectomy for gastric carcinoma and the relationship between clinicopathological factors and resectability after recurrence. Therefore, we aimed to evaluate the clinical outcomes and endoscopic findings of these patients. In addition, we compared findings in resectable and unresectable patients.
Patients and Methods
Patients
Between January 1996 and May 2011, 17 patients who had previously undergone curative total gastrectomy were diagnosed with local recurrence by upper gastrointestinal endoscopy in the Asan Medical Center, Seoul, Korea. All patients had histologically confirmed adenocarcinoma of the stomach at the initial diagnosis, without clinical or radiological evidence of distant metastasis, and underwent curative resection (R0) and D2 lymphadenectomy as the primary treatment. After total gastrectomy, the negative resection margins of the surgical specimen were identified by pathological examination. Based on the final pathology of the surgical specimens, adjuvant chemotherapy was performed in patients with a high risk of local relapse (stage T2 with histopathological risk factors, T3-4, positive lymph nodes). Standard postoperative adjuvant chemotherapy consisted of fluoropyrimidine-based regimens.
The tumors were divided into 2 groups on the basis of their histology: those with differentiated histology, which included papillary adenocarcinoma and well or moderately differentiated adenocarcinoma, versus those with undifferentiated histology, which included poorly or undifferentiated adenocarcinoma, signet-ring cell carcinoma, and mucinous carcinoma. The retrospective study protocol was approved by the Institutional Review Board of the Asan Medical Center (IRB number 2012-0052).
Follow-up schedule
As a routine process, follow-up schedules consisted of physical examination, laboratory tests, chest radiography, upper gastrointestinal endoscopy and abdominopelvic computed tomography (CT) at intervals ranging from 3 to 6 months during the first 2 years and 6 to 12 months thereafter. Especially with routine endoscopy, patients who underwent total gastrectomy were examined 6-12 months after the operation and annually thereafter until 5 years. Follow-up ended on December 31, 2014.
Definitions
Local recurrence of gastric cancer was diagnosed based on endoscopic findings suggestive of recurrence along with presence of a biopsy-proven tumor containing adenocarcinoma cells. The main endoscopic patterns of recurrence were divided into 4 groups as described previously by Lee et al (7): mass, ulcer, stricture, and nodularities (Fig. 1). The cancers were restaged according to the American Join Committee on Cancer (AJCC) tumor node metastasis (TNM) system, 7th edition. Resectability was decided based on clinical, radiological, and pathological exams if there was no evidence of distant metastasis.
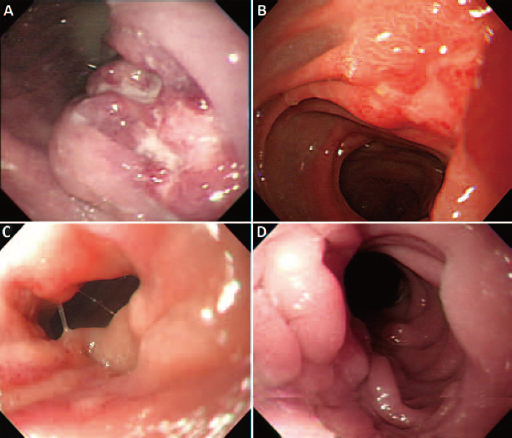
Endoscopic findings of local recurrence after curative total gastrectomy: mass (
Statistical analysis
Values are reported as medians with interquartile ranges (IQR). Differences between the study groups were calculated using the Mann-Whitney U-test for continuous variables and Fisher's exact probability test for categorical variables. The Kaplan-Meier method was used to estimate survival probability as a function of time. The threshold for significance was set at p<0.05. Statistical analyses were performed using SPSS Statistics v.18 for Windows.
Results
Baseline characteristics of the patients
The initial baseline characteristics of the study patients are shown in Table I. The median age was 52.0 years and 82.4% were male. Fifty-nine percent of the tumors were located in the upper third portion of the stomach and the median longest tumor diameter was 9.0 cm. The median distance of the tumor from the proximal margin was 1.5 cm (IQR 0.5-3.75 cm). All recurrent cases were advanced gastric cancers at initial diagnosis, and stage III was the most common (76.5%). Thirteen patients (76.5%) underwent adjuvant chemotherapy after total gastrectomy at the initial diagnosis of a gastric cancer. No patient underwent neoadjuvant chemotherapy. No patient underwent chemoradiation therapy.
Baseline characteristics of patients who underwent total gastrectomy for gastric cancer
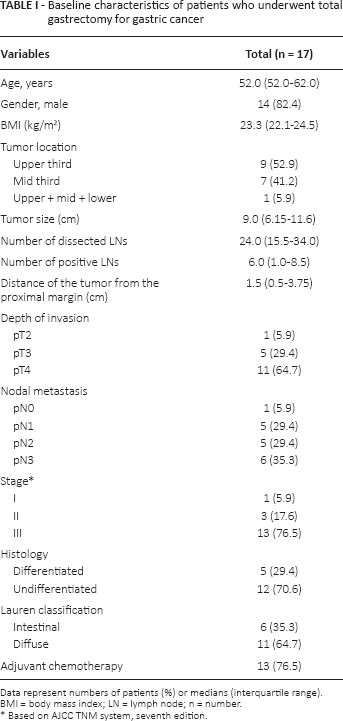
Data represent numbers of patients (%) or medians (interquartile range).
BMI = body mass index; LN = lymph node; n = number.
Based on AJCC TNM system, seventh edition.
Clinical and endoscopic findings
Among the 17 cases detected by upper endoscopy, 5 patients (29.4%) had only local recurrence whereas the other 12 patients had combined patterns with peritoneal seeding (17.6%), liver metastasis (23.5%), recurrence in the abdominal cavity such as colon, small bowel, and/or abdominal lymph nodes (23.5%), or malignant pleural effusion (5.9%). Seven patients (41.2%) were asymptomatic whereas 10 patients (58.8%) were symptomatic at the time of diagnosis of recurrence. In the symptomatic patients, the chief complaints were abdominal pain (40%), dysphagia (20%), nausea/vomiting (20%), general weakness (10%), and poor oral intake (10%).
The location of local recurrence involved the anastomotic area in 8 cases, the proximal part of the afferent or efferent loop in 7 cases, and the afferent loop stump in 2 cases (Tab. II). The endoscopic findings of the local recurrence (Fig. 1) were of a mass in 8 cases, a stricture in 4 cases, nodularities in 3 cases, and an ulcer in 2 cases. When the tumors were divided into resectable and unresectable, the site of local recurrence, endoscopic findings, tumor histology, time from gastrectomy to recurrence, and the number of esophagogastroduodenoscopies (EGDS) performed did not differ significantly between the 2 groups (Tab. II).
Clinicopathological factors in patients with recurrence after total gastrectomy according to resectability (n = 17)
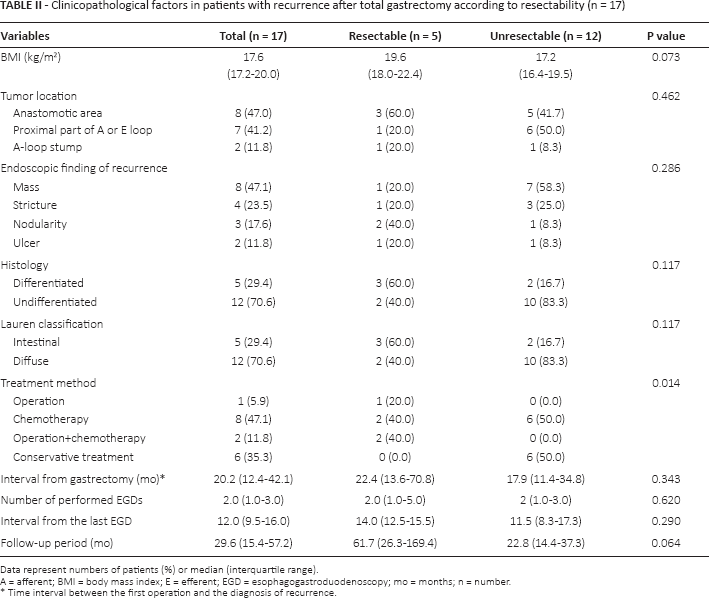
Data represent numbers of patients (%) or median (interquartile range).
A = afferent; BMI = body mass index; E = efferent; EGD = esophagogastroduodenoscopy; mo = months; n = number.
Time interval between the first operation and the diagnosis of recurrence.
Resectable recurrent gastric cancer detected by esophagogastroduodenoscopy after curative total gastrectomy
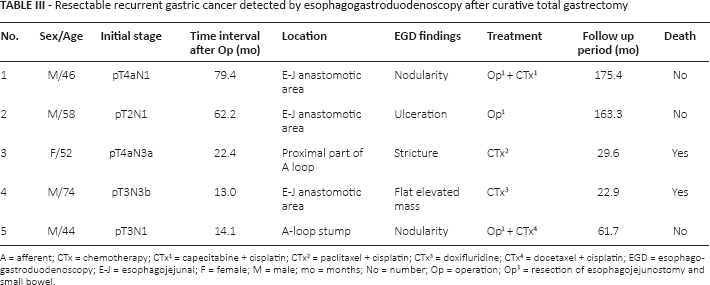
A = afferent; CTx = chemotherapy; CTx1 = capecitabine + cisplatin; CTx2 = paclitaxel + cisplatin; CTx3 = doxifluridine; CTx4 = docetaxel + cisplatin; EGD = esophagogastroduodenoscopy; E-J = esophagojejunal; F = female; M = male; mo = months; No = number; Op = operation; Op1 = resection of esophagojejunostomy and small bowel.
Oncological outcomes
The mean time to recurrence was 20.2 months (IQR 12.4-42.1 months). In the resectable group, 3 patients were treated by reoperation and remained alive throughout the follow-up period. A 74-year-old man who was resectable at the time of the recurrence refused to undergo repeat surgery because of his age and poor general condition. In a 52-year-old woman who was resectable, reoperation was not performed because the procedure was expected to be technically very difficult with a high risk of complications. In the unresectable group, 6 patients received chemotherapy and their median survival time was 5.4 months (IQR 2.5-9.4 months); in the remaining 6 patients, who received conservative management, the median survival time was 1.6 months (IQR 3.2-6.7 months).
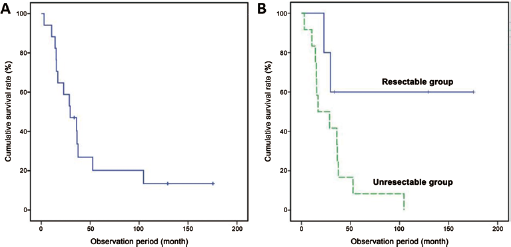
The cases of resectable and unresectable local recurrence after curative total gastrectomy are described in Table III and Table IV, respectively. Of the 17 patients, 14 died during the follow-up period. Most of these patients (13/14, 92.9%) died within the first year after the diagnosis of recurrence. The mean survival time after local recurrence was 5.2 months (95% CI 2.8-7.7 months). Figure 2A shows the survival curve of the 17 patients and Figure 2B presents the cumulative survival according to resectability.
Unresectable recurrent gastric cancer detected by esophagogastroduodenoscopy after curative total gastrectomy
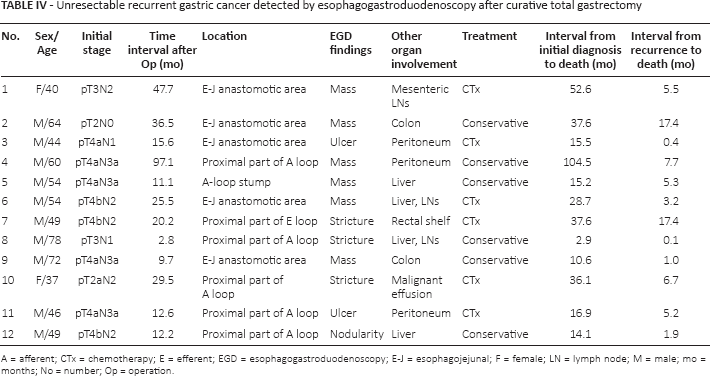
A = afferent; CTx = chemotherapy; E = efferent; EGD = esophagogastroduodenoscopy; E-J = esophagojejunal; F = female; LN = lymph node; M = male; mo = months; No = number; Op = operation.
(
Discussion
The overall survival of patients receiving curative gastrectomy remains poor and most recurrences occur within the first 5 years. The incidence of recurrence after curative gastrectomy is reported to be 22%-51% (8, 9). Recurrence can be divided into locoregional, peritoneal and hematogenous (distant) (4, 5, 10). In previous studies, the incidence of locoregional recurrence following curative resection was 25%-32% within 5 years (7, 11-12-13). After curative total gastrectomy, the rate seems to be lower at 6%-12% (7, 14, 15). Yoo and colleagues (14) reported a local recurrence rate of 6% (10/166) after total gastrectomy in a study of the long-term results of proximal and total gastrectomy for gastric adenocarcinoma. Jeong and colleagues (15) found that 6% (8/131) of patients who underwent laparoscopy-assisted total gastrectomy for gastric cancer suffered local recurrence. However, these studies did not involve endoscopy and we do not know whether the recurrent lesions would have been detectable by endoscopy. We are aware of only 1 study reporting endoscopic findings concerning local recurrence after curative total gastrectomy. Lee and colleagues (7) studied 233 patients with tumor recurrence after total gastrectomy, 47 of whom had locoregional recurrence including combined patterns of recurrence with peritoneal seeding or distant metastasis. Only 24 of these 47 lesions were accessible by endoscopy (7). This is because only a small proportion of tumor recurrences are endoscopically accessible when the tumor recurs in the inner layers of the hollow viscus.
In our study, the most frequently encountered endoscopic finding was a mass. Lee et al (7) reported that stricture, the second most common type in our study, was their most common type of recurrence. Masses and strictures, which are the more serious types of recurrence, were more frequent than ulcers or nodularities, which are usually early forms of cancer. Local recurrence after total gastrectomy usually occurs in the region proximal to the esophagojejunal junction (16). In our case, 15 (88.2%) of the tumors were in the anastomotic area or the proximal part of the jejunal loop and only 2 (11.8) were in the afferent loop stump.
Recurrence in the esophagojejunal anastomotic area after total gastrectomy can be explained by implantation of intraluminal tumor cells into the anastomosis (3). According to several reports, recurrence can occur in the jejunal stump due to spreading of cancer cells via submucosal or subserosal lymphatic vessels, or implantation of exfoliated cancer cells (16-17-18).
In the present study, endoscopically detected local recurrence had a very poor prognosis. Most cases of local tumor recurrence were combined with recurrences at other sites and curative reoperation was impossible. Furthermore, these patients died within the first year after the diagnosis of tumor recurrence, with a median survival time of as little as 5.3 months. Lee et al also reported a poor prognosis for patients with logoregional recurrence detected by endoscopy after total gastrectomy, with a mean survival time of 8 months (7). In another study of patients after curative resection for gastric cancer, patients with locoregional recurrences had a longer survival time than patients with peritoneal or hematogenous recurrences (11.0 months vs. 6.4 and 9.4 months, respectively) (4). The shorter survival time after diagnosis of recurrence in our patients compared with previous studies may be due to the fact that 3 patients (25%) of the patients who were unresectable died of acute events such as bleeding or pneumonia within 1 month of the diagnosis of recurrence, and most unresectable cases had combined peritoneal or hematogenous metastases.
Cardoso et al (8), reviewing 5 publications, concluded that detection of early recurrence can allow patients to receive palliative treatments such as chemotherapy, resulting in better outcomes. In our study, among the patients in whom recurrence was detected early, those who received surgical treatment enjoyed disease-free survival, whereas those who received chemotherapy alone had poor outcomes with short survival. Curative surgery for locally recurrent gastric cancer after total gastrectomy was rarely possible in our patients because most had combined peritoneal seeding or distant metastasis. Furthermore, reoperation after total gastrectomy is also very difficult technically due to adhesions induced by the previous surgery and the fact that the surrounding organs, diaphragm, lung, and aorta are easily injured. However, when curative surgery is possible, it offers the best chance of cure.
The main limitations of this study were its retrospective nature and the small number of cases. The latter limitation reflects the rarity of local recurrences detectible by endoscopy. Further randomized controlled trials will be needed to confirm the diagnostic effectiveness and cost-effectiveness of follow-up procedures and establish what type of follow-up schedule will improve quality of life and survival in patients after gastric cancer resection.
In conclusion, local recurrence detected by upper gastrointestinal endoscopy after curative total gastrectomy is rare and has a poor prognosis. Curative surgery is rarely possible because most patients also have distant metastases.
Footnotes
Financial support: None.
Conflict of interest: The authors have no conflicts of interest related to this work.